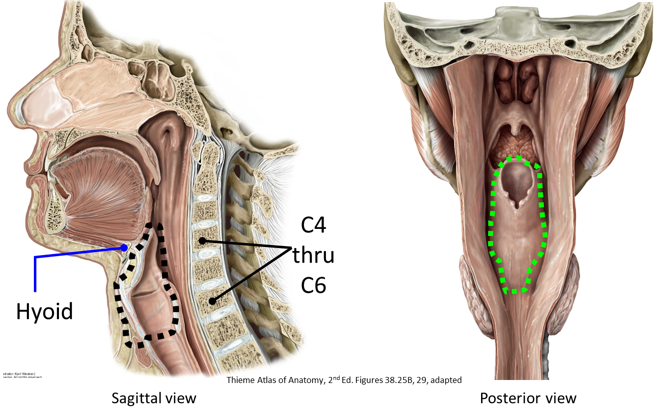
The larynx is an organ of the respiratory system and the part of the airway situated between the pharynx and trachea. It is located anterior to the lower pharynx and esophagus, between the levels of C-4 to C-6 vertebrae. Textbooks consider the larynx to be the most inferior part of the upper respiratory tract. It consists of cartilages, ligaments, skeletal muscles, vocal folds, a mucosal lining, nerves, and arteries. The “skeleton” of the larynx is composed of cartilage. The larynx is a superficial structure—several of its cartilages are easily visible and palpable on the surface of the neck. Therefore, it is vulnerable to injury due to penetrating wounds or blunt trauma.
Largest but incomplete cartilage; it is entirely open posteriorly. A visual analogy is an open textbook, standing upright.
Two flat surfaces laterally = laminae; they are fused in the midline to form the laryngeal prominence (“Adam’s apple”). The prominence is the spine of the textbook in our analogy. Males have larger thyroid cartilages than females and the angle between the laminae is more acute, causing the Adam’s apple to be more prominent.
To the laminae are attached the inferior constrictor, sternothyroid, and thyrohyoid muscles.
Superior horn of thyroid cartilage: Connected superiorly to the hyoid via the thyrohyoid membrane.
Inferior horn of thyroid cartilage: Articulates with the cricoid cartilage at the cricothyroid joints, which help to adjust the length of the vocal folds.
Shaped like a “signet (class) ring.” The only laryngeal cartilage that completely surrounds the airway. Has a short arch anteriorly and a tall lamina posteriorly.
Attached to the first tracheal ring by a ligament.
Figure 36.2.
Elastic cartilage covered by a mucous membrane; functions to cover the laryngeal opening (inlet) when swallowing.
Attached by ligaments to both the thyroid cartilage and hyoid bone.
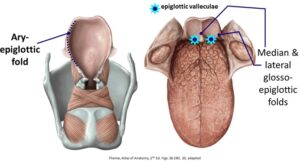
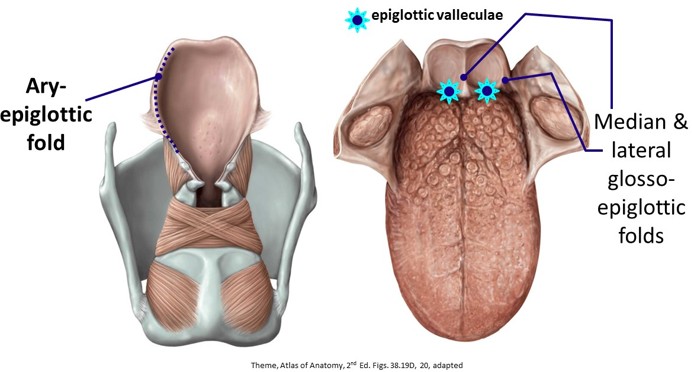
Laryngeal inlet: Entrance to the larynx anterior to the pharynx; anterior border of the inlet is formed by the free margin of the epiglottis.
Aryepiglottic folds: Lateral mucosal borders of the inlet extending from arytenoid cartilages (described next) to the epiglottis.
The epiglottis is attached to the root of the tongue by three mucosal folds = these are the glosso-epiglottic folds.
The epiglottic valleculae are the two depressions between the glosso-epiglottic folds. These are important landmarks for tracheal intubation procedures.
These are pyramid-shaped cartilages that are perched atop the lamina (posterior part) of the cricoid cartilage. They are covered by a mucous membrane. The bases of arytenoid cartilages have two processes = vocal and muscular.
Muscular process: Project laterally. Attachment of posterior and lateral cricoarytenoid muscles
Crico-arytenoid joints: articulation with the cricoid lamina; the arytenoid cartilages move atop the cricoid cartilage = they can rotate and glide.
Movement of the arytenoid cartilages abduct or adduct the vocal folds, thus widening or narrowing the space between the vocal folds.
Clinical correlation
A cricothyrotomy is a procedure used in an emergency to establish an airway by placing a tube through an incision in the skin and underlying cricothyroid membrane. It is rarely performed but can be lifesaving if intubation cannot be carried out to establish an airway through the respiratory passageways above. Unlike tracheostomy (described in
Overview of the Neck Viscera; Thyroid and Parathyroid Glands), there are no large blood vessels between the cricothyroid membrane and the skin.
Larygneal cavity (Airway of the larynx)
The cavity (airway) of the larynx is lined by a mucous membrane. Its parts are named as are the mucosal folds in its lateral walls.
Two mucosal folds project into the laryngeal cavity and define the spaces of the interior larynx (more on these folds below in the Fibro-elastic Membranes section):
Vestibular folds
“False” vocal folds, because they do not function to produce sound. The space between the vestibular folds in the midline of the airway is the rima vestibuli.
Vocal folds (“vocal cords”)
These are the “true” vocal folds, since they produce sound when vibrated. The space between the vocal folds in the midline of the airway is the rima glottidis.
The glottis is defined as the part of the larynx that produces sound. The structures that make up the glottis therefore are the vocal folds + rima glottidis (the space between vocal folds). The vestibular folds do not produce sound, so they are not part of the glottis.
Clinicians use the glottis as a landmark for describing diseases and lesions = supraglottic or infraglottic.
FYI
Singers know about the glottis, because certain vocal techniques make use of an open glottis or sudden closures of the glottis (“glottal stops”).
Clinical correlation
Examination of the laryngeal cavity is called laryngoscopy.
Indirect laryngoscopy is the simplest type. It is done with an angled mirror and a light.
Direct laryngoscopy is more involved. Direct visualization of the laryngeal airway is gained with the use of a curved blade inserted into the region of the epiglottic valleculae to push down the tongue. The clinician is positioned above the head of the recumbent patient in order to look into the laryngeal cavity. This procedure is done under general anesthesia, to biopsy laryngeal tissue or to facilitate endotracheal intubation. Direct laryngoscopy can also be done with a fiber-optic scope placed through the nasal cavity and down the pharynx.
Fibro-elastic membranes
The lateral walls of the laryngeal cavity are supported by fibro-elastic membranes deep to the mucosa. These impart rigidity to the mucosal folds as well as elastic flexibility.
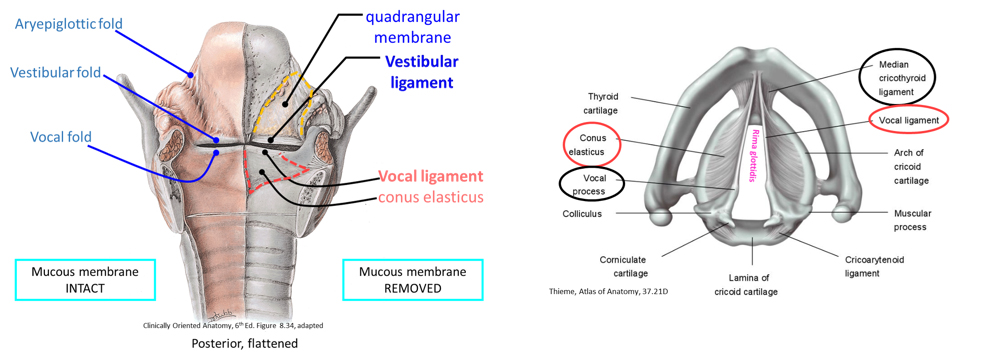
Figure 36.3. Coronal section of laryngeal cavity. The fibro-elastic membranes deep to the mucosa are diagrammed: Quadrangular membrane deep to the vestibular folds and the conus elasticus deep to the vocal folds.
Submucosal sheet of fibro-elastic tissue, extending between the ary-epiglottic folds above to the vestibular folds below.
Vestibular ligaments: Free inferior margins of the quadrangular membranes. These stretch from the internal aspect of the thyroid cartilage anteriorly to the arytenoidcartilages posteriorly. The mucous membrane covered vestibular ligament is the vestibular fold—the ligament is the fibro-elastic core of the fold that gives it stability.
The vestibular folds are not used to phonate—instead, their function appears to be to protect the airway and to assist the vocal folds in closing the airway when performing a Valsalva maneuver (the “bearing down” technique used when lifting a heavy object or when increasing intra-abdominal pressure to defecate).
Rimavestibuli: Space between the vestibular folds.
Submucosal sheet of fibro-elastic tissue, extending between the internal surface of the cricoid cartilage below to the vocal folds above.
Vocal ligaments: thickened free upper margins of the conus elasticus. These stretch from the internal aspect of the thyroid cartilage anteriorly to the vocal processes of the arytenoid cartilages posteriorly. The mucous membrane covered vocal ligament is the vocal fold (vocal cord)—the ligament is the fibro-elastic core of the vocal fold.
Rima glottidis: Opening between the two true vocal folds
Table 36.1. Intrinsic muscles of the larynx
Muscle
Action
Innervation
Muscles that affect the position of the vocal folds and size of the rima glottidis
Posterior crico-arytenoid
Rotate arytenoid cartilages to abduct the vocal folds
Widen rima glottidis
Recurrent laryngeal nerve
Lateral crico-arytenoid
Rotate arytenoid cartilages to adduct vocal folds
Narrow rima glottidis
Recurrent laryngeal nerve
Transverse arytenoid
Slides arytenoid cartilages medially to adduct vocal folds
Close the posterior part of the rima glottidis.
Work with the lateral crico-arytenoid to completely seal the airway
Recurrent laryngeal nerve
Muscles that affect the tension on the vocal folds
Cricothyroid
Tilt thyroid cartilage forward to tense the vocal folds
Raise the pitch of the voice
External laryngeal nerve
Thyro-arytenoid
Approximate the arytenoid cartilages to the thyroid cartilage to relax the vocal folds
Lower the pitch of the voice
Recurrent laryngeal nerve
Vocalis
Medial-most fibers of the thyro-arytenoid; located within the vocal folds.
Muscle fibers insert directly on the vocal ligament.
Tenses and thickens segments of the vocal fold to vary the tonal qualities and pitches of the voice.
Recurrent laryngeal nerve
Clinical correlation: Regional pathologies of the larynx
Enlargement of the ventricular saccule may produce a diverticulum called a laryngocele. The mucous membrane in the ventricles has many mucous glands. In laryngitis, these become enlarged and secrete an over-abundance of mucous, which covers the vocal folds. With the subsequent edema, it's hard to phonate—hoarseness results.
The vocal folds are common sites of tumors and nodules, which can produce hoarseness. These folds have no direct lymph drainage, so if the tumor is malignant, early removal may prevent metastasis.
Laryngeal muscles
The skeletal muscles that act upon the larynx can be organized into two categories:
Extrinsic laryngeal muscles
Move the larynx as a whole: infrahyoid muscles depress it; suprahyoid muscles and stylopharyngeus muscle elevate it.
Intrinsic laryngeal muscles
Alter length or tension of the vocal ligaments,or change the size and shape of the rima glottidis. A table that summarizes the intrinsic muscles of the larynx is provided below.
Innervation: Recurrent laryngeal (all intrinsic muscles, except one) and external laryngeal nerves (one intrinsic muscle = the cricothyroid).
Figure 36.4.
Figure 36.5.
Figure 36.6.
Figure 36.7.
Figure 36.8.
Figure 36.9.
In addition to their effects on vocal quality, intrinsic muscles also act as sphincters, bringing the ary-epiglottic, vestibular, and vocal folds together Working together, intrinsic muscles of the larynx can completely close the airway when we swallow, hold our breath, or perform a Valsalva maneuver.
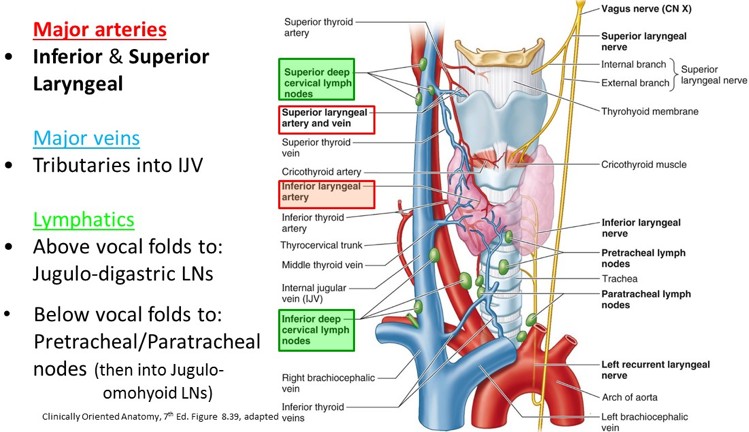
Superior laryngeal: Branches off the vagus nerve just below the jugular foramen.
External branch (motor): Also called the external laryngeal nerve. Descends posterior to the sternothyroid with the superior thyroid artery. It lies on the inferior constrictor muscle.
Supplies: Inferior constrictor muscle and cricothyroid muscle.
Internal branch (sensory): Also called the internal laryngeal nerve. Pierces the thyrohyoid membrane (with superior laryngeal artery)
Sensation to the mucosa of the laryngeal cavity above the vocal fold and including the vocal fold.
Recurrent laryngeal
Runs in the tracheo-esophageal groove
Enters the larynx by passing deep to the inferior border of the inferior constrictor muscle with the inferior laryngeal artery.
Supplies all the intrinsic muscles of the larynx,EXCEPT the cricothyoid.
Sensory to the mucosa of the laryngeal cavity below the vocal fold inferiorly into the trachea
Lymphatics drain along the blood vessels upwards and downwards, to superior and inferior deep cervical nodes.
Clinical correlation
The internal laryngeal nerve is an important nerve because it provides sensory fibers to the upper larynx = the area of the laryngeal cavity just inside the larygneal inlet. Any foodstuffs of liquids that should enter the laryngeal airway from the pharynx stimulate sensory fibers of the internal laryngeal nerve and elicit a pwerful cough reflex in order to eject the offending substances. The internal laryngeal nerve is therefore known as the "guardian of the airway."
Clinical correlation
The relationship of the recurrent laryngeal nerves to the thyroid glad and inferior thyroid arteries has already been discussed. Surgeons should be aware of this to prevent damage to the nerves.
Additionally, paratracheal lymph nodes are found along the tracheo-esophageal grooves in proximity to the recurrent laryngeal nerves, as are mediastinal nodes near the arch of the aorta. Node enlargement (lung cancer, lymphoma) could impinge upon the nerves, producing symptoms of dysphonia.
Trachea
1 inch in diameter in adults.
Extends from the inferior end of the larynx into the thorax.
“C” shaped hyaline cartilage rings, with the posterior open ends connected by smooth muscle (trachealis).
Common carotid arteries and lobes of the thyroid gland are located lateral to the trachea.