PhD · Clinical Assistant Professor, Department of Translational Medicine & Physiology
Office: PBS 41C
Table of Contents
Optional reading
Langman’s Medical Embryology: Chapter 17, Head and Neck. The relevant sections are: Introduction, Pharyngeal Apparatus, Thyroid Gland, and Face.
Most of the events that produce the definitive anatomy of the head and neck are covered in this chapter. The pharyngeal apparatus (the source of the primordial tissues) is discussed first, followed by detailed discussions of the development of the face and thyroid gland. The development of other head and neck organs are discussed with their gross anatomy in later chapters.
The pharyngeal apparatus
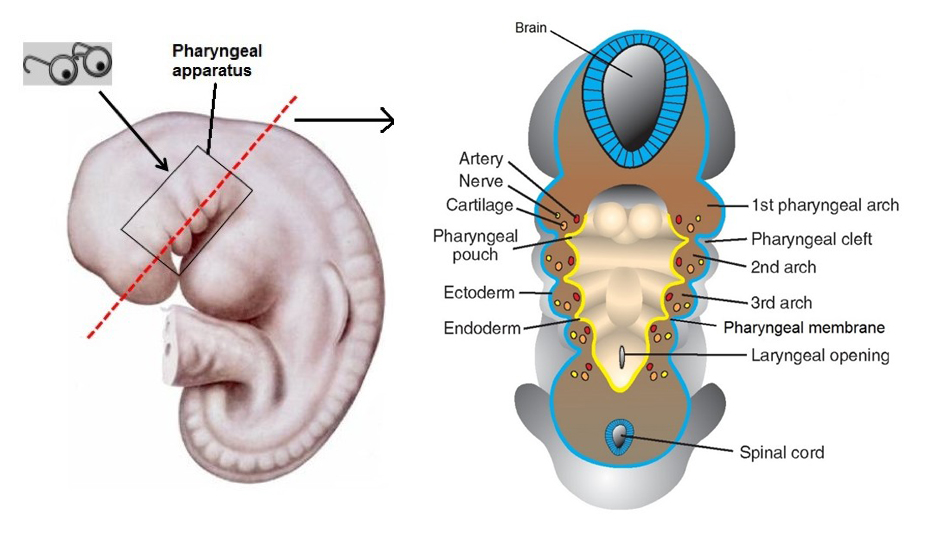
Figure 1. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 17.6.
Beginning in Week 4, the basic tissues of development in the cranial region of the embryo become organized into the pharyngeal apparatus, formerly called the branchial apparatus, since it resembles gill slits in fish. It is the forerunner of head and neck structures.
The pharyngeal apparatus is constructed of four components:
Pharyngeal arches
Pharyngeal pouches
Pharyngeal clefts
Pharyngeal membranes
Most congenital anomalies in the head and neck region result from faulty transformation of the pharyngeal apparatus into adult structures.
Composition of a pharyngeal arch
The pharyngeal arches support the lateral walls of the pharynx (the upper part of the foregut).
Human embryos have five pairs of discernable arches, numbered one, two, three, four, and six. The fifth arch in humans either does not develop or is rudimentary and quickly regresses. The sixth arches cannot be seen externally.
Similar to other tissues in the embryo, the pharyngeal arches develop in a cranial to caudal sequence, with the upper arches appearing earlier. The arches are separated externally by pharyngeal clefts and internally by pharyngeal pouches.
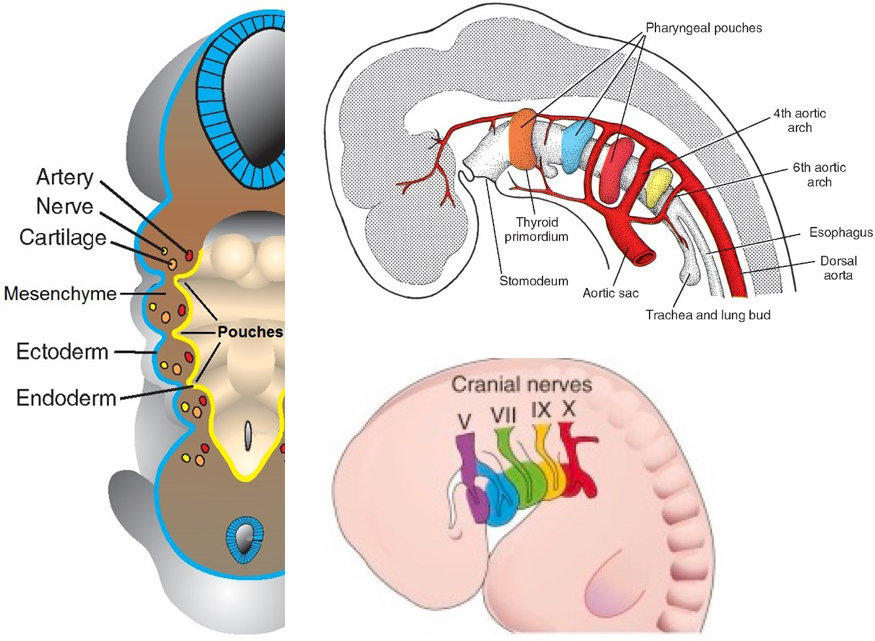
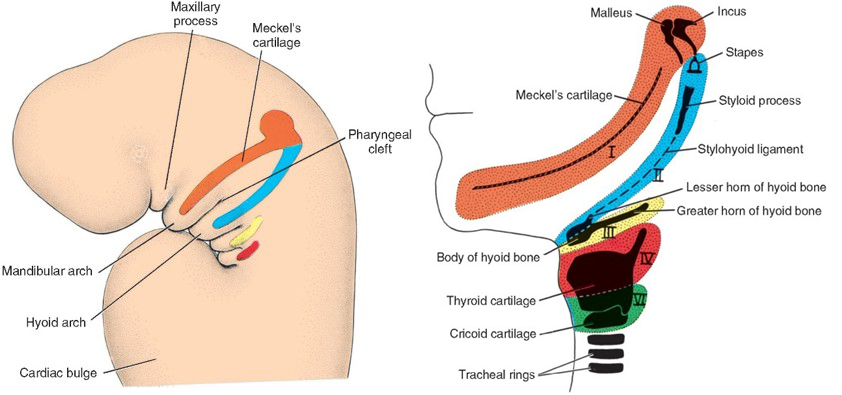
Figure 2. Composition of pharyngeal arch, with cranial nerves and aortic arch arteries. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURES 17.4, 17.6, AND 17.7.
Each arch is composed of these tissues:
Mesenchyme derived from paraxial mesoderm: Gives rise to skeletal muscles.
Neural crest, which migrates from the region of the developing brain: Gives rise to skeletal structures and connective tissues.
A cartilage bar made from neural crest—this is a temporary structure thought to give initial support to the pharyngeal arch: Later it is transformed into other structures (often bone, adult cartilage, or ligament).
External layer of ectoderm.
Internal layer of endoderm.
A cranial nerve (or cranial nerve branch).
An artery (derived from the aortic arches—these were introduced with heart development).
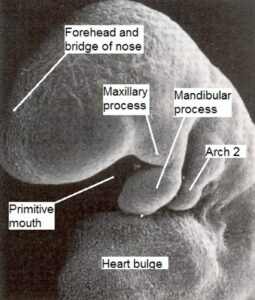
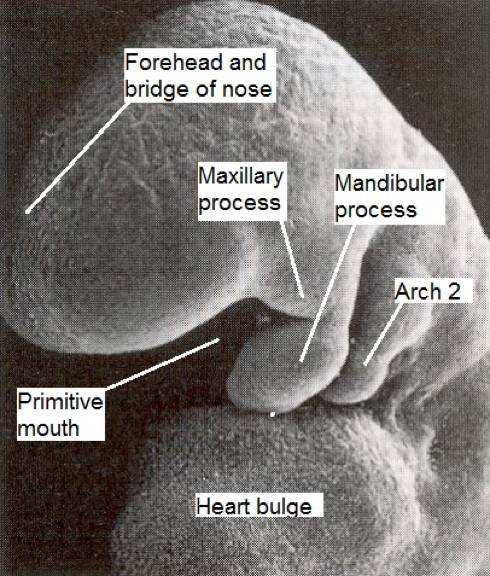
Subdivides into a cranial maxillary process and a caudal mandibular process. These produce the upper and lower jaws, respectively.
Neural crest condenses to form the transient cartilage of the maxillary process and cartilage of the mandibular process (Meckel’s cartilage). From these cartilages develop the incus and malleus—bones of the middle ear.
Mesenchyme from neural crest forms the substrate for facial bones that develop via intramembranous ossification = maxillae, mandible, zygomatic bones, and the squamous part of the temporal bones. Maldevelopment of the first arch can produce facial abnormalities.
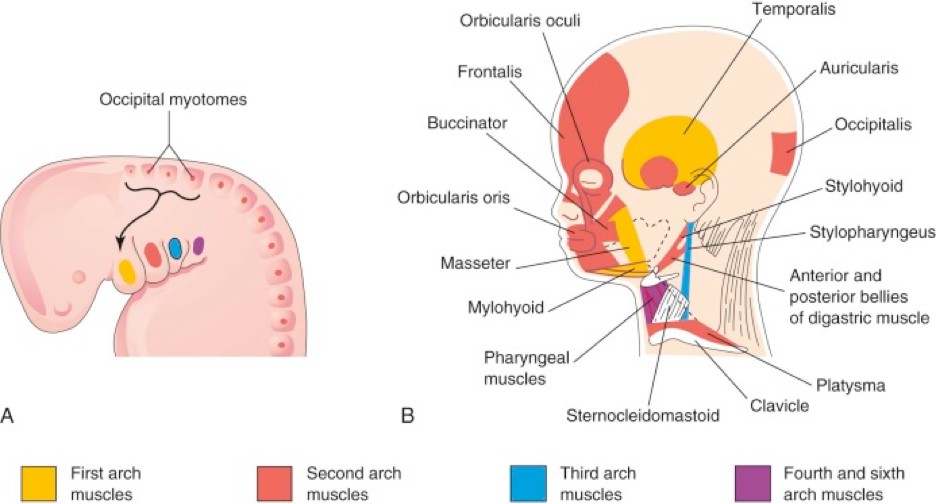
Mesenchyme from paraxial mesoderm gives rise to muscles associated with the first arch = mastication muscles (temporalis, masseter, medial and lateral pterygoid) as well as the mylohyoid, anterior belly of the digastric muscle, the tensor tympani (middle ear) and tensor veli palatini (soft palate).
The cranial nerve associated with the first arch is the trigeminal (cranial nerve V)—but only its maxillary and mandibular divisions (V2and V3).
The first aortic arch artery regresses as the first pharyngeal arch develops. It probably only contributes to a small portion of the definitive maxillary artery.
Figure 3.
Neural crest cells form the cartilage of the second arch (Reichert’s cartilage). From the cartilage develops the stapes (middle ear), the styloid process of the temporal bone, the stylohyoid ligament, and the lesser horns and upper part of the body of the hyoid bone.
Mesenchyme from paraxial mesoderm of the second pharyngeal arch migrates across the developing face to form mimetic muscles (muscles of facial expression), as well as the posterior belly of the digastric and stylohyoid muscles in the neck, and the stapedius muscle (in the middle ear).
The cranial nerve of the second arch is the facial nerve (cranial nerve VII).
The second aortic arch artery regresses as the second pharyngeal arch develops. Its only vestige is the small stapedial artery of the middle ear.
Neural crest of the third arch produces the cartilage of the third arch. From this cartilage develops the greaterhorn and the lowerpartofthebodyofthehyoid bone. Thus, the hyoid bone is a composite structure built from two pharyngeal arches.
Mesenchyme from paraxial mesoderm of the third arch produces only the stylopharyngeus muscle of the pharynx.
The cranial nerve associated with the third arch is the glossopharyngeal nerve (cranial nerve IX).
As described when we studied the development of the heart, the third aortic arch arteries give rise to the major arteries of the head: left and right common carotid arteries and the proximal portions of the internal carotid arteries.
These arches are usually considered together since they combine to give rise to the larynx. Some sources claim that a true separate sixth arch does not exist.
The cartilages of the larynx are formed from the embryonic cartilages of the fourth and sixth pharyngeal arches. There is debate among embryologists concerning the source of mesenchyme for these cartilages. Some authors claim neural crest, while others suggest lateral mesoderm from the trilaminar disc is the source. Most authors do agree that the epiglottic cartilage develops much later than the other laryngeal cartilages, perhaps as late as the 5th month.
Mesenchyme from paraxial mesoderm of the 4th and 6th arches givesrise to its muscles: pharyngeal constrictor muscles (superior, middle, and inferior), intrinsic muscles of the larynx (muscles of phonation = produce sound), the levator veli palatini (soft palate), and the palatoglossus muscles (associated with tongue and soft palate).
The vagus nerves (cranial nerve X) innervate the fourth and sixth arches. More precisely, the superior laryngeal nerves supply the fourth arches, while the recurrent laryngeal nerves supply the sixth arches.
The fourth and sixth aortic arch arteries give rise to arteries in the thorax. From the right fourth aortic arch comes the proximal part of the right subclavian artery while the left contributes to the development of the arch of the aorta. The sixth aortic arches give rise to the proximal portions of the pulmonary arteries as well as the embryonic ductus arteriosus.
Figure 4. Summary: Derivatives of arch cartilages. LANGMAN’ S MEDICAL EMBRYOLOGY, FIGURES 17.8 AND 17.9.
Figure 5. Summary: Muscular derivatives of pharyngeal arches. THE DEVELOPING HUMAN, FIGURE 9-5.
How does the smooth contour of the neck result?
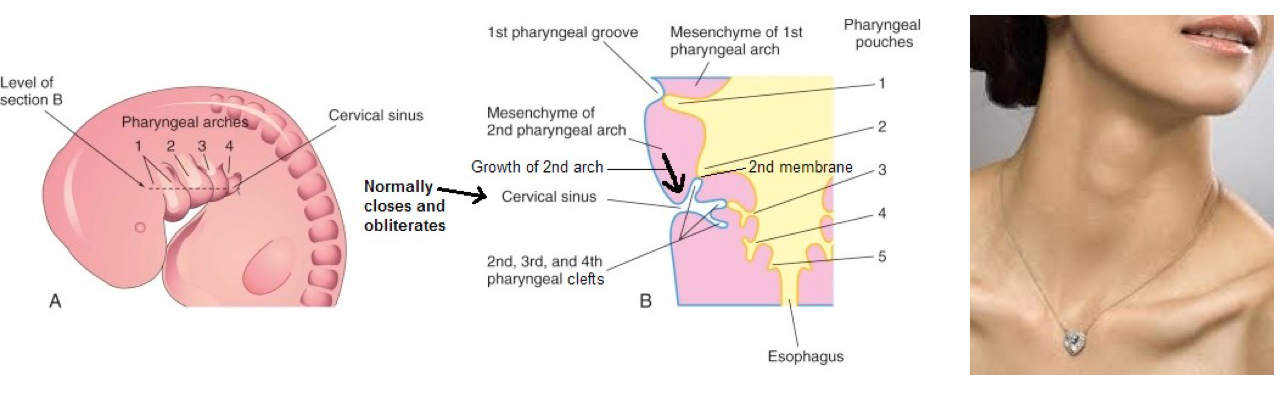
Figure 6. Growth of 2nd arch caudally provides for a smooth lateral neck contour. THE DEVELOPING HUMAN, FIGURE 9-9.
As you might have noticed, fully developed humans don’t have swellings in their necks with clefts between them. How is the pharyngeal apparatus transformed to produce the aesthetically pleasing transition between head and shoulders?
During the fifth week, the second arches enlarge and migrate caudally, overgrowing the third and fourth arches. The second arches fuse with the tissues of the upper thorax.
This process covers up and internalizes the second, third, and fourth pharyngeal clefts. Subsequently the three clefts fuse to form bilateral potential spaces in the developing neck called cervical sinuses. Normally the cervical sinuses collapse and are obliterated.
Clinical correlation
In some cases, normal neck development goes awry:
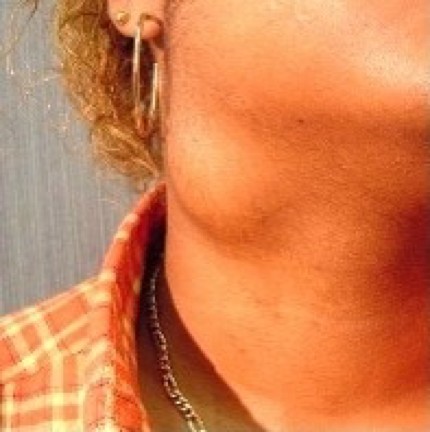
Figure 7. Lateral cervical cyst.
Lateral cervical cysts (a.k.a. branchial cysts) are fluid- or debris-filled masses that develop from persistent cervical sinuses. These presentin the neck along the anterior border of thesternocleidomastoid muscle.
Find a mass along the anterior border of the SCM in the neck of a youngster or pre-teen? Think lateral cervical cyst.
Branchialsinuses are small canals that open onto the lateral neck along the anterior border of the sternocleidomastoid (externalbranchial sinus) or into the pharynx near the tonsillar fossa (internal branchial sinus). These result from incomplete closure of the cervical sinus laterally as the 2nd arch grows caudally over the 3rd and 4th arches (external sinus) or rupture of the second pharyngeal membrane (internal sinus). If the sinus connects internally to a lateral cervical cyst, the sinus may “weep” fluid onto the neck surface.
A branchial fistula is a rare tract or small canal that has two openings: one external and one internal. The external opening is usually along the anterior border of the sternocleidomastoid and the internal opening is near the tonsillar fossa.
A fistula has two openings, a sinus has one opening, and a cyst is a closed sac containing a liquid or semisolid material without any openings.
Pharyngeal pouches
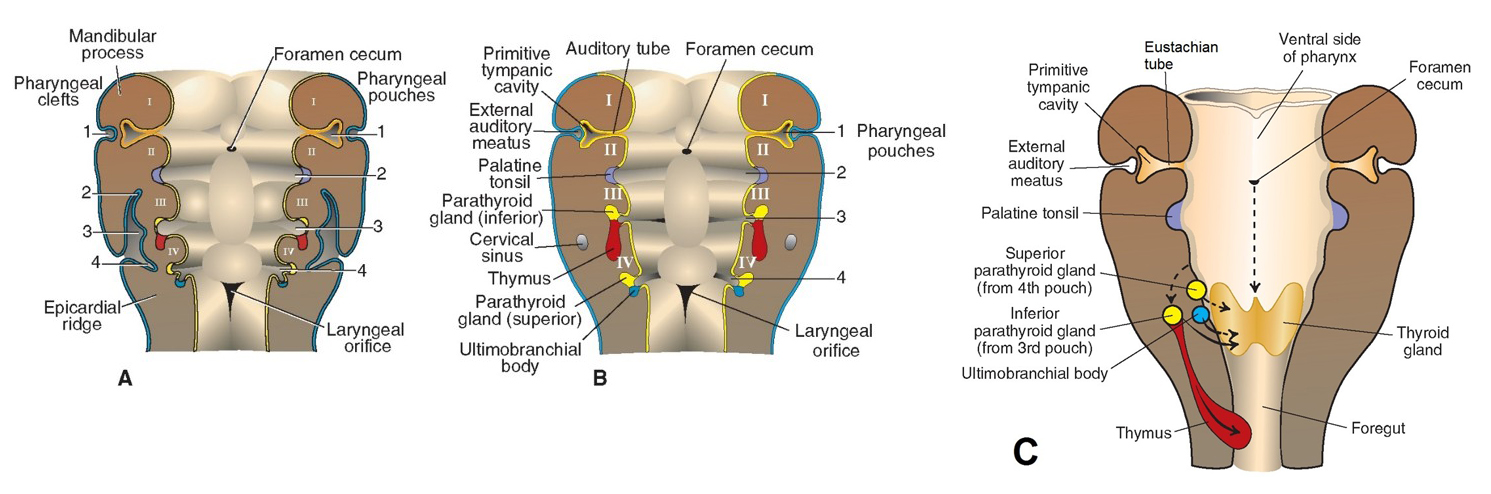
Figure 8. Fates of pharyngeal pouches. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURES 17.10 AND 17.11.
The endoderm of the pharynx lines the internal aspect of the pharyngeal arches and forms a series of diverticula that protrude outward between the arches. These are the pharyngeal pouches.
The pouches internally and clefts externally are separated by the pharyngeal membranes.
Four pouches develop, numbered from cranial to caudal: first, second, third, and fourth.
The third and fourth pouches each develop dorsal and ventral processes.
The pouches grow and expand away from the pharynx. The first and second pouches retain their internal connections to the pharynx, while the third and fourth pouches detach and form structures distant from the pharynx.
Figure 9. Adult derivatives of pharyngeal pouches. THE DEVELOPING HUMAN, FIGURE 9-8.
Pharyngeal pouch
Definitive structures
First
Tympanic cavity and Pharyngotympanic (Eustachian) tube Note that the proximal opening of the Eustachian tube is in the nasopharynx, while distally it opens into the tympanic cavity (middle ear cavity) in the temporal bone. The tympanic cavity develops from the distal part of the first pouch, while the Eustachian tube is its proximal part.
Second
Tonsillarfossa
Later, mesenchyme invades the fossa to form the palatine tonsil. The tonsillar fossa is in the lateral wall of the oropharynx.
Third
Dorsal process = Inferior parathyroid gland
Ventral process = Thymus
Fourth
Dorsal process = Superior parathyroid gland
Ventral process = Parafollicular cells (C-cells) of thyroid gland The ventral process of the fourth pouch is often referred to as the ultimobranchial body. Some embryologists claim it to be a 5th pouch instead (ultimo translates to “last”, so it is the last pouch to form and that makes it the caudal-most pouch). Regardless of its classification, it gives rise to the parafollicular cells, which make the hormone calcitonin.
The paradox of the parathyroid glands
Ponder this: Why is it that the definitive inferior parathyroid glands (which are caudal to the superior parathyroid glands after development is completed) come from the 3rd pharyngeal pouches, which are cranial to the 4th pouches in the embryo (and give rise to the superior parathyroid glands)?
Recall that the endoderm of the 3rd pouches also gives rise to the thymus, an organ of the thorax. The descent of the 3rd pouch caudally toward the thorax apparently carries the future inferior parathyroid glands below the level of the 4th pouch endoderm (future superior parathyroid glands), flip-flopping their before-and-after development locations.
Clinical correlation
Although classic descriptions of the parathyroid glands have them located directly posterior to the thyroid gland, the developmental migration of the 3rd and 4th pouches guarantees that ectopic locations are common place. Some resources report ectopic parathyroids in 20% of patients.
Common ectopic locations reported include the tracheoesophageal grooves in the neck for superior parathyroid glands, while the inferior parathyroids can often be found in the superior mediastinum near the thymus. Surgeons treating patients with tumors of the parathyroid glands (one possible cause of hyperparathyroidism) need to be aware of these variations.
Pharyngeal clefts
The first pharyngeal clefts give rise to the external acoustic meatuses. These transmit sound waves into the head. The second,third, and fourth pharyngeal clefts are overgrown by the second pharyngeal arch when the smooth neck forms. Subsequently, they fuse to form the cervical sinus (discussed earlier), a potential space that normally obliterates later in development.
Pharyngeal membranes
The membranes are located where ectoderm-lined pharyngeal clefts are adjacent to the endoderm-lined pharyngeal pouches. Normally there is a layer of mesoderm interposed between the cleft and pouch, making the membrane a trilaminar structure.
The first pair of pharyngeal membranes gives rise to the tympanic membranes (eardrums).
Obliteration of the 2nd, 3rd, and 4th clefts along with growth and migration of the 3rd and 4th pouches eliminates the other pharyngeal membranes = they do not form any definitive adult structures.
Hint: Don’t overlook this short chapter
Since many head and neck defects are due to faulty development of the pharyngeal apparatus, Boards exams usually include questions on this topic!
Development of the face and parotid gland
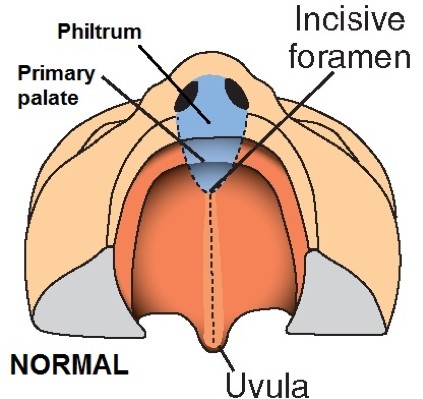
Figure 10. Normal development of lip and palate. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 17.28.
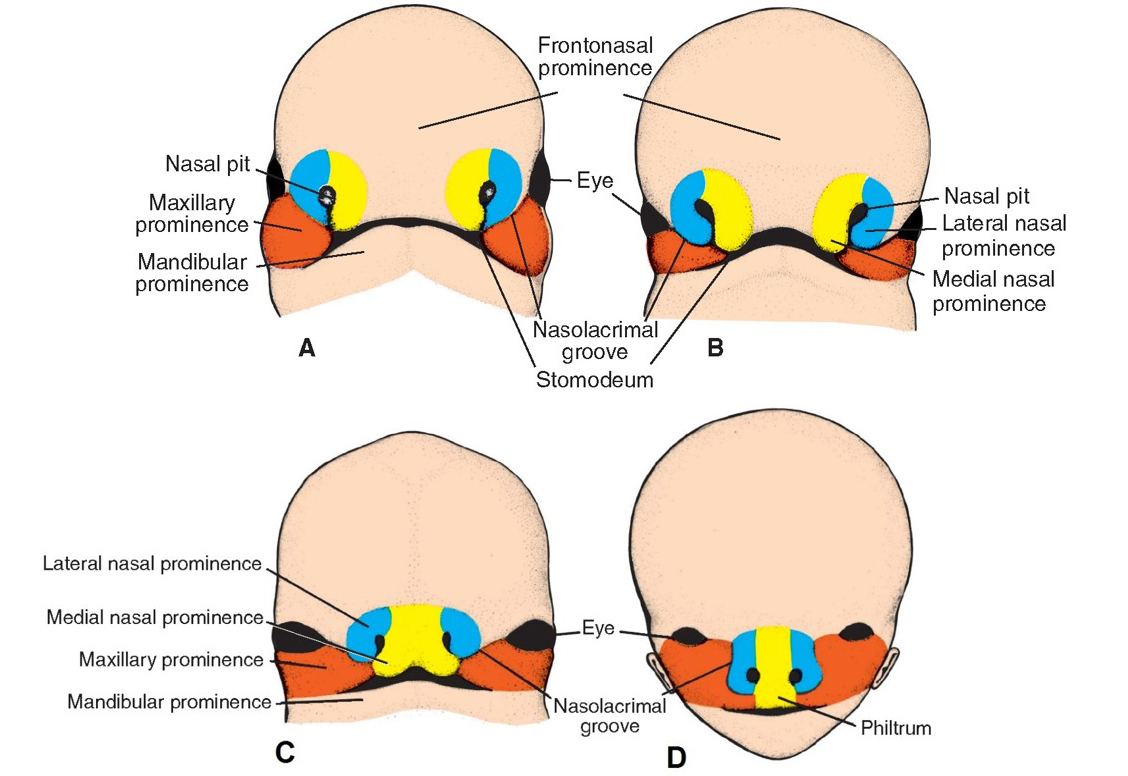
The face develops from five ectoderm-covered and mesenchyme-filled primordial structures: a single frontonasal prominence and left and right maxillary and mandibular prominences. These grow and converge around the primitive mouth (stomodeum).
Frontonasal prominence: Develops cranial to the developing brain. The embryonic head fold brings it down in the center of the developing face. The ophthalmic division of trigeminal (V1) innervates it.
At the caudal end of the frontonasal prominence, ectoderm invaginates to form left and right nasal pits. Mesenchyme in the frontonasal prominence piles up around the pits to form medial and lateral nasal prominences. (See Figure 11: Medial nasal prominences are yellow; lateral nasal prominences are blue).
The medial nasal prominences fuse. The upper portion of the fused medial nasal prominences forms the dorsum (bridge) of the nose and the nasal septum. The lower portion of the fused medial nasal prominences forms what is called the intermaxillary segment. The intermaxillary segment gives rise to the philtrum of the upper lip and the primary palate = the triangular region of the palate anterior to the incisive foramen, which includes the upper incisor teeth. See Figure 10.
Summary of the parts of the face/head derived from the frontonasal prominence (see Figure 11):
Forehead
Upper eyelids
Nose and nostrils (dorsum of nose and nasal septum from medial nasal prominences, alae of nose from lateral nasal prominences)
Philtrum of upper lip
Upper incisor teeth
Primary palate (all from the intermaxillary segment).
Maxillary prominences develop from the first pharyngeal arch. They give rise to the upper jaw and are innervated by the maxillary nerve (V2).
Fusion of the maxillary prominences with the lateral nasal prominences gives a smooth transition from the side of the nose to the cheek.
Fusion of the maxillary prominences with the intermaxillary segment completes the upper lip.
Mandibular prominences also develop from the first arch and are innervated by the mandibular nerve (V3). They give rise to the lower jaw. They fuse below the mouth to complete the lower lip and chin.
The parotid gland is formed by invagination of facial ectoderm in the cleft between the maxillary and mandibular prominences. The ectoderm pinches off from the surface of the face, but maintains a connection (future parotid duct) to the angle of the wide embryonic mouth. As the mouth size is reduced, the duct loses it connection to the angle of the mouth, but retains its connection to the oral cavity, now opening opposite the 2nd upper molar.
Figure 11. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURES 17.22 AND 17.23.
Clinical correlation: Congenital defects of the face
Incomplete or partial fusion of the facial prominences results in facial clefts. These are the most common craniofacial anomalies.
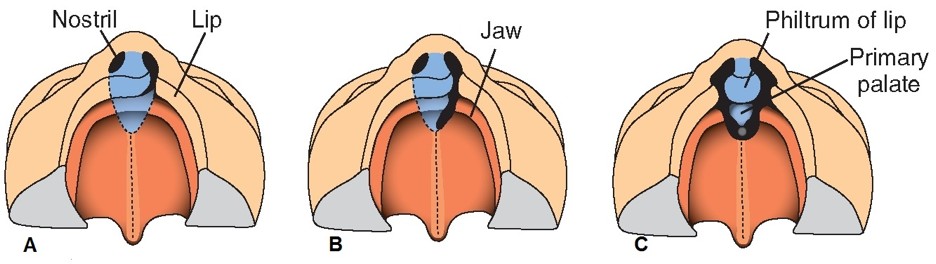
Figure 12. A: Unilateral cleft of lip
B: Unilateral cleft of lip and anterior palate
C: Bilateral cleft of lip and anterior palate.
LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 17.28.
Cleft lip is the most common facial cleft. It is caused by failure of the maxillary prominences to fuse properly with the intermaxillary segment (fused medial nasal prominences) along the edge of the philtrum. Underdevelopment of mesenchyme due to deficiencies in neural crestcell migration and proliferation is thought to be the reason. The degree of clefting is variable—from small notches in the border of the lip to complete separation of the lip and underlying bone.
Underdevelopment of the first pharyngeal arch can lead to varied malformations of the face. First arch syndrome is a collection of genetic malformations involving derivatives of the maxillary and mandibular prominences. These may include underdevelopment of the mandible or zygomatic bones, enlargement of the mouth, and malformations of the eyelids, ears, or palate. It appears that a failure of proliferation of neural crest cells may be the underlying factor. Treacher Collins syndrome is a well-known manifestation of first arch syndrome.
Development of the thyroid gland
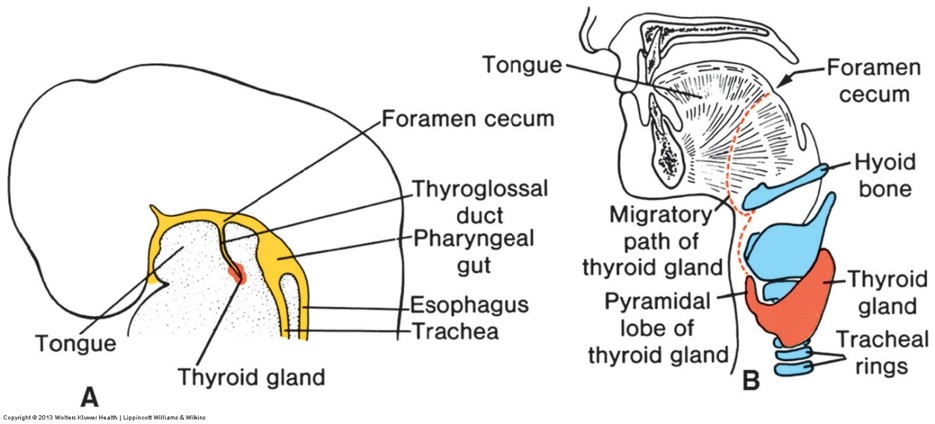
Figure 13. LANGMAN’S MEDICAL EMBRYOLOGY, 12TH ED., FIGURE 17.18.
The butterfly-shaped thyroid gland is the first endocrine gland to develop—starting in Week 4. It functions in the fetus. The thyroid develops from three embryonic primordia.
The median thyroid primordium originates as a diverticulum of endoderm that grows caudally in the midline from the floor of the primitive pharynx. It is not part of the pharyngeal apparatus (described earlier). As it grows caudally in the neck it acquires a bi-lobed morphology. By the 7th week of development, it has descended in front of the hyoid bone and future larynx to its final position anterior to the trachea. After descent, it remains connected to the floor of the pharynx by a collapsed tube of endoderm called the thyroglossal duct. After the tongue develops in the floor of the mouth, the proximal opening of the thyroglossal duct within the oral cavity is indicated by the foramen cecum on the dorsal surface of the tongue. The follicles of the thyroid gland (that produce thyroid hormones) develop from the median thyroid primordium.
Left and right lateral thyroid primordia develop from endoderm (and possibly neural crest) of the ultimobranchial body = the ventral part of the 4th pharyngeal pouch. These primordia migrate medially in the neck and join the median thyroid primordium to complete the thyroid gland. The parafollicular (“C”) cells and connective tissues (stroma) of the thyroid gland develop from the lateral thyroid primordia.
Clinical correlation
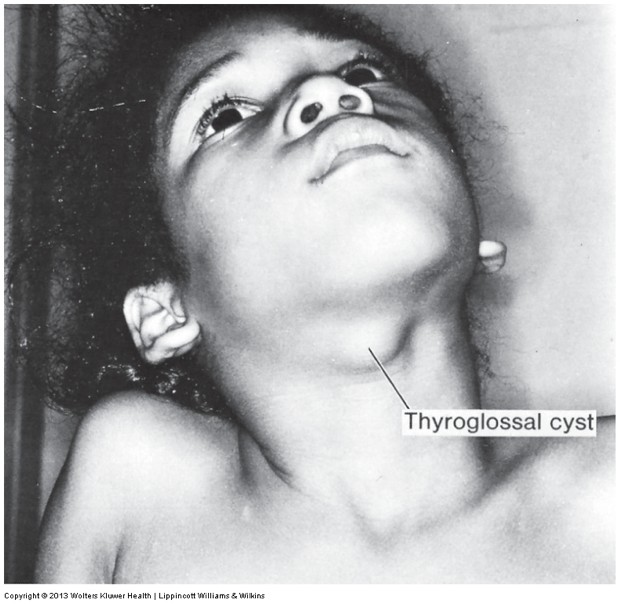
Figure 14. LANGMAN’S MEDICAL EMBRYOLOGY, 12TH ED., FIGURE 17.20.
The thyroglossal duct normally closes and atrophies. If it doesn’t, it provides a potential space for a cyst to develop within. Thyroglossal duct cysts can occur anywhere along the route of the thyroglossal duct – but most occur near the hyoid bone.They account for up to 70% of congenital neck masses. They present as round, painless swellings in the midline of the anterior neck and classically elevate when the tongue is protruded. When infected they become red, painful lumps. Thyroglossal duct cysts are removed by surgical excision of the cyst, the thyroglossal duct tract, and the central portion of the hyoid bone (this is called the Sistrunk procedure). This somewhat radical procedure greatly reduces the likelihood that the cyst will recur.
When diagnosing a thyroglossal duct cyst is important to rule out another diagnosis = ectopic thyroid. Ectopic thyroid tissue can be found anywhere along the course of the thyroglossal duct. Thyroid tissue occurring near the foramen cecum of the tongue is known as a lingual thyroid. Accessory thyroid tissue that projects upwards from the isthmus of the thyroid is a common variation—this tissue is known as a pyramidal lobe of the thyroid gland. Ectopic thyroid is histologically and functionally normal thyroid tissue.
Chapter summary
After studying this chapter, you should be able to describe the development/ tissue sources of these structures:
Muscles of mastication
Muscles of facial expression
Stylopharyngeus muscle
Muscles of the larynx and pharynx
Muscles of the soft palate
Muscles in the tympanic cavity
Mylohyoid and digastric muscles
Bones of the upper jaw
Bones of the lower jaw
Auditory ossicles
Styloid process
Hyoid bone
Common carotid arteries
Ductus arteriosus
External acoustic meatus
Pharyngotympanic (Eustachian) tube
Tympanic cavity
Tympanic membrane
Tonsillar fossa
Parathyroid glands
Thyroid gland (follicular and parafollicular cells)