In thinking about the overall architecture of the neck, it can be organized into 4 units:
1. Visceral unit
The visceral unit contains the neck’s visceral organs (the focus of this chapter). It is located anteriorly.
2. Vertebral unit
The vertebral unit is posterior; it contains the vertebral column and its associated muscles, and the spinal cord.
3–4. Vascular units
Two vascular units are located anterolaterally. These are essentially the carotid sheaths and their contents.
The viscera of the neck themselves can be further organized into three different layers:
Respiratory
Digestive
Endocrine
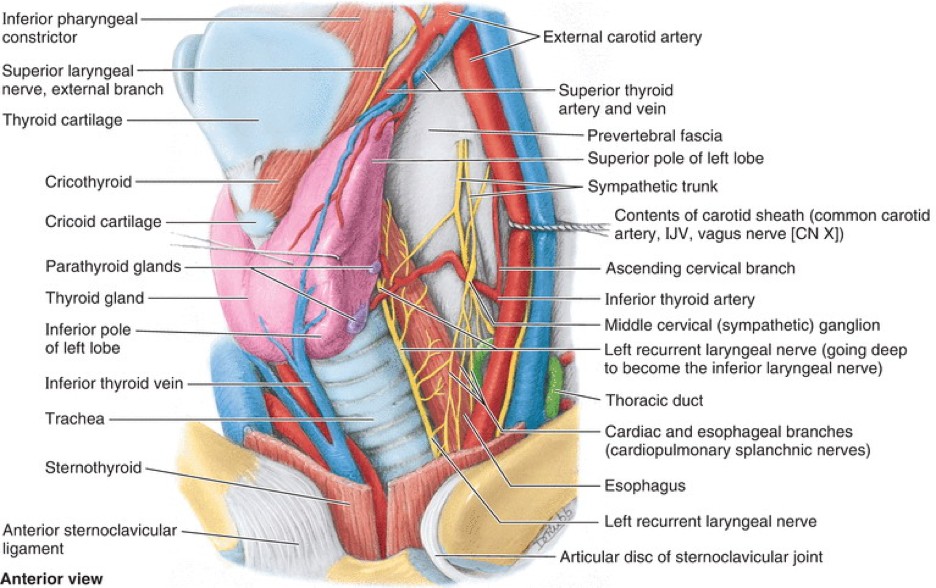
Figure 1. The visceral unit of the neck. CLINICALLY ORIENTED ANATOMY, 8TH ED., FIGURE 9.28.
Each of these layers contains two organs. This chapter provides an overview of the neck viscera, as well as a detailed description of the thyroid and parathyroid glands. All the neck viscera are covered by the pretracheal layer of deep cervical fascia and lie in the floor of the muscular triangle, deep to the infrahyoid muscles.
Respiratory layer: Larynx and trachea
Larynx
Lies between C4–6; its thyroid and cricoid cartilages can be palpated easily.
Below the thyroid cartilage, the rounded cricoid cartilage of the larynx is palpable.
The soft spot that can palpated in the midline of the neck between the thyroid and cricoid cartilages is the cricothyroid membrane. This is the site where emergency airways can be created (cricothyrotomy).
Begins at C6 just below the cricoid cartilage and passes inferiorly into the mediastinum. Its superficial location allows it to be easily palpated just above the bony suprasternal notch. The texture of the trachea is characterized by the presence of cartilage rings.
The upper part of the trachea is covered anteriorly by the isthmus of the thyroid gland.
Clinical correlation
A temporary airway can be surgically created by opening the trachea in the neck, should the normal airway route above it become obstructed or impaired. This procedure is called a tracheostomy.
It is usually performed in situations that rquire an alternate airway route for longer periods of time: for example, due to trauma, vocal cord paralysis, or if an illness requires a ventilator machine. Most tracheostomies are done in a hospital setting. Emergency tracheostomies are done but are riskier, because large blood vessels (inferior thyroid veins) overlie the trachea in the neck and in rare situations (~8% of individuals), a variant artery (thyroid ima artery) may also cross the trachea.
The pharynx (“throat”) is a muscular tube common to the respiratory and digestive tracts. It is located posterior to the nasal and oral cavities and larynx and anterior to the skull base and cervical vertebrae. It serves as both an airway and a route for ingested solid foods and liquids. The pharynx is covered in detail in The oral region and pharynx.
Paratracheal lymph nodes also lie between the trachea and esophagus.
Endocrine layer: Thyroid and parathyroid glands
Thyroid and parathyroid glands: Lie deep to the infrahyoid (strap) muscles, in the floor of the muscular triangle. A fibrous capsule derived from pretracheal fascia surrounds them.
Thyroid gland
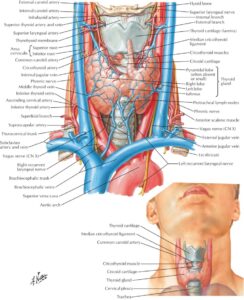
Figure 2. Thyroid gland. NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 87.
Constructed of a median isthmus and two lateral lobes. Each lateral lobe has a superior and an inferior pole.
Isthmus: Connects the two lateral lobes; lies anterior to 2nd–4th tracheal cartilage rings
Sometimes a pyramidal lobe of the thyroid projects superiorly from the isthmus in the midline of the neck. See Figure 2. This is a common variation in which thyroid tissue develops along the course of the thyroglossal duct, which is a vestige of thyroid development (covered in Head and neck development).
Rich blood supply, as would be expected for an endocrine organ. The superior thyroid arteries are the first branches of the external carotid arteries; the inferior thyroid arteries are branches from the thyrocervical trunk via the subclavian arteries. These vessels anastomose freely within the gland. The superior thyroid arteries supply the anterior part of the gland, while the inferior thyroid arteries supply the posterior side.
Thyroid ima artery: Variant (~8%); branch of thebrachiocephalic trunk, passes upward to the isthmus, superficial to the trachea.
Superior and middle thyroid veins drain to the internal jugular vein; the inferior thyroid veins drain below into the brachiocephalic veins, and overlie the trachea.
Lymph drains first to periglandular nodes near the thyroid gland (prelaryngeal, pretracheal, and paratracheal nodes). After percolating through these nodes, lymph enters the deep cervical nodes situated along the internal jugular veins.
Thyroid hormones (T3 and T4) are produced by the follicular cells of the thyroid gland. They function to control metabolism rate; Calcitonin is a hormone produced by the parafollicular (“C”) cells of the thyroid—it functions to lower blood levels of calcium. Follicular and parafollicular cells have different development histories, as we shall see.
Clinical correlation: Relationship of the Thyroid Gland and Its Arteries to the Laryngeal Nerves
During thyroid gland surgery (such as a lobectomy), surgeons carefully ligate or cauterize the thyroid arteries or their branches. Surgeons need to be aware that nerves are related to both the superior and inferior thyroid arteries, so care must be taken to avoid injuring them.
The external branch of the superior laryngeal nerve (a.k.a. = external laryngeal nerve) travels with the superior thyroid artery. If this nerve were damaged, a monotone quality to the voice could result. Why, you say? Remember that the function of the external laryngeal nerve is to innervate one (and only one) muscle = the cricothyroid muscle. Do you recall the function of this muscle? Answer: It raises vocal pitch by placing tension on the vocal folds. Without the muscle, vocal pitch is affected.
The recurrent laryngeal nerves branch from the vagus nerves in the mediastinum (on the left) and neck (on the right) and then ascend to the larynx in the tracheoesophageal grooves. As they pass behind the left and right lobes of the thyroid gland, they are crossed by the inferior thyroid arteries. You should recall that the recurrent laryngeal nerves innervate ALL of the intrinsic muscles of the larynx, except one (the cricothyroid!). These muscles affect the position of the vocal folds, so if a recurrent laryngeal nerve were damaged, a vocal fold may not be able to be placed in a position necessary for phonation, resulting in vocal hoarseness = a voice that sounds breathy or weak.
Pathologies and Congenital Defects
A goiter (from the Latin guttur, meaning “throat” or “neck”) is abnormal enlargement of the thyroid gland. Some causes are iodine deficiency or inflammation due to autoimmune disorders.
A thyroglossal duct cyst is a benign congenital anomaly that presents as a soft, mobile mass in the midline of the neck anywhere between the tongue and thyroid gland. Failure of the thyroglossal duct (a tubular remnant of thyroid gland descent during development) to obliterate can provide a potential space for cyst development. Since the duct is connected to the tongue, the cyst will move upward when the tongue is protruded.
Thyroid tumors: Benign and malignant; are fairly common.
Ectopic thyroid tissue: May be found on the posterior tongue (lingual thyroid) or below the tongue in the midline of the neck. Since the thyroid gland develops from endoderm in the floor of the pharynx near the location of the future tongue and descends through the neck down to its definitive location (leaving behind the thyroglossal duct), ectopic tissue could form along this pathway. More discussion of this in Head and neck development.
Parathyroid glands
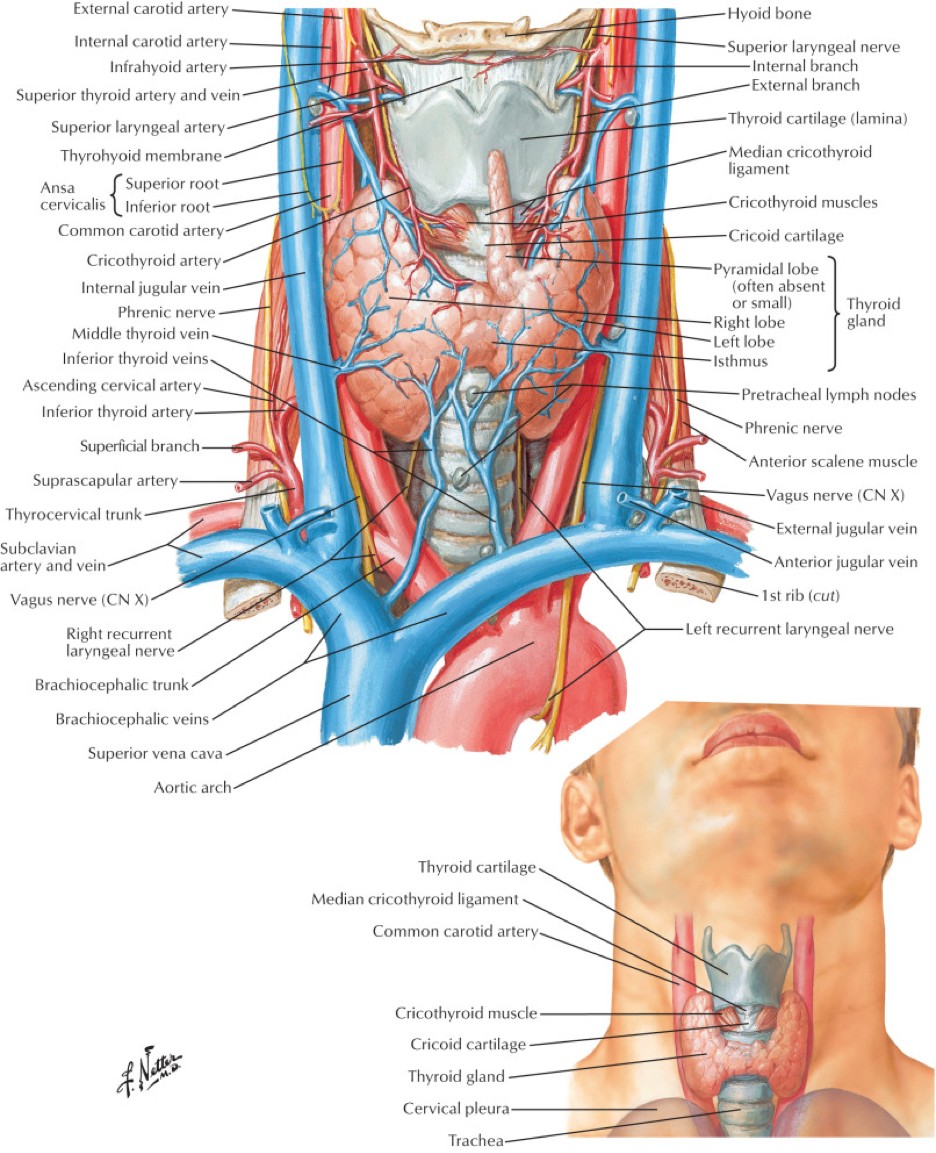
Figure 3. Relationships of thyroid and parathyroid glands, inferior thyroid artery, and recurrent laryngeal nerve. NETTER, ATLAS OF HUMAN ANATOMY,7TH ED., PLATE 89.
Reddish-brown in color, usually four in number (left and right, superior and inferior), and about the size of a lentil. Their location is often said to be in the capsule on the posterior side of the thyroid gland—however, ectopic locations are common, ranging from the carotid bifurcation superiorly to the mediastinum inferiorly.
They produce parathyroid hormone (parathormone), which functions to elevate the levels of blood calcium (by stimulating osteoclast activity in bone), helps to regulate serum phosphate levels, and promotes vitamin D synthesis.
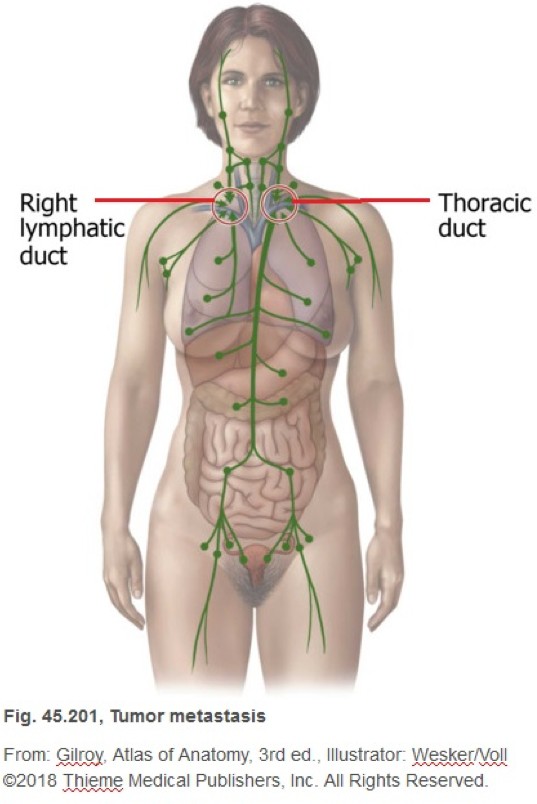
Figure 4. Lymph from the entire body drains to the left and right jugulosubclavian junctions (a.k.a. left and right venous angles)—indicated by the red circles. Stomach carcinoma may metastasize to the left supraclavicular lymph nodes. Systemic lymphomas may also spread to deep cervical lymph nodes by this pathway.
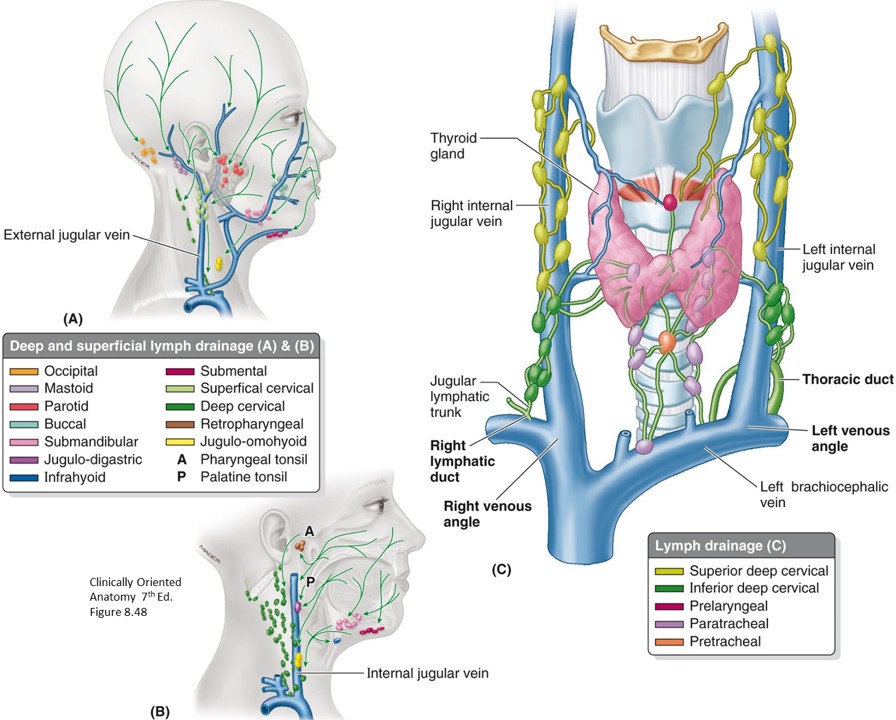
Lymph from the entire head and neck ultimately drains to the deep cervical nodes. Another way of saying this is that the deep cervical notes receive the terminal lymphatic drainage of the head and neck. These nodes lie on the carotid sheaths, closely associated with the internal jugular veins. Lymph from the deep cervical nodes enters the left and right jugular lymph trunks. These may join the subclavian or internal jugular veins independently, or they may join the right lymph duct on the right side, and the thoracic duct on the left side, which drain to the left and right venous angles (jugulosubclavian junctions).
Peripheral nodes
The deep cervical nodes receive lymph from peripheral (outlying) nodes in the head and neck. The peripheral nodes in the neck can be roughly organized into superficial and deep groups.
Superficial group of peripheral nodes
Collect lymph from the superficial fascia and skin of the neck.
Anterior jugular nodes and external jugular nodes, located along the veins of the same name. Lymph from these nodes is then passed to deep cervical nodes.
Deep group of peripheral nodes
Collects lymph from tissues DEEP to the investing layer of deep fascia. These are the paratracheal, pretracheal, and retropharyngeal lymph nodes. Lymph from these nodes is then passed to deep cervical nodes.
Deep cervical nodes
The deep cervical nodes themselves are divided into a superior group and an inferior group.
Superior deep cervical nodes
Lie along the internal jugular veins, superior to the omohyoid muscles. One of the largest of the superior deep cervical nodes receives a special name:
Jugulodigastric node: Located where the posterior belly of digastric crosses the internal jugular vein; large node that receives drainage from the palatine tonsil, and is often enlarged in tonsillitis (the “tonsillar node”); also receives lymphatic drainage from the posterior one-third of the tongue.
Inferior deep cervical nodes
Located along the internal jugular vein at the level of and below where it is crossed by the omohyoid muscle.
Jugulo-omohyoid node: Large deep cervical node that receives most of the lymph drainage from the anterior part of the tongue and oral cavity (from submental and submandibular lymph nodes draining the lips, chin, and tongue).
Supraclavicular nodes: The most inferior group of inferior deep cervical nodes. These nodes are located near the left and right venous angles.
The deep cervical nodes are clinically important nodes because they are connected to the large lymph ducts at the root of the neck via small communicating lymphatic channels. Lymph in these ducts (thoracic duct on the left, right lymph duct on the right), which originates from large areas of the body, could percolate backwards through lymph channels into supraclavicular nodes, and it is therefore possible that cancer cells from distant organs could wind up in nodes at the base of the neck.
Clinical correlation
Supraclavicular lymphadenopathy is usually a bad sign. These nodes are classified as “signal nodes” or “sentinel nodes” because they are nodes to which cancer cells likely spread from primary tumors. Clinicians call enlarged supraclavicular nodes “Virchow’s nodes.”
Enlarged supraclavicular nodes on the left side may indicate that cancer cells have metastasized from a primary tumor in the abdomen, oftentimes stomach carcinoma. Enlarged supraclavicular nodes on the right side often are indicative of lung carcinoma.
Figure 5.
Nice to know, but not need to know
Surgeons have devised schemes for organizing the head and neck lymph nodes into regions or “levels.” Infectious agents and tumor cells from certain regions of the head and neck (and even distant regions of the body) predictably migrate to nodes in particular levels.