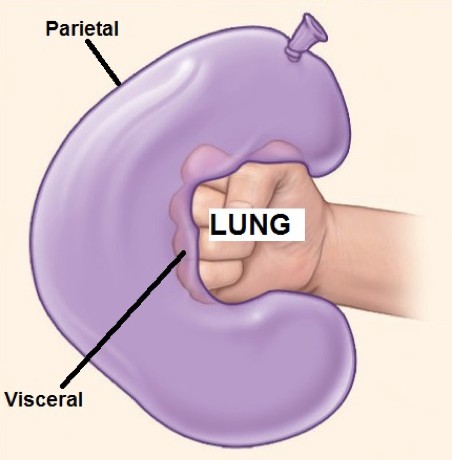
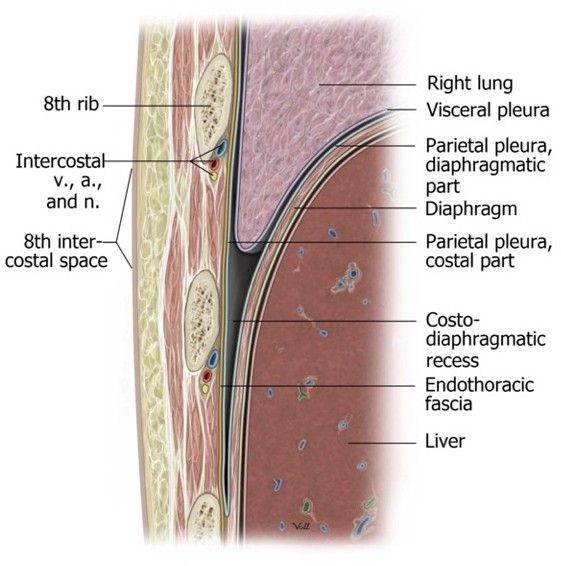
Visceral pleura invests each lung; in fact, it forms the outermost layer of the organs themselves. It is snugly adherent and difficult to remove. Being structurally part of the lungs, it is derived from splanchnic mesoderm and supplied by visceral nerve fibers.
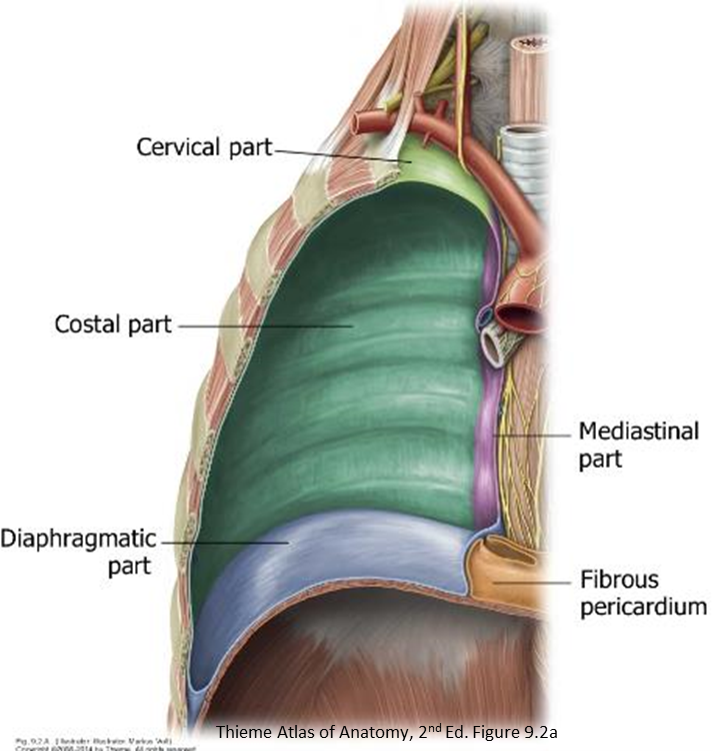
Parietal pleura lines the thoracic cavity. Since it is part of the body wall, it is derived from somatic mesoderm and supplied by somatic nerves. It is divided into named parts based upon the structures it covers:
-
- Costal pleura is glued to the inside of the anterior, lateral, and posterior thoracic wall.
- Diaphragmatic pleura covers the superior surface of the diaphragm.
- Mediastinal pleura covers the lateral sides of the mediastinum.
- Cervical pleura (a.k.a. cupula) projects above rib 1, where it forms a dome above the apex of the lung.
The four parts of the parietal pleura form a continuous layer. Sharp transitions occur where one part changes direction to become another: for example, where costal pleura leaves the anterior thoracic wall to become mediastinal pleura.
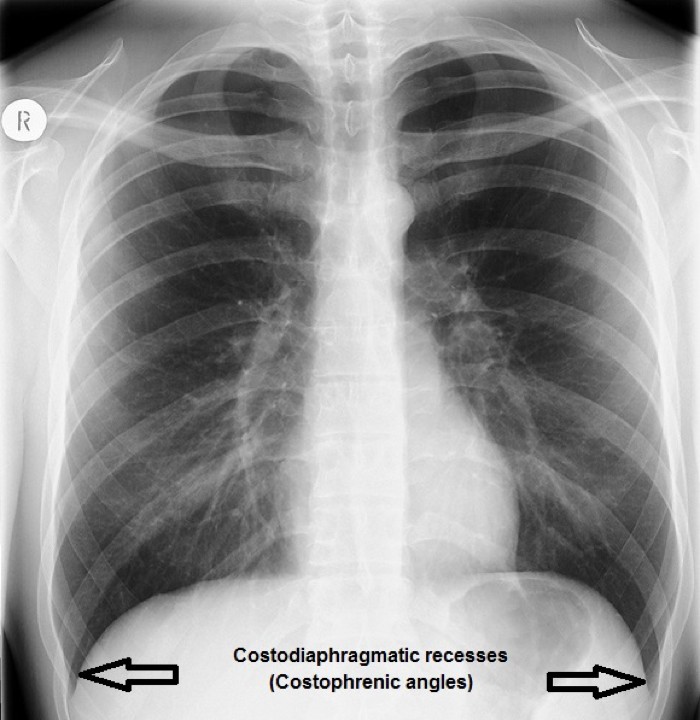

Placement of needles for thoracentesis and percutaneous liver biopsy are two examples.
Inspiration is an active process requiring contraction of muscles attaching to the rib cage. These produce movements that affect the size of the thoracic cavity in three dimensions:
-
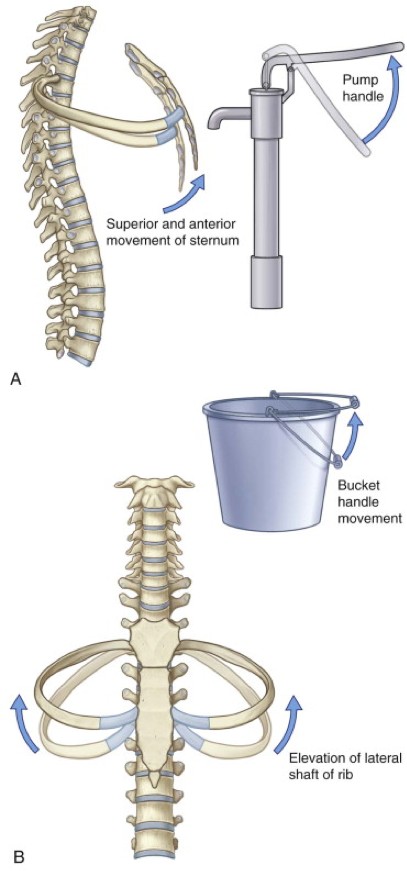
- The anteroposterior dimension is affected by elevation or depression of the upper ribs. Elevation of the ribs occurs with contraction of the external intercostal muscles. Since the anterior ends of the ribs attaching to the sternum are inferior to the posterior parts attaching to the vertebral column, elevation of the upper ribs moves the sternum forward and upward, like the motion of an old-fashioned “pump handle.”
- The transverse (lateral) dimension is affected by elevation or depression of the lower ribs. Elevation is due to contraction of the external intercostal muscles. The lower ribs are arranged as loops, with their middle portions lower than their anterior and posterior ends. Elevation of these ribs swings their middle portions laterally, like the metal handle on a bucket of paint (“bucket handle” movement).
-
- The vertical dimension is affected by elevation and depression of the diaphragm. When contracted, the diaphragm flattens and lowers, increasing the vertical dimension of the thoracic cavity. Relaxation of the diaphragm causes it to elevate, reducing the volume. The movements of the diaphragm are the most important factor in altering the volume of the thoracic cavity (accounting for 2/3 of the volume change).
Expiration is mainly passive in normal breathing, involving elastic recoil of the lungs and body wall after they have been stretched during inspiration. Forced expiration is accomplished by recruiting the internal intercostal muscles to depress the ribs and muscles of the abdominal wall to increase intra-abdominal pressure and cause the diaphragm to elevate.
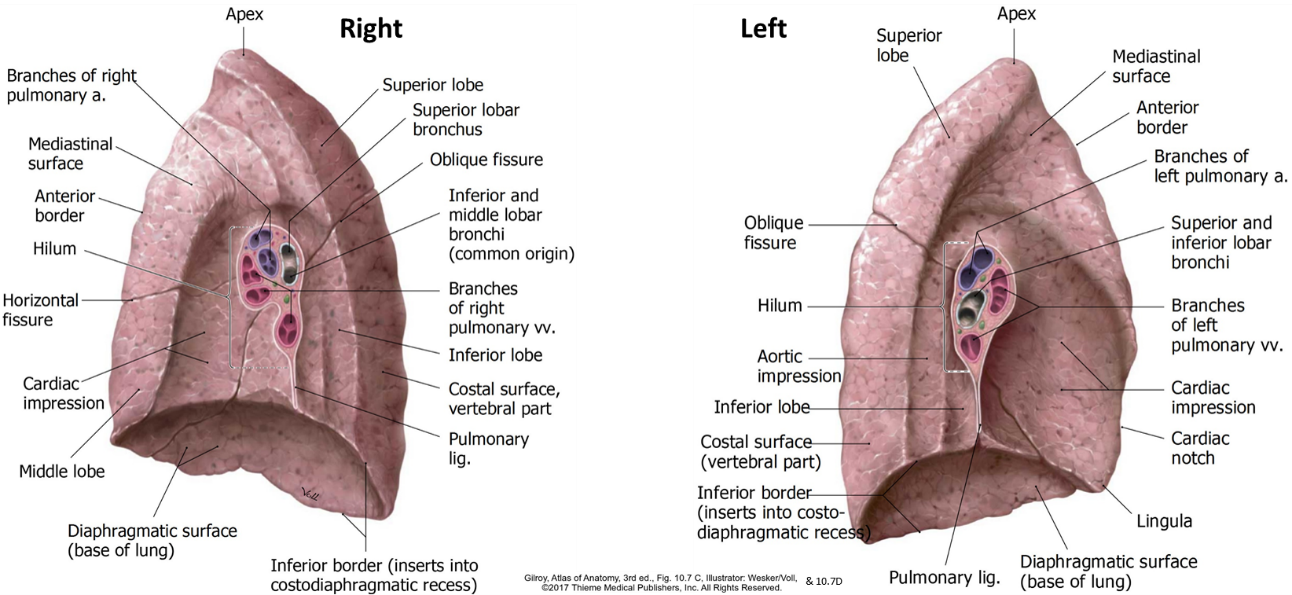
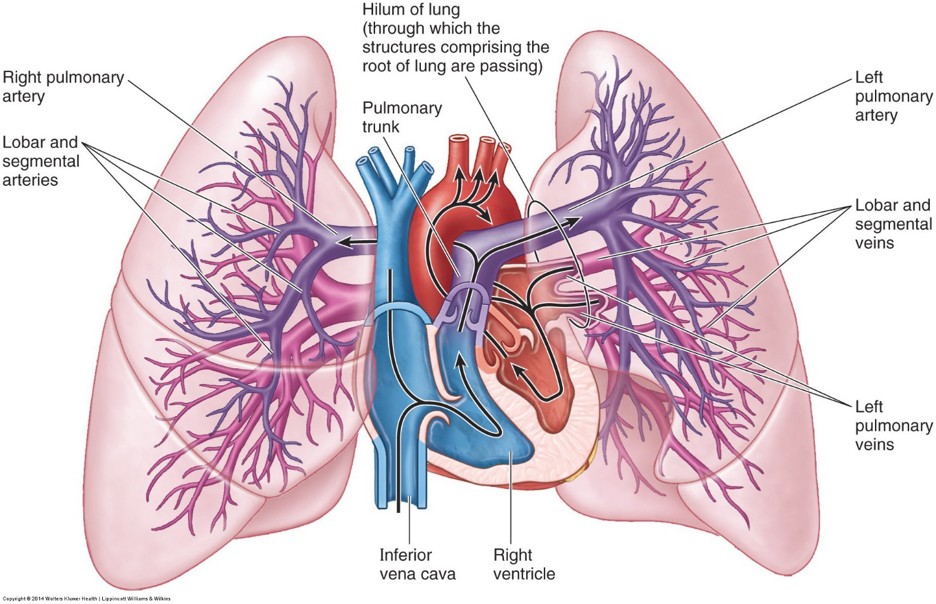
The lungs receive a double blood supply: One set of vessels for gas exchange/oxygenation (pulmonary vessels) and one set for the metabolic needs of the lung tissues (bronchial vessels).
Pulmonary arteries: Transmit poorly oxygenated blood
- Right and left pulmonary arteries (1 per lung): Bifurcate from the pulmonary trunk to the left of the ascending aorta.
- The left pulmonary artery is short and vertical. It enters the hilum of the left lung above the left main bronchus.
- The right pulmonary artery is longer and horizontal. It passes under the arch of the aorta. As it enters the hilum of the right lung, it divides into a right upper lobe artery and an interlobar artery. These are posterior to the right main bronchus.
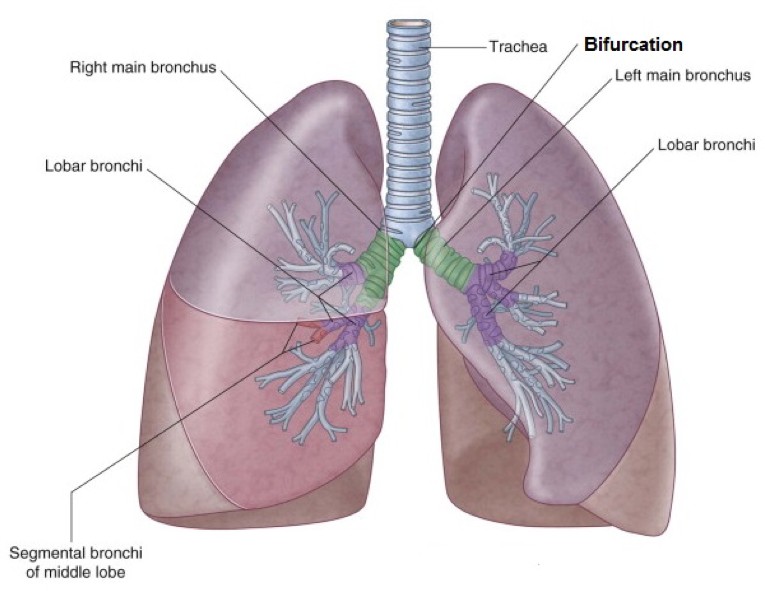
- The branching pattern of the pulmonary arteries follows that of the air tubes.
- Ultimately give rise to pulmonary capillaries, which participate in gas exchange with the alveoli.
Pulmonary veins
- Two per lung: Superior and inferior. Carry oxygen-rich blood away from the lungs.
- Enter the left atrium of the heart.
Bronchial vessels
- Bronchial arteries (1 or 2 per lung) arise from the thoracic aorta or intercostal arteries. They follow the bronchial tree, branching in the same pattern. Supply the metabolic needs of the air tubes, supporting tissues of the lungs, and the visceral pleura.
- Bronchial veins drain into the azygos and accessory hemiazygos veins. They drain blood from the bronchial tree, but apparently not the visceral pleura. Venous blood from visceral pleura drains into the pulmonary veins. Odd.
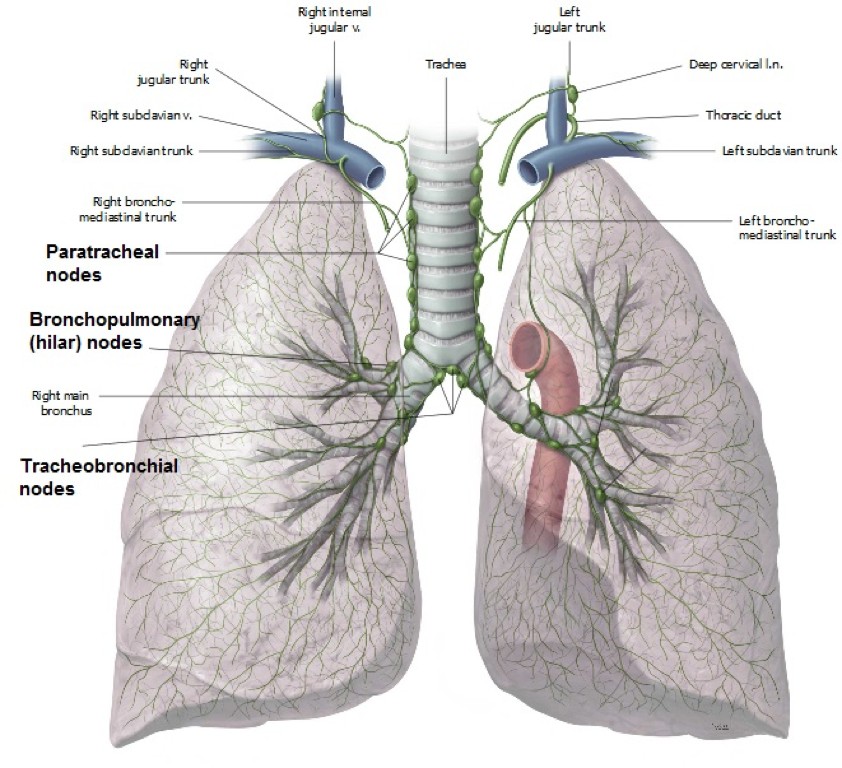
Lymph from the lungs percolates sequentially through the following nodes:
-
-
- Pulmonary nodes: located in the substance of the lung, along bronchi.
- Bronchopulmonary (hilar) nodes: Located in the lung hilum.
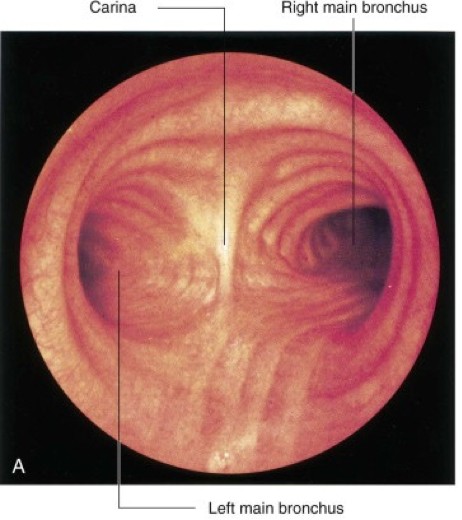
- Tracheobronchial nodes: Huge nodes located at or near the tracheal bifurcation.
- Paratracheal nodes: Located around the trachea and arch of the aorta.
- Lymph from paratracheal nodes enters lymph trunks in the thoracic cavity that drain upwards toward the base of the neck. Here the trunks enter the venous angles (= junctions of the internal jugular and subclavian veins). Variations occur often—sometimes the lymph trunks merge with the thoracic duct on the left or the right lymphatic trunk on the right.
-
The lungs are supplied by the left and right pulmonary plexuses. These contain a mixture of parasympathetic, sympathetic, and visceral afferent nerve fibers.The pulmonary plexuses are located on the left and right main bronchi and are carried into the lungs as the air tubes branch and re-branch.
Parasympathetic fibers are preganglionic and derived from the vagus nerves. They synapse on postganglionic cell bodies in ganglia in the walls of the bronchial tree. Functions:
-
-
Motor to smooth muscle in air tubes (bronchoconstriction)
-
Stimulate glands (mucous secretion)
-
Vasodilation of pulmonary vessels
-
Sympathetic fibers are postganglionic and derived from the sympathetic trunk. Functions:
-
- Relax smooth muscle in air tubes (bronchodilation)
- Inhibit glandular secretion
- Vasoconstriction of blood vessels
Visceral afferent fibers transmit both subconscious reflexive information and pain due to noxious stimuli.
Reflex information is carried to the CNS in the vagus nerves:
-
- Touch sensations for cough reflexes
- Stretch detection for limiting inspiration (Hering-Breuer reflex)
- Baroreceptors and chemoreceptors in pulmonary vessels
Pain signals (probably from visceral pleura and air tubes) are carried to the CNS via reverse sympathetic pathways, entering the spinal cord via upper thoracic spinal nerves.
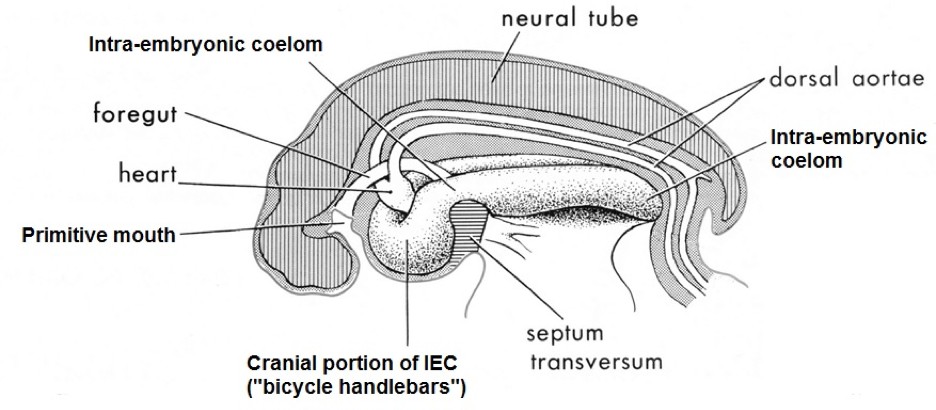
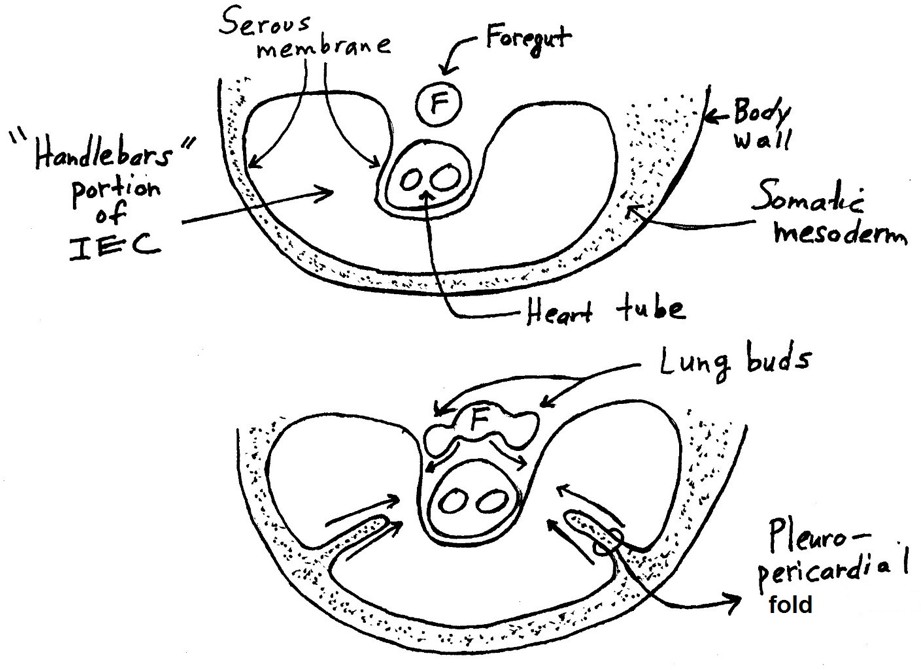
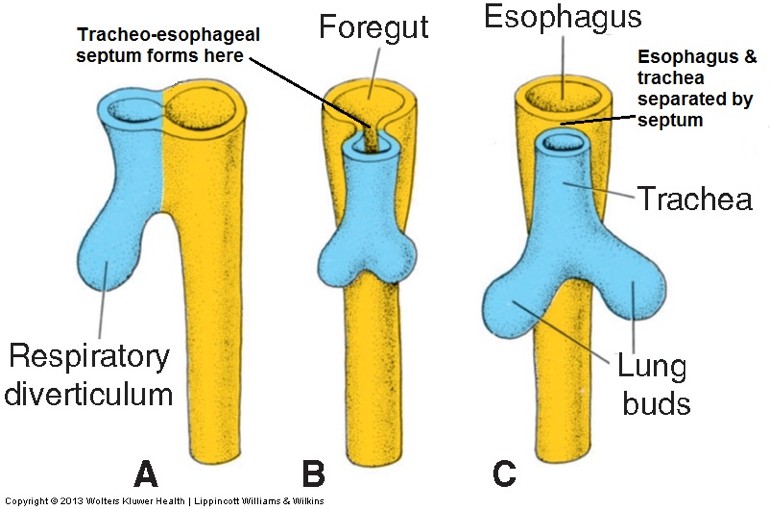
As described earlier in our embryology session, the primitive body cavity (intra-embryonic coelom = IEC) was lined by a primordial serous membrane. The serous membranes that surround the lungs are produced when the cranial portion of the IEC is partitioned into pleural and pericardial sacs.
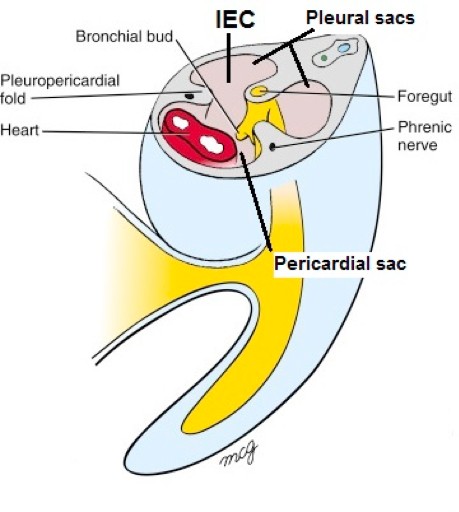
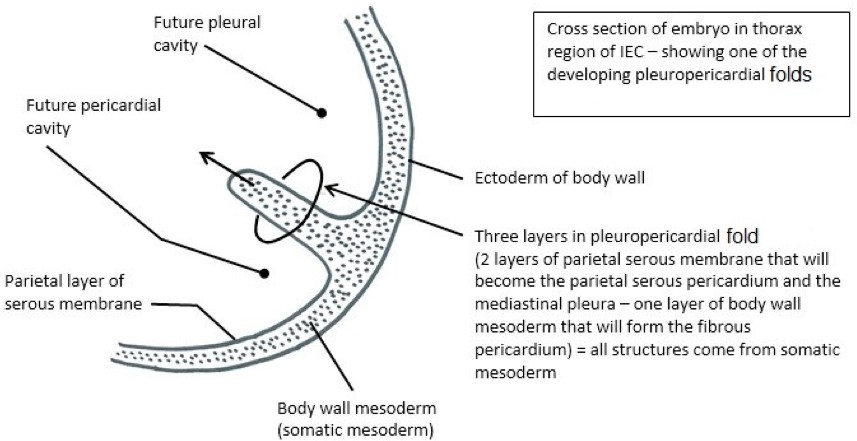
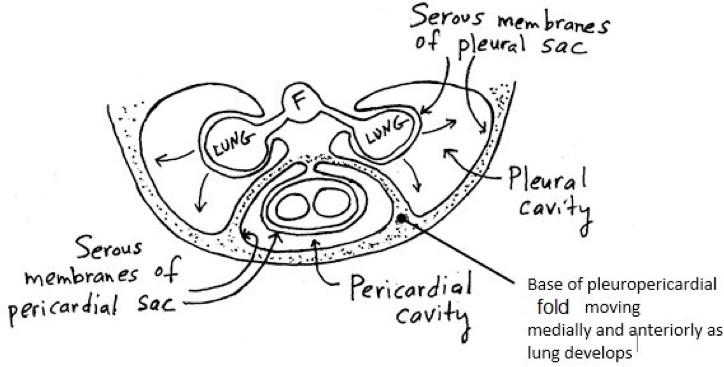
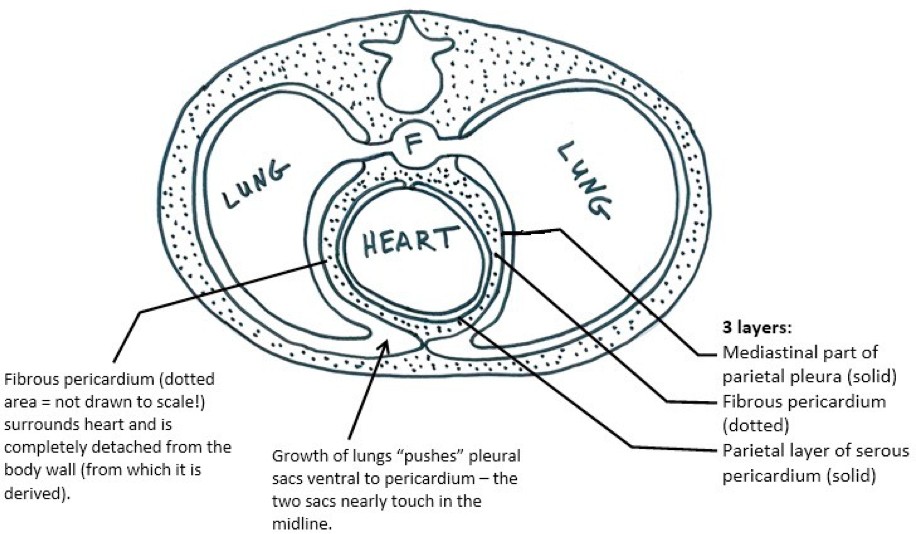
During the 5th week, left and right folds of somatic mesoderm are “pulled off” the inside of the lateral body wall in the cranial (“bicycle handlebars”) region of the IEC. Although these folds appear to migrate medially toward the midline on their own, it is the growth of the heart and associated movement of blood vessels adjacent to the IEC that produces these pleuropericardial folds. The folds grow toward the midline and eventually fuse posterior to the developing heart, partitioning the “handlebar-shaped” portion of the IEC into two posterolateral pleural sacs and a midline pericardial sac.