

Filter by mechanism, then select any disease to see the full clinical picture. Review at least one disease before continuing.
- All Diseases
- Excess water
- Water scarcity
- Warming waters

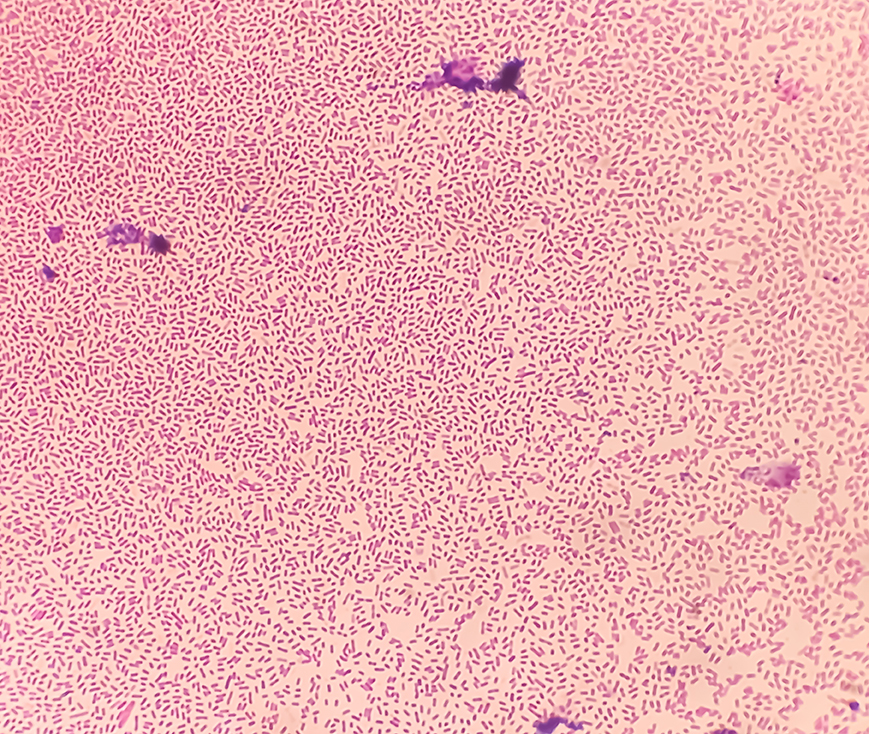
Cholera
- Pathogen: Vibrio cholerae.
- Climate mechanism: Flooding.
- Learn more about cholera.
Typhoid fever
- Pathogen: Salmonella Typhi.
- Climate mechanism: Flooding.
- Learn more about typhoid fever.
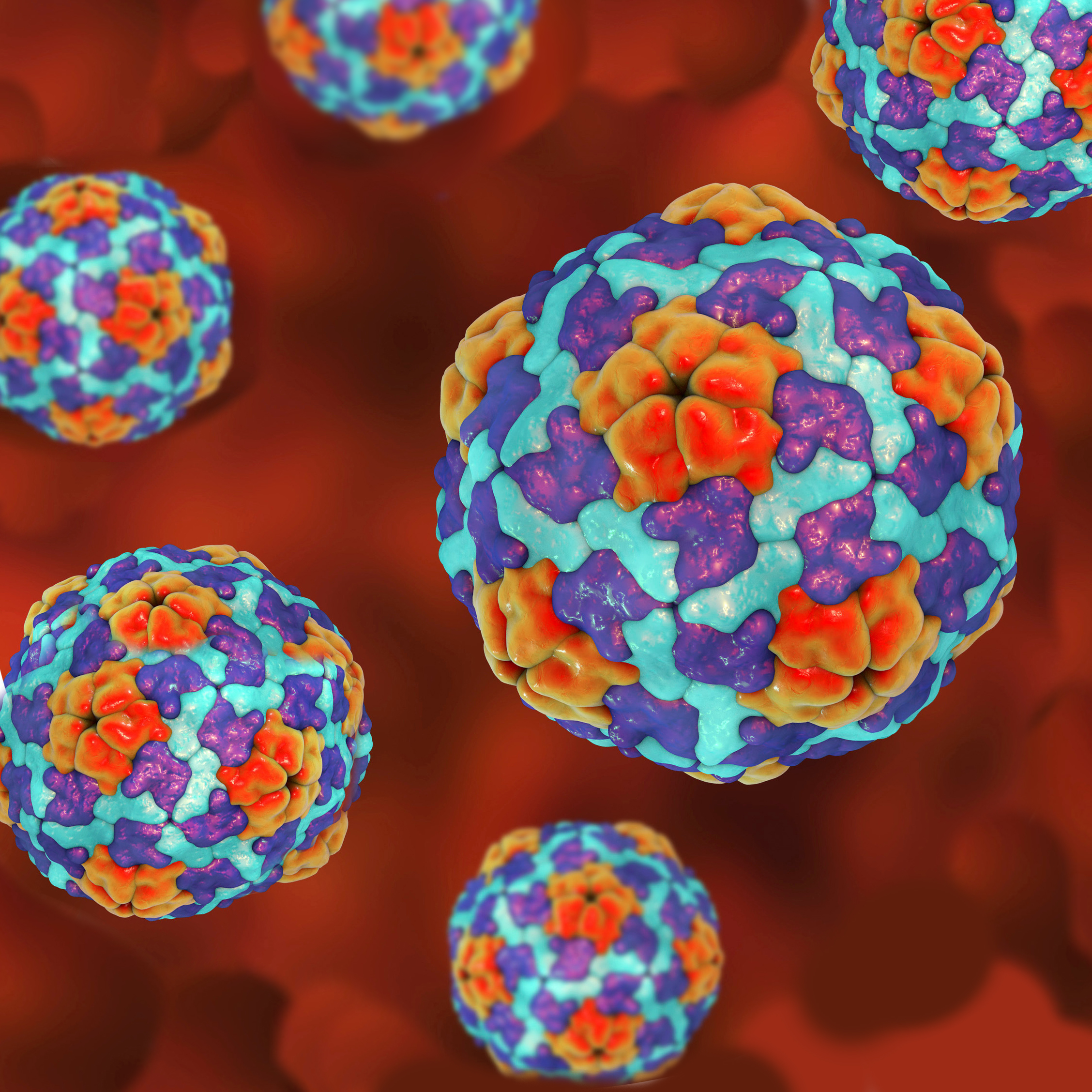
Hepatitis A
- Pathogen: Hepatitis A virus (HAV).
- Climate mechanism: Flooding.
- Learn more about hepatitis A.

Leptospirosis
- Pathogen: Leptospira spp.
- Climate mechanism: Flooding.
- Learn more about leptospirosis.
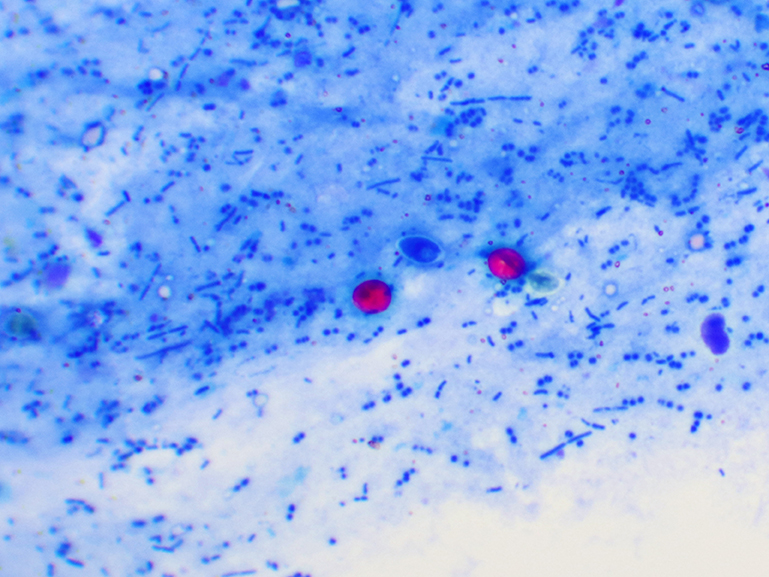
Cryptosporidiosis
- Pathogen: Cryptosporidium spp.
- Climate mechanism: Drought.
- Learn more about cryptosporidiosis.

Fluorosis + arsenicosis
- Pathogen: Chemical (non-infectious).
- Climate mechanism: Drought.
- Learn more about fluorosis and arsenicosis.

Vibrio infections
- Pathogen:
- V. parahaemolyticus.
- V. vulnificus.
- Climate mechanism: Warming.
- Learn more about vibrio infections.
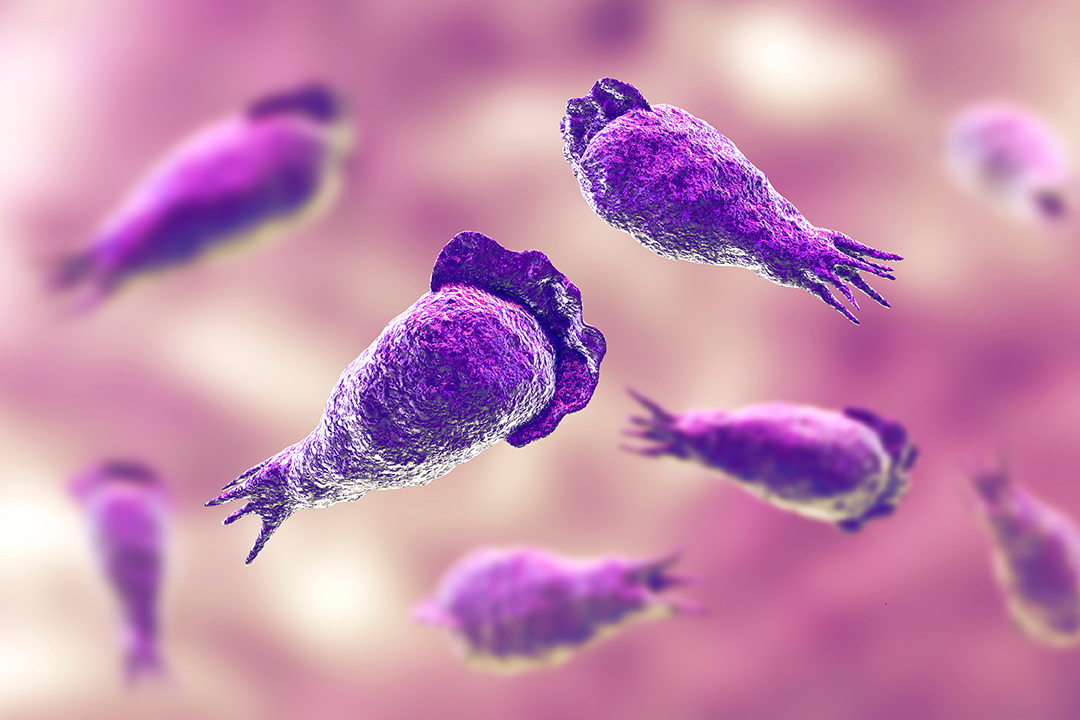
Naegleria fowleri (PAM)
- Pathogen: N. fowleri (thermophilic free-living amoeba).
- Climate mechanism: Warming.
- Learn more about N. fowleri.

Cyanotoxin poisoning
- Pathogen: Cyanobacteria (harmful algal blooms).
- Climate mechanism: Warming.
- Learn more about cyanotoxin poisoning.
Cholera
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
- Extreme precipitation.
- Flooding.
- Flooding overwhelms sanitation infrastructure.
- Fecal contamination of drinking water sources and food supply.
- Profuse rice-water diarrhea.
- Rapid dehydration.
- Electrolyte depletion.
- Potentially fatal without prompt oral or IV rehydration therapy.
- All ages.
- Highest fatality in children under 5 and elderly.
Typhoid fever
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
- Extreme precipitation.
- Flooding.
- Sewage overflow contaminates drinking water and fresh produce.
- Fecal-oral transmission predominates.
- Sustained fever.
- Relative bradycardia.
- Rose spots.
- Hepatosplenomegaly.
- Intestinal perforation in severe untreated cases.
- Children and young adults.
- Unvaccinated populations in endemic regions.
Hepatitis A
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
- Extreme precipitation.
- Flooding.
Fecal-oral transmission via flood-contaminated water and food supplies.
- Jaundice.
- Fatigue.
- Nausea.
- Dark urine.
- Pale stools.
- Elevated transaminases.
- Usually self-limiting.
- Fulminant hepatitis possible in adults.
- Unvaccinated individuals.
- Low-income urban communities.
Leptospirosis
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
- Extreme precipitation.
- Flooding.
- Contact with freshwater, mud, or soil contaminated by urine from infected animals (rodents, cattle, pigs, dogs, and wildlife).
- Leptospira enters via skin abrasions, mucous membranes, or conjunctiva.
- Most symptomatic infections present as a self-limiting febrile illness:
- Fever.
- Severe myalgia (especially calf tenderness).
- Conjunctival suffusion (redness of the eyes without discharge).
- In approximately 5–10% of cases the illness progresses to a severe form (Weil’s disease), including:
- Jaundice.
- Acute kidney injury.
- Pulmonary hemorrhage.
- The early febrile phase is shared by mild and severe disease alike, so it is the key recognition window: Identifying it allows treatment before progression to severe disease.
- Agricultural workers.
- Urban poor.
- Disaster responders.
- Frequently underdiagnosed.
- Consider in post-flood febrile illness.
Cryptosporidiosis
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
- Extreme drought.
- Water scarcity.
Water scarcity forces communities to shared, unprotected surface water sources. Cryptosporidium oocysts are resistant to standard chlorination—a critical clinical distinction.
- Profuse watery (non-bloody) diarrhea.
- Abdominal cramps.
- Nausea.
- Severe and prolonged in immunocompromised patients (HIV, transplant).
- Children under 5.
- Immunocompromised individuals.
- Communities using unprotected surface water (primarily a risk in low-income global settings where surface water is the main drought fallback, rather than in typical United States private well users).
Fluorosis + Arsenicosis
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
- Extreme drought.
- Water scarcity.
Depletion of shallow wells forces reliance on deeper groundwater that contacts fluoride- and arsenic-bearing bedrock, where these minerals naturally leach into the water supply at higher concentrations than in shallow aquifers.
- Dental and skeletal fluorosis (chronic exposure).
- Arsenicosis:
- Keratosis.
- Peripheral neuropathy.
- Elevated risk of skin, bladder, and lung cancer.
Private well users in rural New England and the Southwest face significant arsenic and fluoride exposure from naturally occurring groundwater contamination—no EPA standards apply to private wells. Patients who grew up in Southeast Asia (particularly Bangladesh, India, or Vietnam) may present years later with the consequences of past high-level arsenic exposure. In either context, think arsenicosis when you see unexplained peripheral neuropathy, keratosis, or skin hyperpigmentation.
Vibrio infections
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
Rising water temperatures.
- In warming coastal and estuarine waters, V. parahaemolyticus accumulates in filter-feeding shellfish causing gastroenteritis via ingestion.
- V. vulnificus causes wound infections and primary septicemia via contact with brackish water through broken skin.
- Gastroenteritis after shellfish ingestion (V. parahaemolyticus).
- Primary septicemia or necrotizing wound infection from seawater exposure (V. vulnificus).
- Primary septicemia CFR exceeds 50%, rising to 67% with pre-existing liver disease.
- Wound infection CFR approximately 15%.
- Coastal populations.
- Shellfish consumers.
- Individuals with liver disease or immunocompromise—highest septicemia fatality risk.
Naegleria fowleri (PAM)
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
Rising freshwater temperatures.
Thrives in freshwater above 30°C. Geographic range has expanded significantly northward; the first Minnesota case was 550 miles north of any prior documented case. Enters via nasal passages, not by drinking.
- Primary amebic meningoencephalitis (PAM):
- Headache.
- Fever.
- Nausea.
- Rapidly progressing to neck stiffness.
- Altered mental status.
- Seizures.
- Coma.
- Almost universally fatal:
- Survival rate 2.4%. Source: Fatal Case of Splash Pad–Associated Naegleria fowleri Meningoencephalitis—Pulaski County, Arkansas, September 2023. MMWR Morb Mortal Wkly.
- Clinically indistinguishable from bacterial meningitis.
- Suspect after any freshwater recreational exposure.
- Children and young adults with any recent freshwater recreational exposure.
- N. fowleri’s northward geographic range expansion—with PAM cases now documented as far north as Minnesota—means Pacific Northwest freshwater exposure is no longer outside the risk envelope.
- Consider PAM in any patient with compatible presentation and recent freshwater recreational history.
Clinical pearl
Nasal rinsing with untreated tap water is a documented, under-recognized exposure route. Splash pads and pools with inadequately disinfected water are an emerging exposure.
Cyanotoxin poisoning/harmful algal blooms (HABs)
- Climate driver
- Transmission pathway
- Clinical presentation
- At-risk populations
- Rising water temperatures.
- Drought.
Warming water temperatures expand the range and season for harmful algal blooms (HABs). Drought amplifies this: Reduced water flow creates slow-moving, nutrient-concentrated conditions that promote bloom formation—making drought a co-driver alongside rising temperatures.
- Acute:
- Nausea.
- Vomiting.
- Diarrhea.
- Hepatotoxicity (microcystins).
- Neurotoxin-producing species (anatoxin-a, saxitoxin) cause neurologic symptoms including:
- Muscle weakness and seizures.
- Skin irritation from direct water contact.
- Respiratory irritation through aerosol inhalation.
Populations using affected lakes or reservoirs for drinking water and recreation. This diagnosis is frequently missed—consider it in any patient with unexplained acute hepatotoxicity or a neurologic presentation and a history of freshwater exposure.
Mechanisms in practice
Now that you have explored the climate drivers of water-borne disease and the specific pathogens they produce. This case shows what this looks like in practice: A real community in Nepal, a real flood event, and the health system response to the diarrheal disease outbreak that followed.
Watch for:
- Which water system failure mechanism is operating.
- What the clinical burden looks like at the community level.
- How early warning systems can interrupt the exposure pathway.
Watch the video (~11 min.). Then, answer the two questions before continuing to the case study.
Question 1
The Nepal community in the video experiences a diarrheal disease outbreak following a flood event. Using the two-directions framework, identify which water system failure mechanism is responsible and explain the process connecting the flood to the outbreak
Question 2
The early warning system in the video connects environmental conditions to disease risk at the population level. How does a physician apply a similar approach when taking a history from a patient who has experienced flooding, drought, or disruption to food or water access?