The “lay of the land”: The pelvic viscera are below the peritoneum, surrounded by visceral pelvic fascia, and separated from one another by subperitoneal pelvic connective tissue “packing material.”
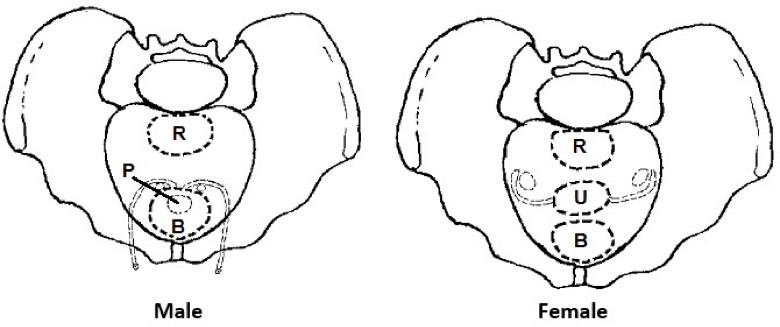
Most of the organs in the pelvic cavity (rectum, uterus, prostate, and bladder) line up in a row along the midline, between the sacrum and pubic symphysis. The only organs that don’t are the ovaries, uterine tubes, and ductus deferentes.
Figure 20.1 Drawings demonstrating the organization of pelvic viscera, superior view. HAND-DRAWN CONLEY-GRAMS.
Urinary organs
Ureters
Muscular tubes that convey urine from the kidneys to the bladder. Half of their course is in the posterior abdominal wall (abdominal portion) and half in the pelvic cavity (pelvic portion).
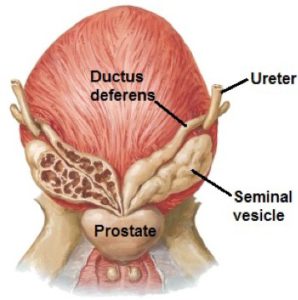
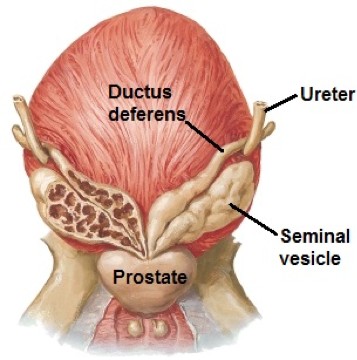
Figure 20.2 Ureter relations in the male. NETTER, ATLAS OF HUMAN ANATOMY, PLATE 362.Ureters cross the pelvic brim near the bifurcation of the common iliac arteries.
They enter the posterolateral corners of the bladder.
In the male, behind the bladder, each ureter enters the bladder sandwiched between the ductus deferens above and the seminal vesicle below.
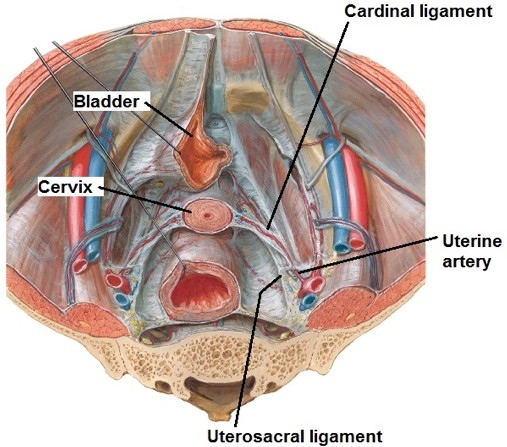
In the female, the ureters pass under the uterine arteries in the cardinal ligament. As the ureters approach the bladder, they are close to the cervix and vagina.
Sympathetic: Vascular tone of blood vessels; apparently does not innervate the ureter itself.
Parasympathetic: Stimulates peristalsis in ureter smooth muscle.
Afferent: Most of the ureter is above the pelvic pain line, so pain follows sympathetic routes to lower thoracic and upper lumbar spinal cord levels.Pain from kidney stone blockage in the ureter refers to the lower back and groin region. Which dermatomes are these?
Urinary bladder
The bladder stores urine. An empty bladder is almost entirely in the pelvic cavity behind the pubic bones where it rests on the pelvic diaphragm. However, when distended after a night at your favorite watering hole, it can rise into the abdomen as high as the umbilicus!
The empty bladder (rarely the case in the living body) is shaped like an inverted pyramid, and its anatomic parts are described in its empty state. The actual position and shape of the bladder vary according to the amount of urine it contains and the age of the person.
Superior surface (dome of the bladder) is covered by peritoneum. The other surfaces of the bladder are subperitoneal.
Posterior surface is called the base or fundus of the bladder.
Apex of bladder: Connects the bladder to the anterior abdominal wall via a fibrous cord called the median umbilical ligament (urachus).
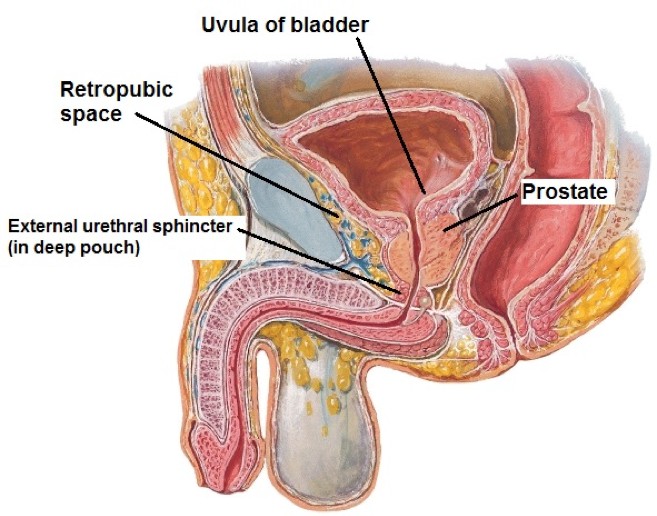
Neck of bladder: Points inferior. This is where urine leaves the bladder and enters the urethra. In the male, the neck rests on the prostate and is fused to it.
Figure 20.3 NETTER, ATLAS OF HUMAN ANATOMY, PLATE 313.
The mucosa of the empty bladder is folded and loose, except in an area at the base called the trigone, where it is smooth and firmly tacked down to the underlying muscle.
The trigone is defined by three orifices = two internal ureteric orifices and the internal urethral orifice. The trigone is at the base of the bladder.
The trigone may be elevated in males = this is called the uvula of the bladder. It can become quite prominent in older males when the underlying prostate enlarges.
The smooth muscle in the bladder wall is called the detrusor (Latin = “to drive away”). It contracts to squeeze out the urine. The detrusor is the juicer!In the neck, smooth muscle forms the involuntary internal urethral sphincter.
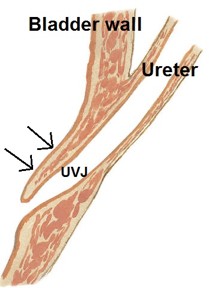
Ureterovesical junction (UVJ): The ureters pass through the wall of the bladder at an oblique angle. This is the intramural part of the ureter. As the bladder fills and distends, the intramural part closes to prevent backflow of urine from bladder into ureter. This valve mechanism doesn’t work so well in children because the intramural part of the ureter is short and there is not enough bladder musculature. Reflux of urine is a common cause of urinary tract infections in kids.
Sympathetic: Facilitates continence and bladder filling by relaxing the detrusor muscle and causing contraction (closing) of the internal urethral sphincter.
Parasympathetic: Pelvic splanchnic nerves facilitate voiding by causing contraction of the detrusor muscle and relaxing the internal urethral sphincter.
Afferent: Carry information concerning stretch, fullness, and burning/pain associated with urgency. Afferents from the dome of the bladder (at the pelvic pain line) probably follow sympathetics to the lower thoracic and upper lumbar spinal cord levels. Afferents from the base and neck follow the pelvic splanchnic nerves to sacral spinal cord segments. Since most of the bladder is below the pelvic pain line, patients with inflammation of the bladder (cystitis) often complain of pain in the “saddle” region of the perineum = S-2 to S-4 dermatomes.
A rest-and-digest function, regulated by parasympathetic innervation. It is under voluntary control but may occur asa reflex involving the micturition center in the brainstem, as in children not “toilet-trained” or when one has an intense fight-fright-flight emergency response.
As the bladder fills, stretch receptors communicate fullness to the brain, causing reflex contraction of the detrusor muscle and relaxation of the internal urethral sphincter.
This reflex can be overcome by contraction of the voluntary external urethral sphincter in the deep perineal pouch (if you are toilet trained!), preventing flow of urine in the urethra.
Conscious relaxation of the pelvic diaphragm and external urethral sphincter allows urine to flow. When you can’t relax (as in a crowded public restroom), tense muscles and sympathetic closure of the internal urethral sphincter results in an unfortunate inability to micturate.
This site has a nice description of neural control of micturation.
Urethra
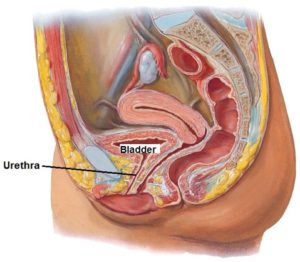
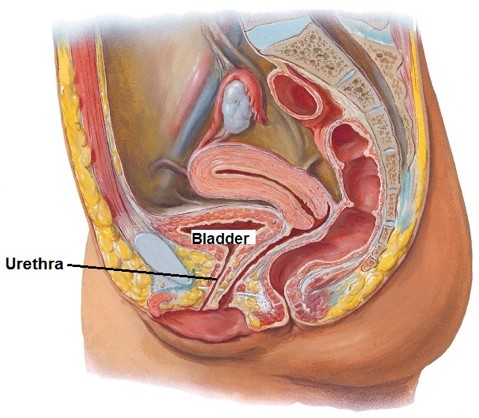
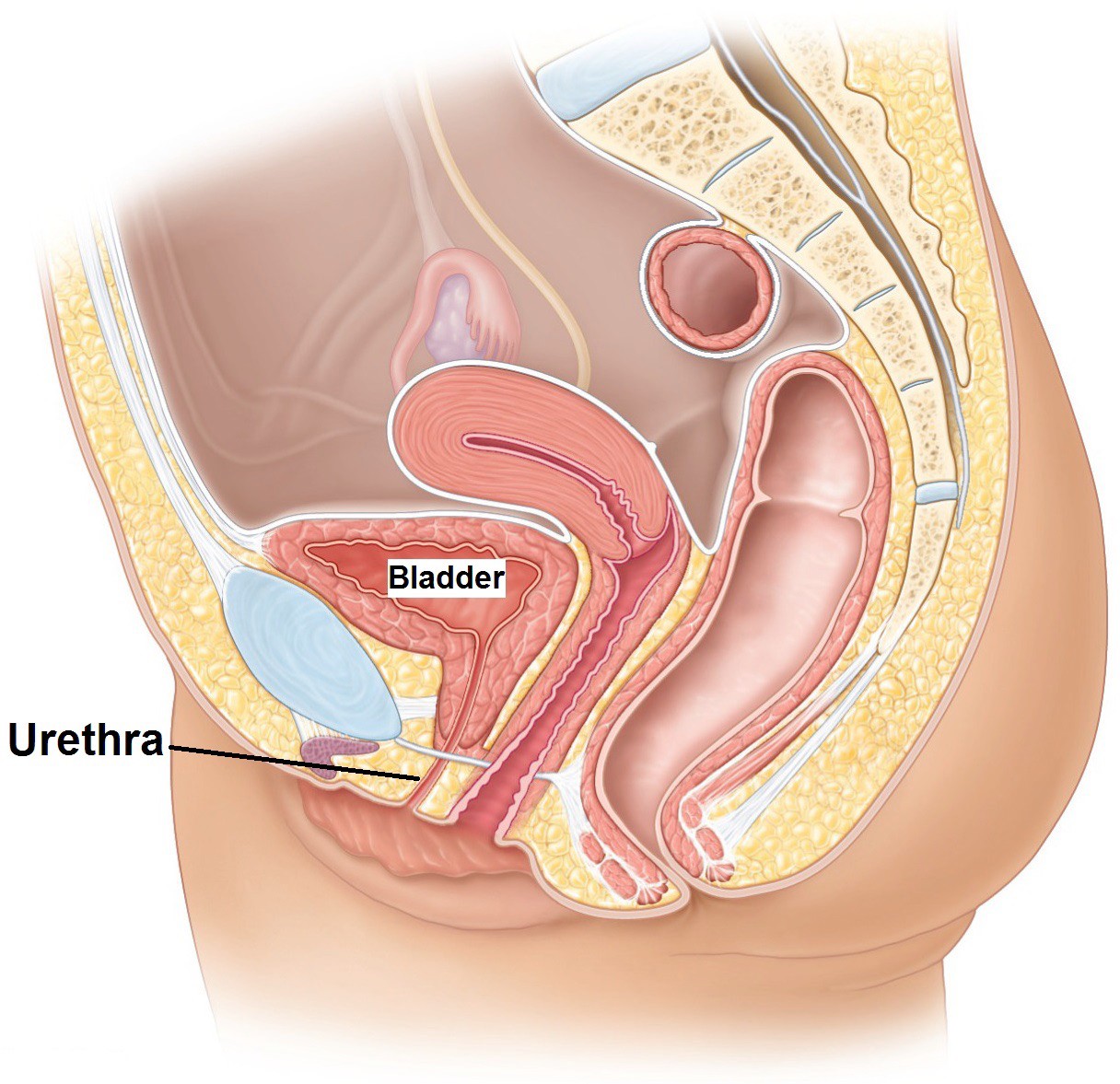
Female
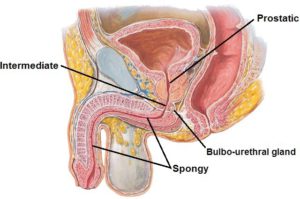
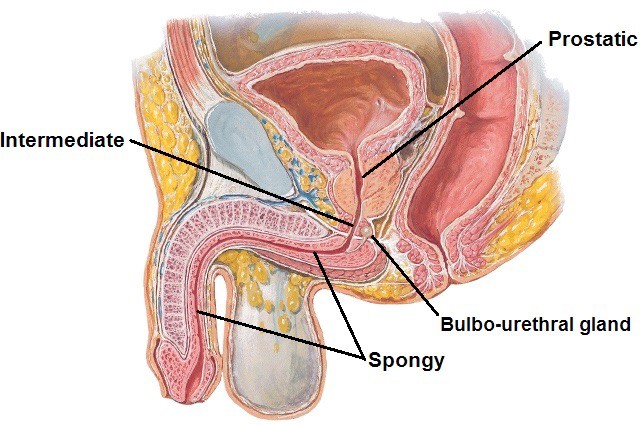
Male
Figure 20.4 NETTER, ATLAS OF HUMAN ANATOMY, PLATE 340.
Short (~4 cm) and straight.
Passes through the urogenital hiatus in the pelvic diaphragm with the vagina and then through the deep perineal pouch.Most of the female urethra is in the perineum.
It opens just anterior to the vagina in the vestibule (described earlier with the perineum).
Figure 20.5 NETTER, ATLAS OF HUMAN ANATOMY, PLATE 344.
Relatively long, ~20 cm and sharply curved at the base of the penis. This region is liable to injury if penetrated by an improperly inserted catheter.
Carries semen as well as urine.
Three portions:
Prostatic
Intermediate (membranous)
Spongy.
Only the prostatic portion is contained in the pelvic cavity. The other parts are in the perineum and penis.
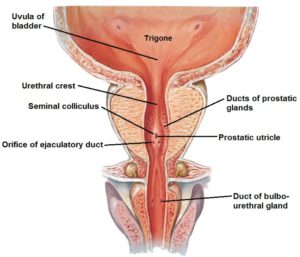
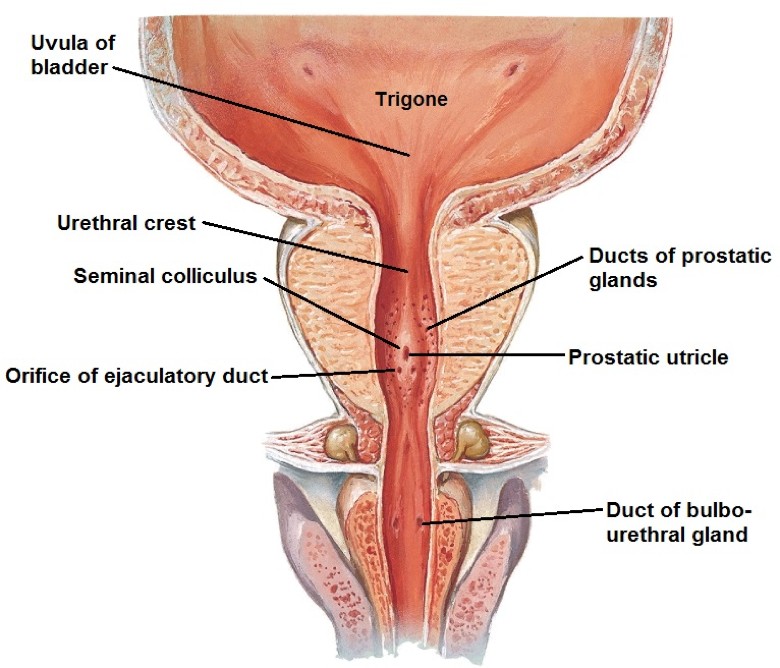
Figure 20.6 NETTER, ATLAS OF HUMAN ANATOMY, PLATE 362.
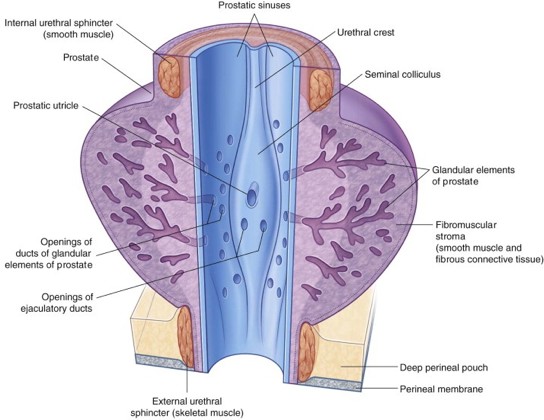
The prostatic urethra traverses the prostate—about 3 cm in length. The posterior wall (“floor”) has several unique features:
A median ridge called the urethral crest.
A raised circular mound in the crest called the seminal colliculus (known to clinicians as the verumontanum: Latin = mountain ridge), the center of which contains a small diverticulum known as the prostatic utricle. Believe it or not, the utricle is the male homologue of the female uterovaginal canal (the caudal end of the embryonic paramesonephric ducts).
The openings of the ejaculatory ducts are indicated by two small slits on the seminal colliculus on either side of the prostatic utricle.
Channels on either side of the urethral crest are called the prostatic sinuses, where the orifices of the prostatic ducts open—the ducts of the dozens of prostatic glands.
Clinical correlation
The female bladder is more prone to infection than the male because the female urethra is short and straight, making microbial access easier. The female external urethral orifice is also closer to the vagina and anus, so it can more easily receive bacteria from these areas.
The rectum is the segment of the large intestine in the pelvis situated between the sigmoid colon and anal canal. It begins at the level of the third sacral vertebra (rectosigmoid junction) and descends along the curve of the sacrum and coccyx.
Anterior: Rectovesical pouch, prostate, and seminal vesicles (male); recto-uterine pouch (containing loops of ileum), cervix and vagina (female).
Posterior: Sacrum and coccyx.
Lateral: Pelvic plexus of nerves and pelvic diaphragm.
Figure 20.7 Relations of rectum in female. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE 3.34.Figure 20.8 Relations of rectum in male. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE 3.34.
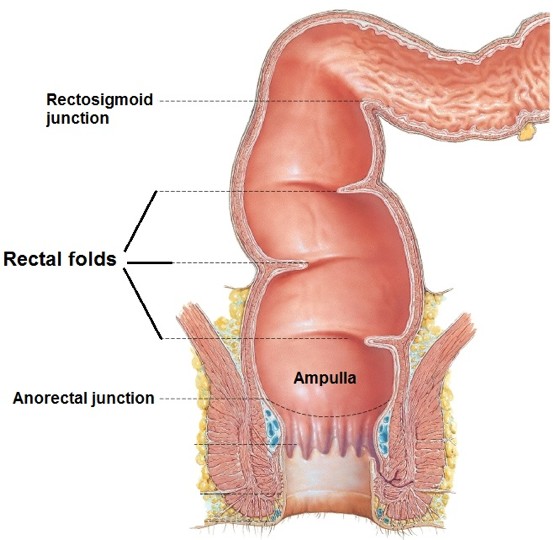
Figure 20.9 Netter, Atlas of Human Anatomy, Plate 371.
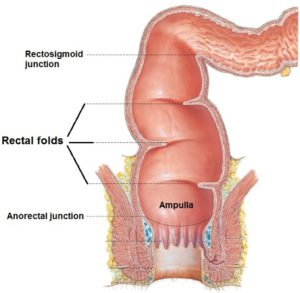
Contrary to what the name “rectum” implies, it is not straight.
The anterior-posterior curvature (concavity faces forward) fits the hollow of the sacrum.
The rectum has three sharp lateral flexures, each forming a transverse fold internally: the rectal folds (valves of Houston). This gives the rectum an S-shaped profile when viewed from the front.
The “rectal threes” = rectum begins at S-3 and it has 3 rectal folds produced by 3 lateral curves.
The lower, dilated part (below the inferior-most rectal fold) is the ampulla, which receives and accumulates a mass of feces for defecation.
Its longitudinal layer of smooth muscle is complete: there are no taeniae coli nor haustra in the rectum.
The lower 2/3 is subperitoneal because of the peritoneal reflection that forms the rectovesical pouch (male) or recto-uterine pouch (female).
The lower limit of the rectum is at the pelvic diaphragm, where the puborectalis muscle marks the anorectal junction. The rectum and anal canal meet at a backward facing 80 degree angle here.
Superior rectal artery (from inferior mesenteric) and middle rectal artery (from internal iliac).
Venous drainage: A submucosal rectal venous plexus drains to the superior rectal vein (portal drainage) and middle rectalveins (systemic drainage = IVC).
Sympathetic: From upper lumbar segments of spinal cord to pelvic plexus via the hypogastric nerves—this is vasomotor,but may also relax smooth muscle to inhibit peristalsis and constrict the internal anal sphincter.
Parasympathetic: From pelvic splanchnic nerves—stimulates peristalsis; relaxes internal anal sphincter.
Afferent: Carry information concerning stretch and fullness to the sacral spinal cord via pelvic splanchnic nerves. Most of the rectum is below the pelvic pain line, so pain is referred to sacral dermatomes and is poorly localized in the pelvic region.
The rectum fills slowly during the day, the feces being delivered by peristalsis in the descending and sigmoid colons.
The urge to defecate is initiated by mucosal receptors in the ampulla. This induces the relaxation of the internal anal sphincter (smooth muscle) and increases rectal peristalsis.
Reflex stimulation of the external anal sphincter (skeletal muscle) resists the pressure produced by peristalsis—maintaining fecal continence.
Relaxation of the voluntary sphincter and puborectalis muscle and initiation of the Valsalva maneuver (“bearing down”) with continued peristaltic activity empties the rectum.
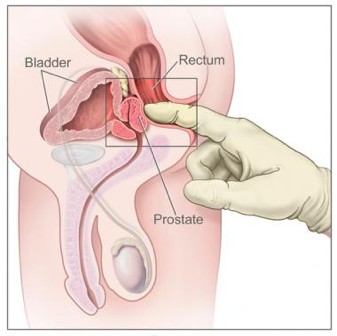
Clinical correlation: Digital rectal examination
In the male, the wall of the rectum, sacrum, coccyx, ischial spines, posterior surface of prostate, bulb of penis, and a full bladder can be palpated. An abnormal seminal vesicle may also be felt “per rectum.”
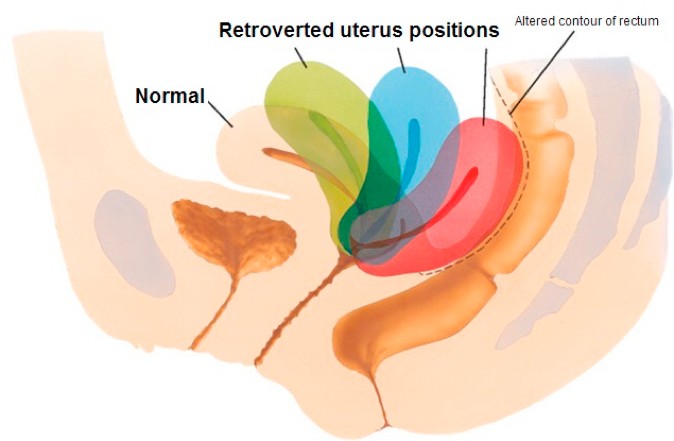
In the female, the rectal wall, sacrum, coccyx, ischial spines, uterosacral ligaments, cervix, and posterior vaginal wall can be palpated. A retroverted uterus and abnormal contents in the recto-uterine pouch (pouch of Douglas) may be felt.
Figure 20.10
Female internal genitalia
Vagina
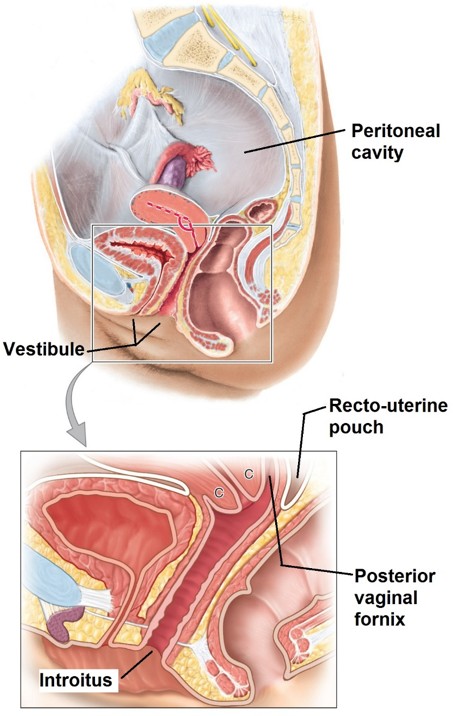
Figure 20.11 MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE 3.43.
The vagina (Latin = “sheath”) is a musculo-membranous tube about 10 cm in length. It inclines posteriorly as it ascends, extending from the vestibule (cleft between the labia minora) to the cervix of the uterus. It functions as a duct for menstrual fluid, a birth canal for delivery of the fetus, and is the female organ of copulation. It passes through the urogenital hiatus of the pelvic diaphragm and through the deep perineal pouch.
The anterior and posterior walls are normally in contact = the vagina is a collapsed tube.
The vaginal mucosa in premenopausal woman has a “corrugated”appearance due to many rugae that allow the vaginal walls to stretch. As estrogen declines in menopause, the mucosa smooths out.
The vagina is lined by a stratified squamous epithelium. The mucosa produces an acidic environment that may protect against pathogens.
The vagina attaches around the upper cervix—the lower cervix protrudes down into the vagina. Thus, the walls of the vagina encircle the cervix, producing anterior, posterior, and lateral cul-de-sacs called vaginal fornices. Due to the angle between the uterus and vagina, the posterior fornix is deepest. The fornices are supported by the cardinal and uterosacral ligaments.
Clinical correlation
The posterior vaginal fornix is adjacent to the recto-uterine pouch (of Douglas). In the upright position, the pouch is the lowest point in the peritoneal cavity, thus fluids can collect there. Abnormal contents in the pouch can be drained through an incision made in the posterior fornix (culdotomy). An endoscope can be placed in the peritoneal cavity through the posterior fornix (culdoscopy). Unsafe abortion procedures can perforate the posterior fornix and enter the peritoneal cavity. Incisions made in the vaginal fornices are part of a vaginal hysterectomy procedure.
The uterine and vaginal arteries supply the upper 80%. The lower part of the vagina near the introitus is supplied by the internal pudendal artery in the perineum.
Venous drainage: Uterovaginal venous plexus drains to the internal iliac veins.
Upper 80% drains along the uterine artery to the internal iliac nodes; lower 20% drains with other perineal structures to the superficial inguinal nodes.
The upper 80% is visceral in nature. Sympathetics probably supply blood vessels and may cause contraction of smooth muscle during orgasm. The function of parasympathetic innervation is not clear, but may cause glandular secretion. Afferents follow the pelvic splanchnic nerves to sacral spinal cord segments. They probably carry stretch information.
The lower 20% is somatic in nature. Somatic afferents carrying touch, pain, and temperature travel with the pudendal nerves to S-2, S-3, and S-4 spinal cord segments.
Uterus
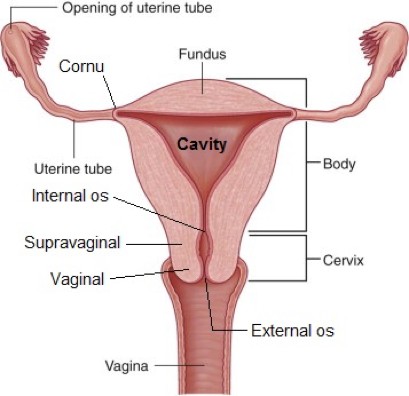
Figure 20.12 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.52.
The uterus is a thick-walled, hollow, muscular organ shaped like an upside-down pear. The uterus is the organ of gestation—specialized for reception, implantation, retention, and nutrition of the conceptus. The smooth muscle in the uterus contracts to expel the fetus in childbirth.
The upper 2/3 of the uterus is the body, with the head or dome of the body referred to as the fundus. Clinicians palpate the position of the fundus in pregnant women to estimate the age of the fetus. The space inside the body is the uterine cavity.
Lateral to the fundus are the cornua (Latin = “horns”) where the uterine (fallopian) tubes and round ligaments attach.
The cervix (Latin = “neck”) is the lower 1/3 of the uterus. Its upper part is above the attachment of the vagina, so it is referred to as supravaginal. The lower part that protrudes into the vaginal canal is the vaginal portion. The cervical canal connects the vaginal canal to the uterine cavity. It has two openings.
The internal os opens into the cavity of the uterine body; the external os communicates with the vagina.
Within the cervical canal is a plug of mucus that changes viscosity during the menstrual cycle to either prevent or allow the entry of sperm.
The uterus is in the center of the pelvic cavity, between the bladder and rectum. The vesico-uterine and recto-uterine pouches are located anterior and posterior to the uterus, respectively.
The body of the uterus is superior to the bladder. Loops of small bowel lie superior to the uterus. Therefore, the uterus has vesical and intestinal surfaces.
Parametrium: Outermost, composed of visceral pelvic fascia.
Myometrium: Middle layer, thick smooth muscle, branches of the uterine vessels are in this layer.
Endometrium: Inner layer, mucous membrane with uterine glands.Undergoes monthly renewal and degeneration—being cyclically prepared by hormones for implantation of the embryo.
Clinical correlation
Benign tumors of the uterine smooth muscle are called uterine fibroids or leiomyomas. They can be suspected on pelvic exam but are best confirmed with ultrasound. Some fibroids can be very large. Surgical management requires careful consideration of the anatomic structures adjacent to the uterus that could be distorted with fibroid growth.
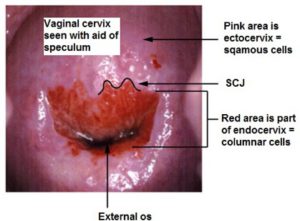
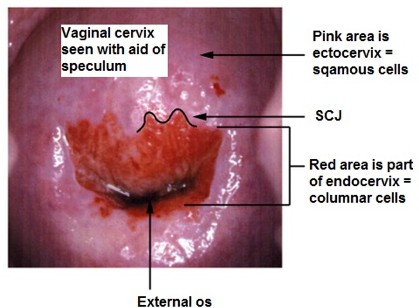
Figure 20.13 UPTODATE.
The cervical canal inside the external os is lined by columnar epithelium. Clinicians call it the endocervix.
The vaginal part of the cervix that can be seen with the aid of a speculum is lined by a stratified squamous epithelium (as is the vagina). Clinicians call this part of the cervix the ectocervix.
Near the external os is the squamocolumnar junction (SCJ), where the epithelia of the endocervix and ectocervix meet. Rapid turnover of cells occurs here. The SCJ is an important clinical landmark since most cervical cancers occur here. A Pap smear is a technique for sampling of cells in the region of the SCJ.
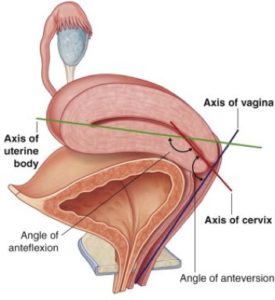
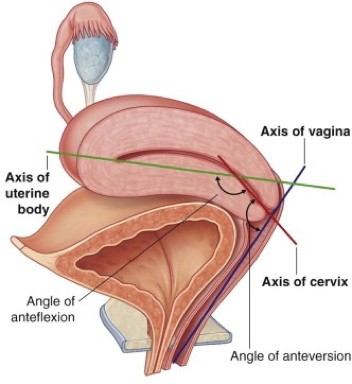
Figure 20.14 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.54.
The typical orientation of the uterus is described as anteflexed and anteverted. Flexion refers to orientation of the uterine body with respect to the uterine cervix. Version refers to the orientation of the entire uterus compared to the vagina.
When anteflexed, the body of the uterus is bent anteriorly upon the cervix.
When anteverted, the entire uterus is tilted forward on the vaginal canal—the uterus and vagina thus have a profile shaped like the number “7” in a lateral view.
Clinical correlation
Perhaps 20% of women have a uterus that tilts posteriorly (retroversion). This can be a consequence of development, previous pregnancies, or due to conditions such as fibroids. Judging the orientation of the uterus is an important part of the bimanual exam performed by clinicians. For example, failure to adjust for a greatly anteflexedor retroverted uterus when inserting an intra-uterine device (IUD) could result in uterine trauma or perforation.
Figure 20.15 NETTER, COLLECTION OF MEDICAL ILLUSTRATIONS: REPRODUCTIVE SYSTEM, PLATE 8-13.
Figure 20.16 Bimanual exam of anteverted uterus. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE B3.18.
Uterine arteries branch from the internal iliac arteries and reach the uterus in the cardinal ligaments. They ascend along the uterine body to anastomose with the ovarian artery.
Venous drainage: Via uterovaginal venous plexus to internal iliac veins.
The precise role of autonomic innervation on myometrial activity is not clear. It is known that uterine smooth muscle cells possess both adrenergic and cholinergic receptors. Studies have shown that most autonomic nerve fibers supply the cervix.
Sympathetic: Vasomotor to blood vessels and may cause contraction of smooth muscle during labor and delivery.
Afferent: The body and fundus are covered in peritoneum, so they are at the pelvic pain line. Pain from distension follows sympathetic routes upwards to lower thoracic and upper lumbar spinal cord levels. This is most likely the explanation for referred pain to the lower back during labor. Afferents from the cervix are below the pain line—they follow pelvic splanchnic nerves to sacral spinal cord segments. Pain due to stretch of the cervix refers to the perineum.
Clinical correlation
Hysterectomy is surgical removal of the uterus. Abdominal hysterectomy (also called open hysterectomy) is done via an incision in the lower abdominal wall.
Vaginal hysterectomy removes the uterus through the vagina. Robotic-assisted laparoscopic hysterectomy is removal of the uterus through the vagina with the aid of a robotic platform that views the pelvic cavity through scopes inserted through small openings in the abdominal wall. Regardless of the method, knowledge of anatomic relationships is vital. Ligation or clamping of the uterine artery must be done with care to avoid injuring the nearby ureter, which passes just below (remember—the water runs under the bridge!).
Clinical correlation
Afferents from the uterus and vagina conduct pain during labor and delivery. They project to a large number of spinal cord segments: T-10 to L-2 for body and fundus of uterus, S-2 to S-4 for cervix (pelvic splanchnic nerves = visceral) and perineum (pudendal nerve = somatic).
Different options for anesthesia/analgesia target different pathways. An epidural is a local anesthetic delivered to the epidural space through a catheter in the lower back.
It blocks lower thoracic and upper lumbar spinal nerves to relieve uterine referred pain. A pudendal nerve block (described in The Perineum) numbs the lower vagina and perineum.
Uterine tubes (fallopian tubes)
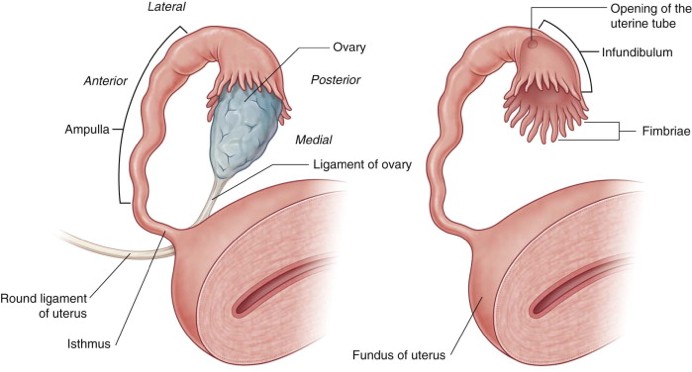
Figure 20.17 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.53.
The uterine (fallopian) tubes connect the uterine cavity with the peritoneal cavity (yes—you heard that right). They function to provide a place for sperm and ovum to meet and a route for the fertilized zygote to reach the uterine cavity. They are about 10cm long and have named portions that will be described from distal to proximal. Since the ovaries are posterior to the uterus, the uterine tubes curl backwards.
Infundibulum: The funnel-shaped distal expansion of the tube. It has an ostium at the bottom of its stem that leads into the next portion, the ampulla. The circumscribed edge of the funnel contains 20 to 30 fronds called fimbriae. These drape over the ovary and sweep the ovum into the infundibulum after it has been ovulated.
The ampulla is the wide, slightly tortuous central portion—it makes up about half the tube length. This is normally where fertilization occurs.
The isthmus is the narrow, medial 1/3 of the tube. It attaches to the cornu of the uterus.
Inside the uterine wall, an intramural section connects the isthmus to the uterine cavity.
The uterine tubes contain smooth muscle that produces peristaltic contractions to move the ovum (or zygote) toward the uterus. Their mucosa has a ciliated epithelium that beats toward the uterus.
The uterine tubes receive both sympathetic and parasympathetic nerve fibers, but their exact functions are not well understood. Ciliary activity, muscular contractility, and tubal fluid flow are complicated processes that probably rely on both endocrine signals and ANS innervation and possibly cues from the ovum and zygote as well.
Sympathetic input is from lower thoracic and lumbar splanchnic nerves =it is vasomotor and may increase ciliary and muscular activity.
Pelvic splanchnic nerves supply parasympathetic fibers. They probably have little impact on functioning of uterine tubes.
Afferent: The uterine tubes are intraperitoneal, so they are above the pelvic pain line. Afferents enter the lower thoracic and upper lumbar spinal cord segments.
Clinical correlation
Sexually transmitted infections (chlamydia, for example), abdominal infections, or surgical procedures can damage the fallopian tubes. The resultant scarring can block the tubes or affect their motility, leading to fertility issues or ectopic pregnancy (the fallopian tubes are the most common site for this).
Ovaries
The female gonad, the ovaries are almond-shaped structures lying against the lateral pelvic walls. Their primary functions are to produce ova and the hormones estrogen and progesterone. Before the first ovulation, the ovary is smooth and pink. Thereafter, the surface becomes pitted and distorted due to the scarring of repeated ovulations.
Ovarian nerve plexus originates from the aortic plexus and descends with the ovarian vessels. It contains both sympathetic and parasympathetic fibers who functions are not entirely known. Ovarian function does not depend on motor nerve supply.
Afferent: The ovaries are peritoneal, so they are above the pelvic pain line. Pain follows sympathetic routes retrograde to the lower thoracic and upper lumbar spinal cord segments.
Question
Some women experience pain at ovulation (called Mittelschmerz: German = middle pain, since it occurs mid-way between periods). This may be due to rupture of an ovarian follicle, smooth muscle spasm, or irritation of nearby peritoneum.The pain is often referred to the umbilical region or to one side of the body over the iliac fossa (presumably corresponding to the side of the body where ovulation occurs).
What dermatome levels are these?
Ligament support of female internal genitalia
Peritoneal ligaments
Vestigal fibrous ligaments
Fibromuscular ligaments
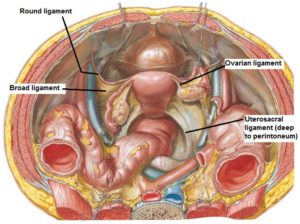
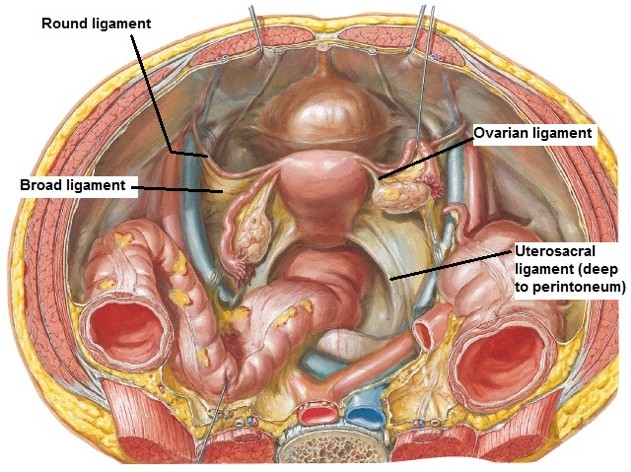
Figure 20.20 Contents of broad ligament. GRANT’S ATLAS OF ANATOMY, FIGURE 5.33.
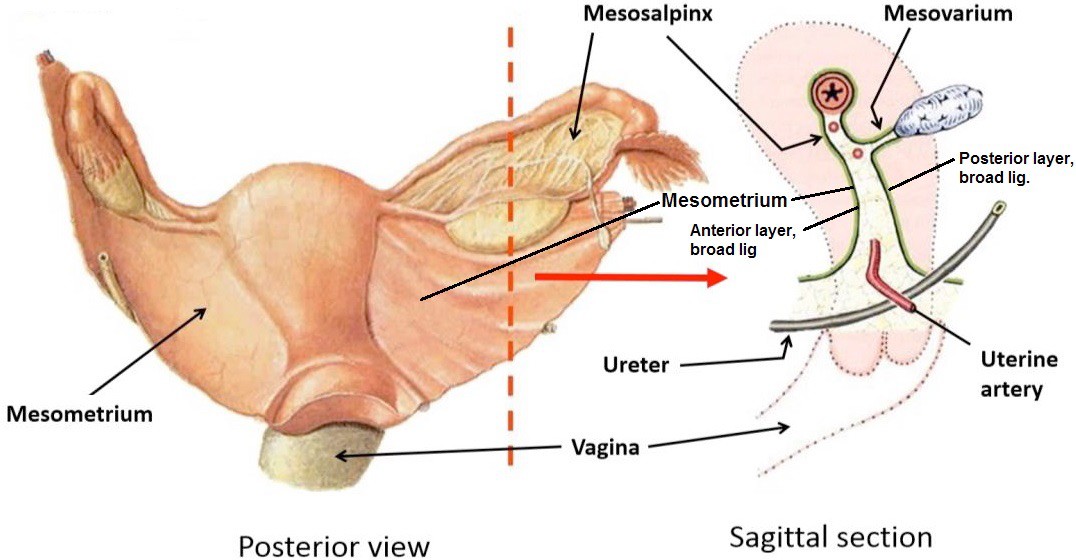
Broad ligament: Double-layer of peritoneum that drapes over the uterus and uterine tubes. Has anterior and posterior layers and three subparts that are continuous with one another:
Mesometrium: Extends laterally from the margin of the uterine body to the pelvic wall.
Mesosalpinx (salpingo: Greek = trumpet): Drapes over the uterine tubes.
Mesovarium: Extends backwards from the mesosalpinx to the anterior border of the ovary.
Contents: The broad ligament is pitched like a tent over the uterus and uterine tubes, and these structures: ovarian ligament (uterus to ovary), round ligament of uterus, cardinal ligament, uterine vessels, and the terminal part of the ureters.
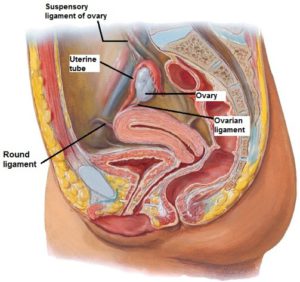
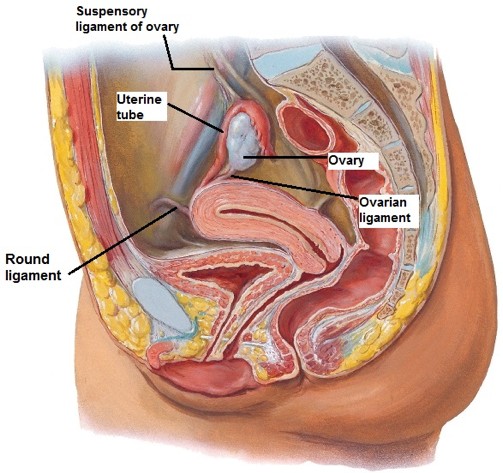
Superiorly and laterally, above the ovaries, the broad ligament continues onto the pelvic brim where it contains the ovarian vessels and is named the suspensory ligament of the ovary (infudibulopelvic ligament). Note that the suspensory ligament is NOT the same thing as the proper ovarian ligament, despite having similar names.
Figure 20.21 Contents of broad ligament. GRANT’S ATLAS OF ANATOMY, FIGURE 5.33.
Round ligaments of uterus. Connect the uterine cornua to connective tissue in the labia majora via the inguinal canals. Stabilize the uterus and may help maintain it in anteflexion. Enlarges during pregnancy and can cause pain in the groin region due to traction exerted by the growing uterus.
Ovarian ligaments (proper ovarian ligaments): Connect ovary to uterine cornu. Continuous with round ligament at the cornu.
Both ligaments are remnants of the embryonic ovarian gubernaculum.
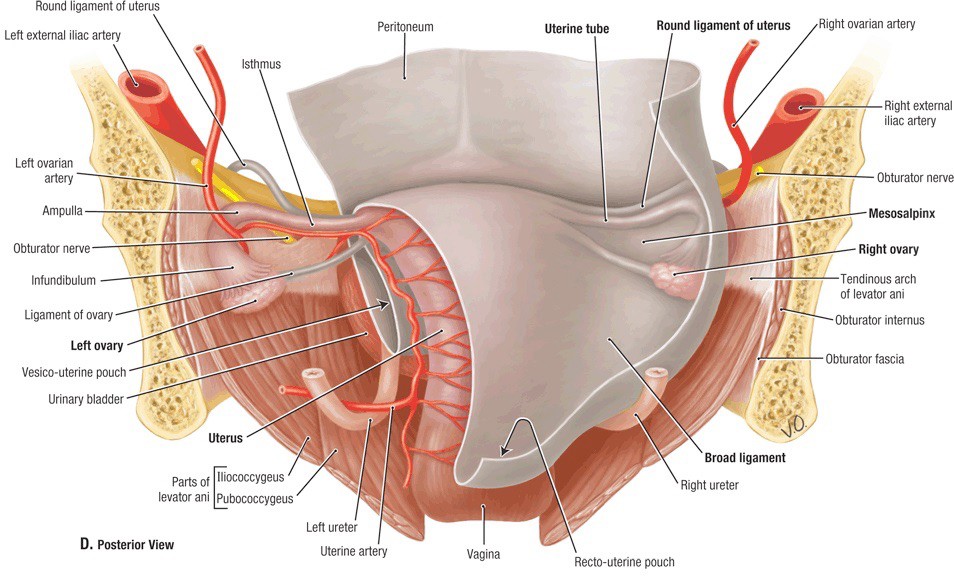
Figure 20.22 Superior view with peritoneum removed. NETTER, ATLAS OF HUMAN ANATOMY, PLATE 343.
The anteverted position of the uterus is important to its support as it allows it to rest on the bladder. The cervix is the least supported part of the uterus, so it is attached to these ligaments:
Cardinal ligaments (lateral cervical ligaments): Thought to be the major support of the uterus, especially the cervix. Prevents prolapse and also supports the vagina, uterine arteries and terminal parts of ureters.
Uterosacral ligaments: Pass posteriorly from the cervix to the mid-sacrum.
Male internal genitalia
Prostate
Figure 20.23 NETTER, ATLAS OF HUMAN ANATOMY, PLATE 344.
A firm, elastic exocrine gland composed of smooth muscle and fibroglandular tissue—about the size of a walnut. The prostate produces a milky, alkaline fluid that makes up about one-third of the semen. Prostatic fluid contains enzymes that enhance sperm motility, liquefy semen (prostate specific antigen—PSA) and gives semen its characteristic odor. Muscular contraction of the prostate squeezes prostatic fluid from its glands into the prostatic urethra prior to ejaculation.
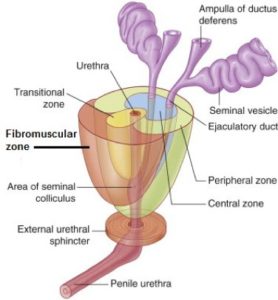
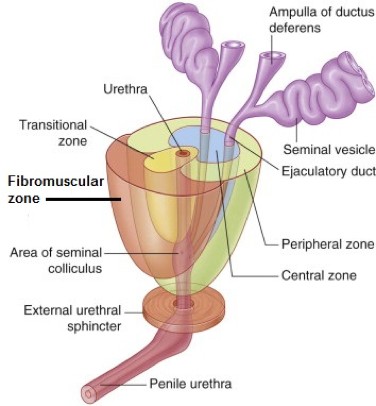
Figure 20.24 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.47.
This can be confusing, since anatomists and urologists use different terms, and they are often mixed and matched. The passage of the urethra and ejaculatory ducts through the prostate divides it into anatomic lobes and clinical zones.
Anterior lobe (isthmus) is anterior to the urethra—also known as the fibromuscular zone. There is no glandular tissue here.
Left and right lobes are lateral to the urethra and meet posteriorly in a shallow groove. These lobes together constitute the peripheral zone, the posterior portion of which is palpated in a rectal exam. This zone is the most common location of prostate cancer.
Median lobe is the tissue surrounding the ejaculatory ducts. Also called the central zone.
The transitional zone is sandwiched between the three zones just described. It encircles the urethra in the core of the prostate, below the bladder. This is the region affected by benign hyperplasia.
Venous drainage is to the prostatic venous plexus surrounding the prostate. The deep dorsal vein of the penis (draining the erectile tissue) is a tributary of this plexus. The plexus drains to the internal iliac veins.There are connections between the internal iliac veins and the vertebral column via valveless veins = a route for metastasis of prostate cancer to bone.
Sympathetic fibers from lumbar splanchnic nerves cause contraction of prostatic smooth muscle and secretion of prostatic fluid into the urethra during ejaculation. They also constrict the internal urethral orifice of the bladder to prevent retrograde passage of semen into the bladder. The function of parasympathetic innervation on the prostate is not clear.
An important subset of parasympathetic fibers derived from the pelvic splanchnic nerves passes directly adjacent to the prostate and through the deep perineal pouch to the erectile tissue of the penis. These tufts of fibers (left and right) are called the cavernous nerves. They produce tumescence and erection of the penis. Parasympathetic = point; Sympathetic = shoot.
Surgeons performing prostate surgery work hard to spare the cavernous nerves. Damage to these nerves can produce erectile dysfunction (impotence).
Afferent: The prostate is below the pelvic pain line, so visceral sensory fibers follow pelvic splanchnic nerves to S-2, S-3, and S-4 spinal cord levels. Pain from prostatitis is dull and throbbing and often felt in the perineum and lower back.
Clinical correlation
Prostatectomy is surgical removal of the prostate. It is done to treat early stage prostate cancer. Access to the prostate is often through the retropubic space, an extraperitoneal space between the bladder and pubic bones, filled with fat. Side effects of this surgery can be incontinence and impotence (= because of damage to the nearby cavernous nerves).
As men reach their mid-40s, the prostate begins to undergo benign growth in the transition zone. Continued growth can constrict the urethra and elevate the prostate into the bladder wall, causing enlargement of the bladder’s uvula. Common symptoms of BPH are weak urinary stream, hesitancy (waiting for voiding to begin), intermittency (stopping and starting of urine stream), a sensation of incomplete emptying, and nocturia (multiple voids during the night).
Examination of the prostate “per rectum”
Owing to the relationship of the prostate and rectum, only the rectal wall and a layer of connective tissue separate the clinician’s gloved finger from the prostate. This procedure is used to determine the size and texture of the prostate, including the presence of nodules indicative of cancer, which may prompt needle biopsy.
Enters the abdominopelvic cavity through the deep inguinal ring. It crosses over the external iliac vessels and pelvicbrim to enter the pelvic cavity, being subperitoneal throughout its pelvic course. Upon reaching the bladder’s base, the ductus crosses superior to the ureter and arches superior and then medial to the seminal vesicle.
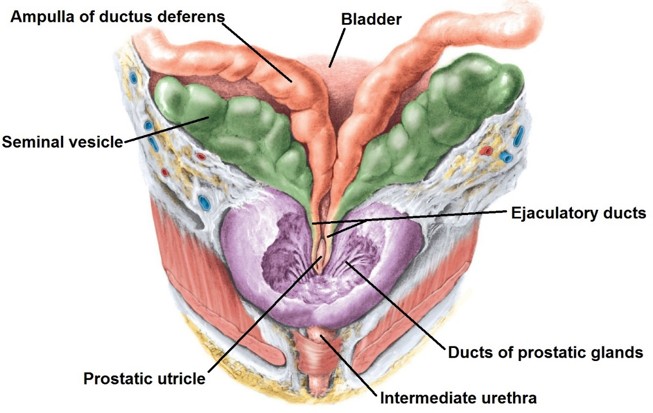
At the base of the bladder the ductus deferens widens to form the ampulla. Medially, this joins the duct of the seminalvesicle just above the base of the prostate to form the ejaculatory duct.
Richly supplied with sympathetic fibers derived from the pelvic plexus that signal peristaltic contraction of smooth muscle for expelling sperm during ejaculation.
Seminal vesicles
Each vesicle contains a tightly coiled tube with many diverticula and a blind-end, all bound together by connective tissue. Amazingly, if outstretched, the tube would reach about 15 cm! The epithelial cells lining the tube produce seminal fluid, which makes up about 70% of the semen ejaculated.
Their secretions play an important role in fertility by affecting maturation, mobility, and capacitation of sperm.
Seminal fluid contains enzymes that clot semen after ejaculation (so it forms a sticky glob to adhere to the uterine cervix) and then liquefy the clot so sperm can swim up the cervical canal (prostate secretions also help in liquefaction).
Seminal fluid contains fructose to nourish sperm (seminal vesicles are “sweet little things”!) and immunosuppressive factors to protect sperm from the female immune response.
Sympathetic fibers derived from the pelvic plexus cause contraction of its smooth muscle and secretion of seminal fluid.
Afferent fibers follow pelvic splanchnic nerves to S-2 through S-4 spinal cord levels.
Ejaculatory ducts
Thin tubes, each about 2 cm long, they enter the prostate at the base and pass through its core at an angle in an anteroinferior direction. Their terminal openings are located within the prostatic urethra, on the seminal colliculus on each side of the prostatic utricle.
Bulbo-urethral glands (Cowper’s glands)
Although these are not located in the male pelvis, they do contribute secretions to semen and like the internal genital organs are innervated by sympathetic fibers as part of the sexual response.
Pea-sized glands located in the deep perineal pouch (discussed in the Perineum section) posterolateral to the intermediate urethra, embedded in the external urethral sphincter. Their ducts penetrate the perineal membrane and open in the urethra within the bulb of the penis.
They secrete mucus upon sexual arousal to flush out urine residue and lubricate the urethra prior to ejaculation. Innervated by sympathetic fibers.
Figure 20.25 Posterior view. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE 3.36.
Figure 20.26 Anterior view. GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.44.