The pelvis is the region of transition where the trunk and lower limbs meet. Since the word pelvis comes from the Latin term for basin, it is used more precisely to describe a ring of bones (pelvic skeleton) and the space the bones surround (pelvic cavity).
Pelvic skeleton
Figure 19.1
Figure 19.2 Radiograph of a child’s acetabulum. Cartilage separates the bones of the pelvic skeleton. GILROY, ATLAS OF ANATOMY, FIGURE 19.3B.
The pelvic skeleton consists of the paired hip bones (coxal bones) and the sacrum.
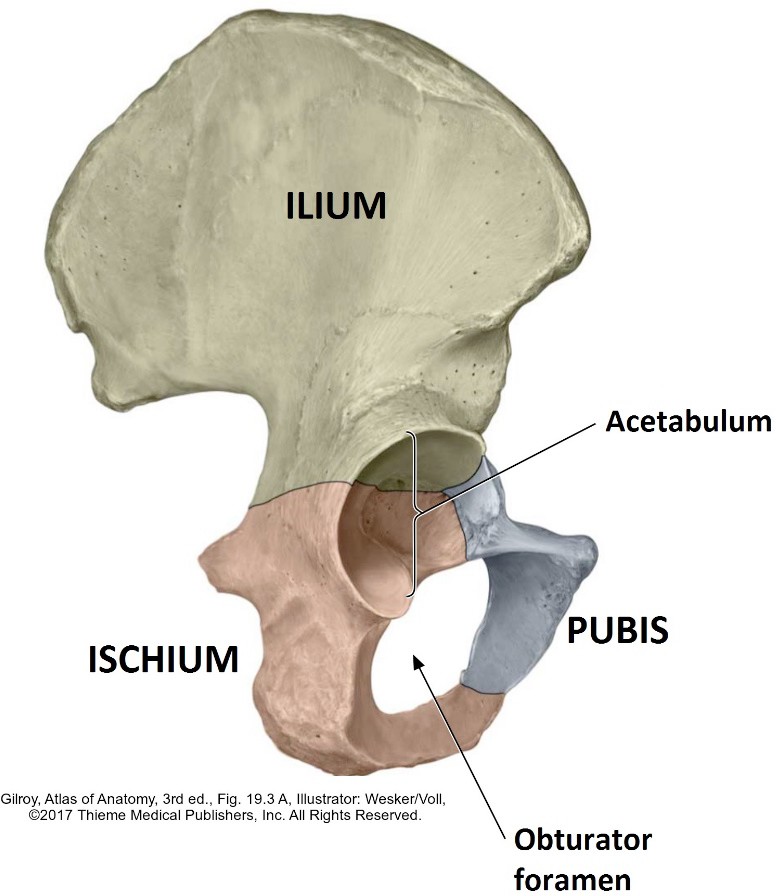
The hip bones are formed from three fused bones: the ilium, ischium, and pubis. All three bones meet at the acetabulum, the deep, cup-shaped cavity that contributes the “socket” to the ball-and-socket hip joint. The ilium, ischium, and pubis don’t completely fuse until after puberty. Prior to this, the bones are joined together by a Y-shaped cartilage (tri-radiate cartilage), located in the acetabulum.
The hip bones are joined together anteriorly by the symphysis pubis, a joint with ligaments and a fibrocartilage disc.
Posteriorly, the hip bones are joined to the sacrum by the stout left and right sacro-iliac joints.
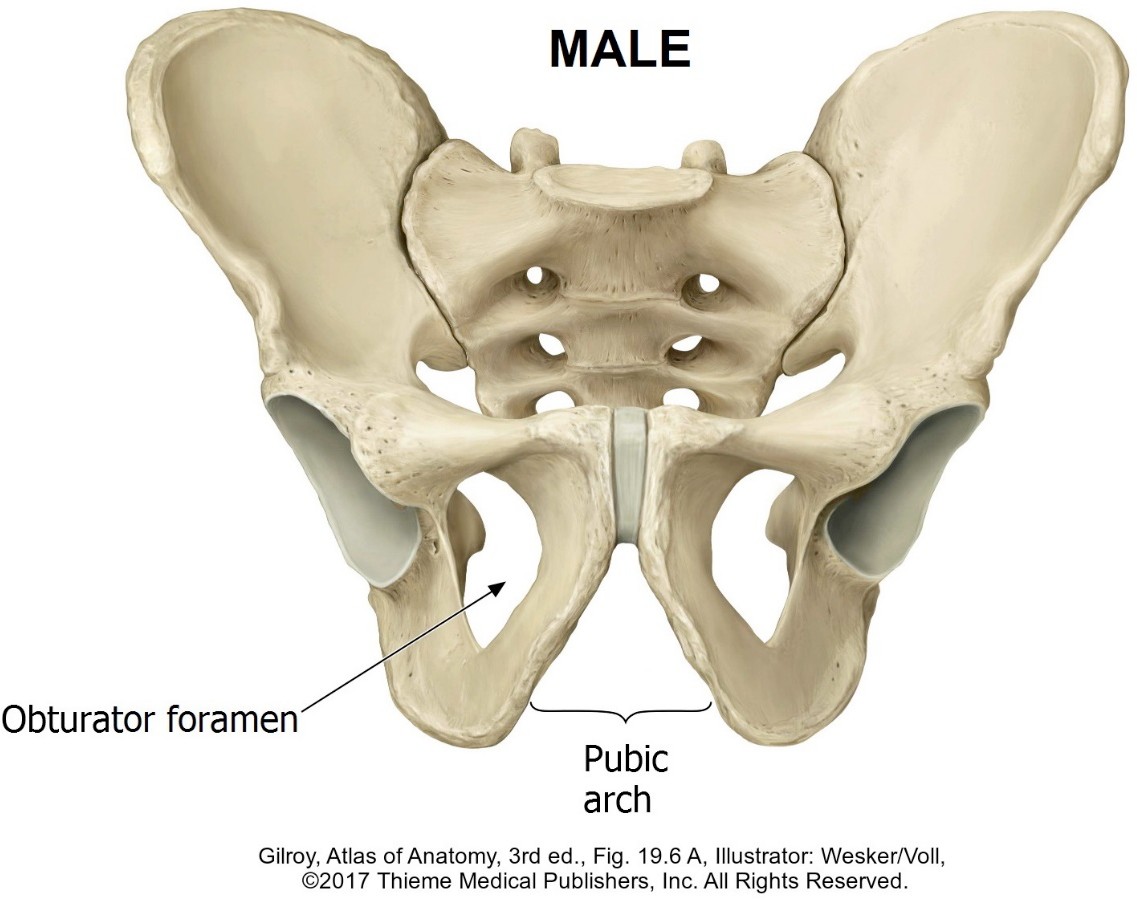
In the dried hip bone, the obturator foramen is prominent anteriorly between the inferior and superior pubic rami. In the living person, this opening is almost completely covered by a membrane (obturator = Latin: “closed”). A small obturator canal opens in the membrane, allowing the obturator nerve and vessels to pass from the pelvic cavity into the thigh.
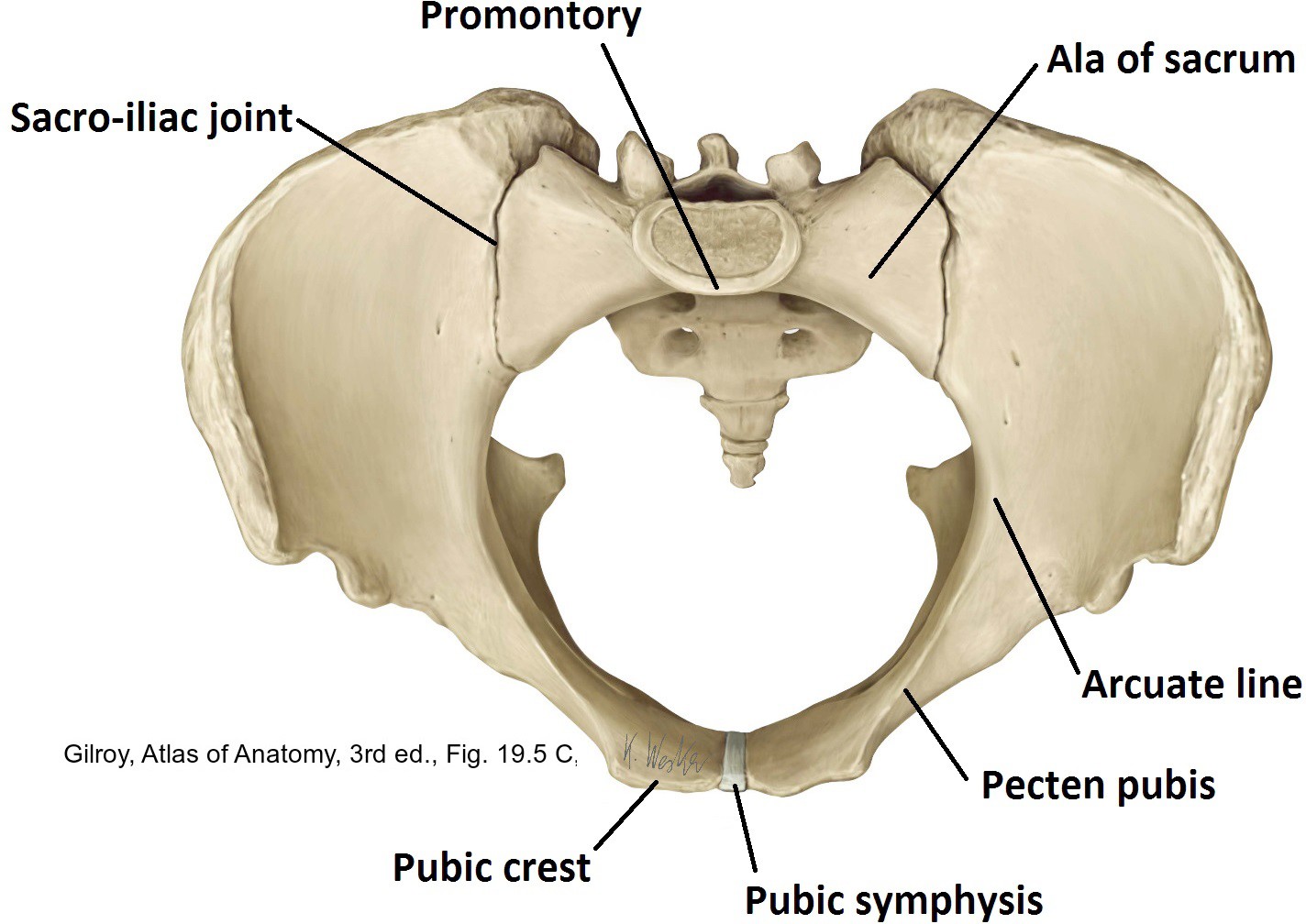
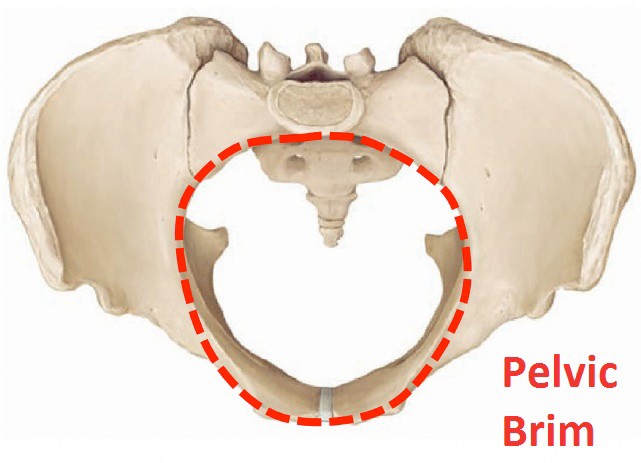
The pelvic brim is the boundary between the so-called true pelvis (pelvis minor) and false pelvis (pelvis major). The brim is formed bilaterally by the pubic crest, pecten pubis, arcuate line of the ilium, and ala of the sacrum, and in the midline by the sacral promontory posteriorly and the symphysis pubis anteriorly. It is an important landmark that we refer to often, so it is worth getting to know.
Figure 19.3
Figure 19.4 GILROY, ATLAS OF ANATOMY, 3RD ED., FIGURE 19.5C.
True or false (pelvis, that is)
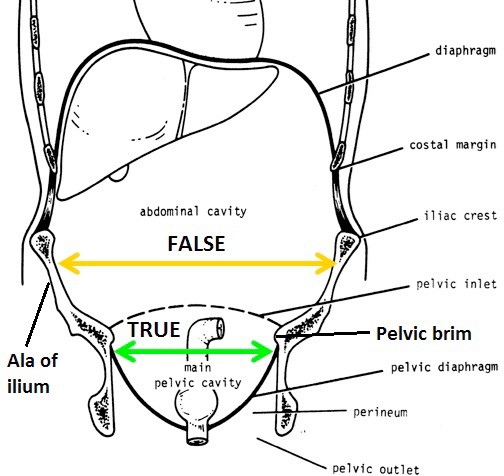
The true pelvis is the area inferior to the pelvic brim between the pubic bones anteriorly and the sacrum posteriorly. The true pelvis houses the pelvic cavity and pelvic viscera.
The false pelvis is the region above the pelvic brim between the alae of the iliac bones (the “wings”). In reality, it contributes to the boundary of the abdominal cavity, and supports abdominal organs like the cecum and sigmoid colon, so it has nothing to do with the pelvic cavity or pelvic viscera, thus the term “false” is applied.
Figure 19.5 SNELL, CLINICAL ANATOMY BY REGIONS, FIGURE 7.1.
Pelvic apertures: The upper and lower boundaries of the true pelvis
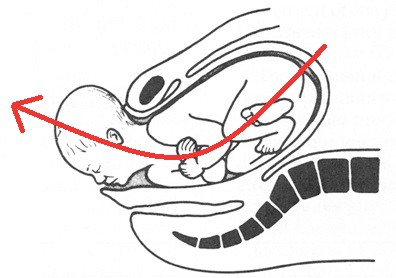
The superior pelvic aperture (pelvic inlet) is somewhat oval and defined by the pelvic brim. The ureters, sigmoid colon, internal iliac vessels, ductus deferentes in the male, and other nerves and vessels pass between abdominal cavity and pelvic cavity through the inlet. The pelvic inlet is important in the later stages of pregnancy when the fetus descends into the pelvic cavity before labor ensues—a process called “engagement” of the fetus.
Figure 19.6 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.32.
Figure 19.7 MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE 3.8.
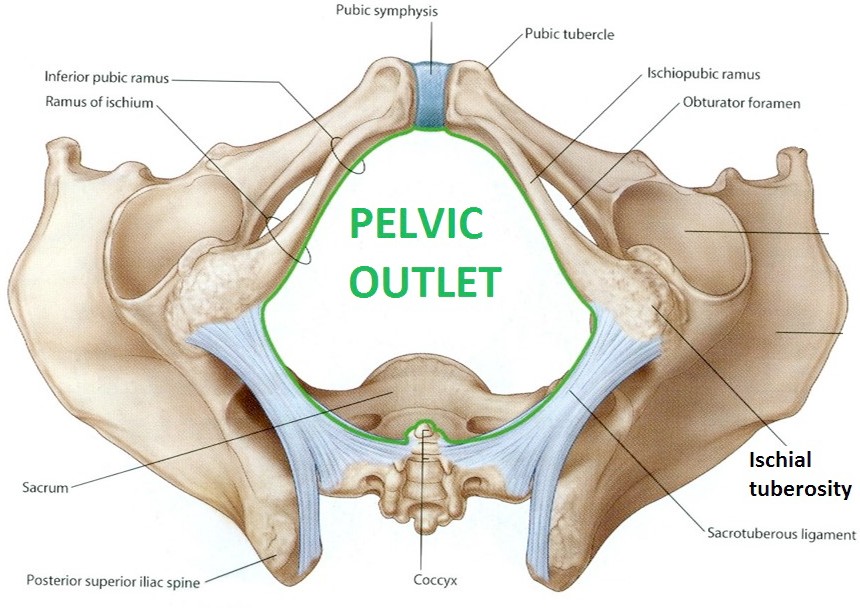
The inferior pelvic aperture (pelvic outlet) is diamond-shaped and bounded by the pubic symphysis, ischiopubic rami, ischial tuberosities, sacrotuberous ligaments, and the coccyx. Note that the pelvic outlet defines the inferior-most extent of the true pelvis—but not the inferior-most extent of the pelvic cavity. The pelvic diaphragm (muscle) defines the floor of the pelvic cavity. The boundaries just described for the pelvic outlet are inferior to the pelvic diaphragm. Thus, the pelvic outlet is actually outside the pelvic cavity, in a region called the perineum. Delivery of the fetus takes place through the pelvic outlet via the vagina.
Orientation of the pelvic skeleton
Figure 19.8 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.26.
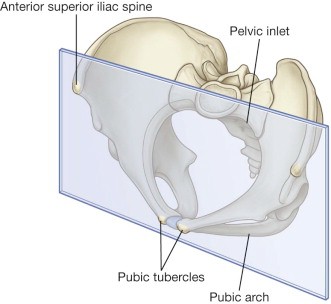
In the anatomical position, the pelvic skeleton does not produce an upright basin, as the name implies. Instead, the pelvic skeleton is tilted anteriorly about 50–60 degrees, such that the pubic tubercles and the anterior superior iliac spines are in the same vertical plane. Indeed, it is possible for a lean person to place their pelvic region against a wall and have all four bony points (left and right) touch the wall. Try it—tell curious onlookers that you are a medical student demonstrating pelvic anatomy!
Consequences of the “pelvic tilt”
The pelvic inlet faces anterior and superior—the outlet faces posterior and inferior.
The axis of the true pelvis is curved, with concavity directed anterior. It is therefore not a “straight shot” for delivery of the fetus during childbirth.
Figure 19.9 SNELL, CLINICAL ANATOMY BY REGIONS, FIGURE 6.16.
Sexual dimorphism in the pelvic skeleton
The pelvic skeletons of females and males differ in several ways, mainly due to the heavier, stronger muscles in males and the adaptations in the female for childbearing.
Male pelvic skeleton
The male pelvic skeleton is thicker and has more prominent bony markings, including everted ischiopubic rami for the attachment of the penis.
When viewed from above, in the male, the sacral promontory juts into the inlet, making it heart-shaped.
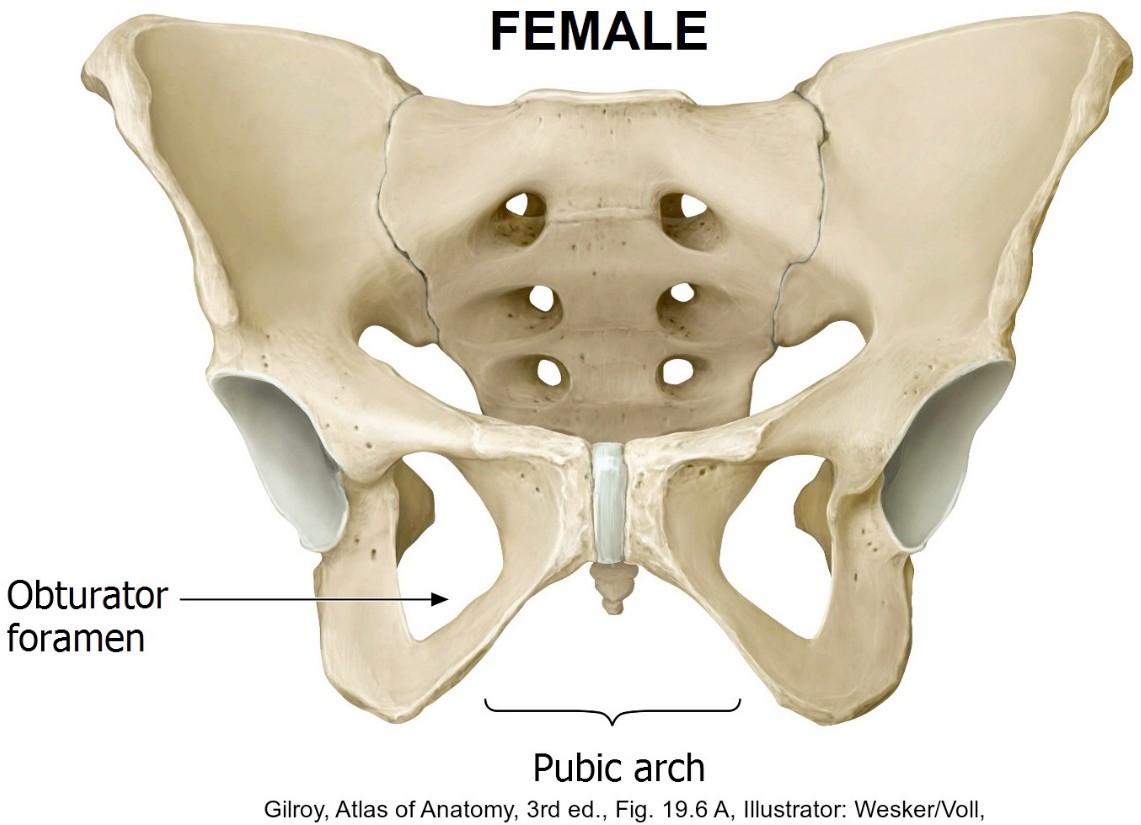
Female pelvic skeleton
The female pelvic skeleton is wider, shallower, and has larger superior and inferior apertures. As a result, the sacrum is shorter and wider, causing the hip bones to be farther apart. This explains why females generally have wider hips.
When viewed from above, the female superior aperture (pelvic inlet) is oval.
Figure 19.10
Figure 19.11
Consequences of the “pelvic tilt”
The pubic arch in the female measures about 90 degrees, while in the male it forms a narrow angle (around 70 degrees or less). Consequently, the ischial tuberosities are farther apart in females than in males.
Clinical correlation
In forensics, the characteristics of the bony pelvis are indicators of gender.
Clinical correlation
The size and shape of the female pelvic skeleton have importance in obstetrics. Pelvic cavity capacity and width of the pelvic outlet are larger in females, an adaptation for childbirth. Measurements of the parts of the pelvic skeleton internally, via vaginal examination, is called pelvimetry.
Ligaments associated with the pelvic skeleton
Figure 19.12
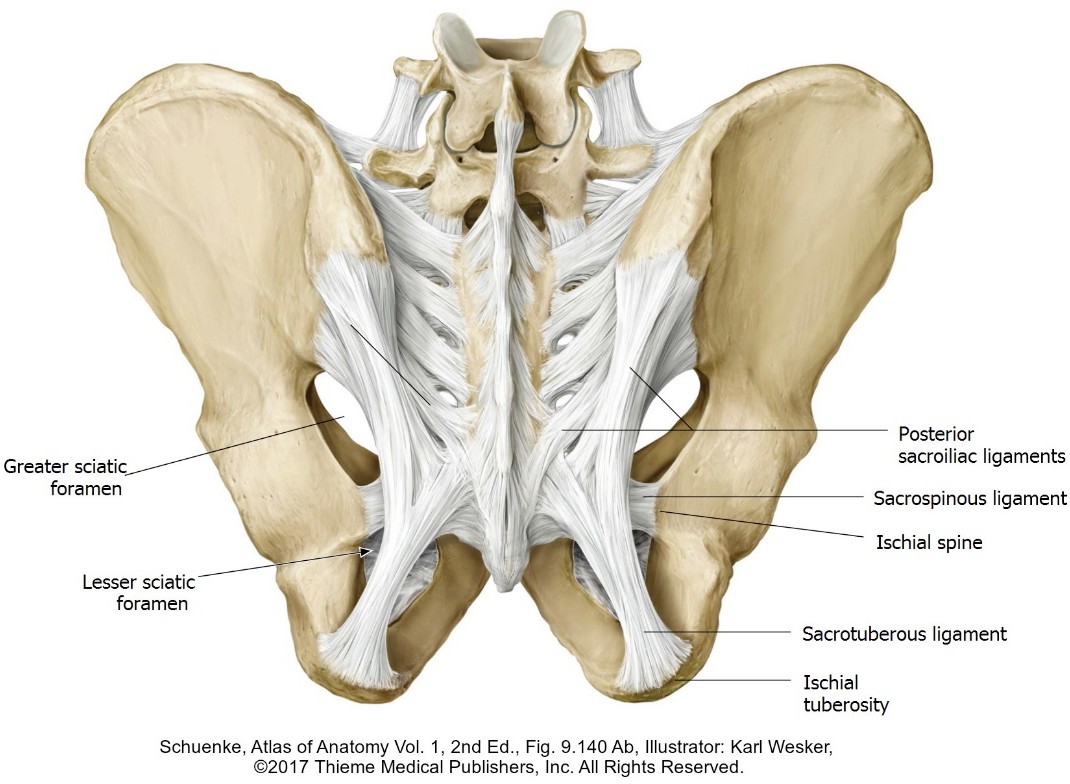
Figure 19.13
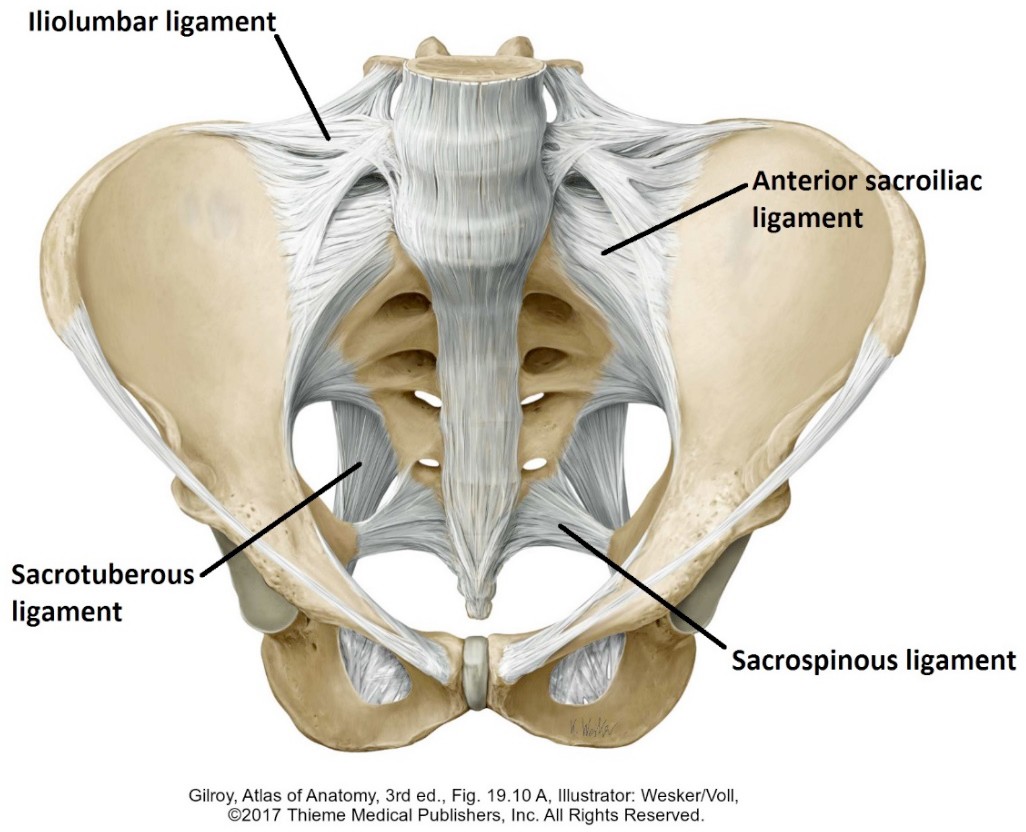
Sacrotuberous ligament
Sacrospinous ligament
Broad origin from the coccyx, sacrum, and the posterior superior iliac spine—inserts into the ischial tuberosity.
Extends from the inferior sacrum to the ischial spine—deep to the sacrotuberous ligament.
The sacrospinous and sacrotuberous ligaments are thought to prevent posterior rotation of the sacrum due to the upper body’s weight pressing down.
Sacro-iliac ligaments
Pubic symphysis
Reinforce the large sacro-iliac joints. They restrict movement of the sacrum and iliac bones as the weight of the trunk pushes the sacrum downward like a wedge between the two hip bones.
A strong joint consisting of a fibrocartilage disc joining together the symphyseal surfaces of the pubic bones. Ligaments above and below the disc reinforce the joint.
The ligaments described above, as well as the pubic symphysis, soften and relax during pregnancy owing to the hormone relaxin (secreted by the ovaries). This allows them to be stretched and somewhat mobile during pregnancy and delivery.
Question
What are the differences between the greater and lesser sciatic notches, on the one hand, and the greater and lesser sciatic foramina, on the other?
Pelvic cavity
Recall that the abdominal and pelvic cavities are continuous, forming a large abdominopelvic cavity. The bony pelvic brim demarcates the junction of the abdominal and pelvic portions, with the pelvic cavity being below the brim.
Notwithstanding the internal genitalia and the bony pelvic differences, the basic anatomy of the pelvic cavity is similar in both sexes.
Boundaries of the pelvic cavity
Anterior: Mainly bone = the bodies of the pubic bones and the pubic symphysis.
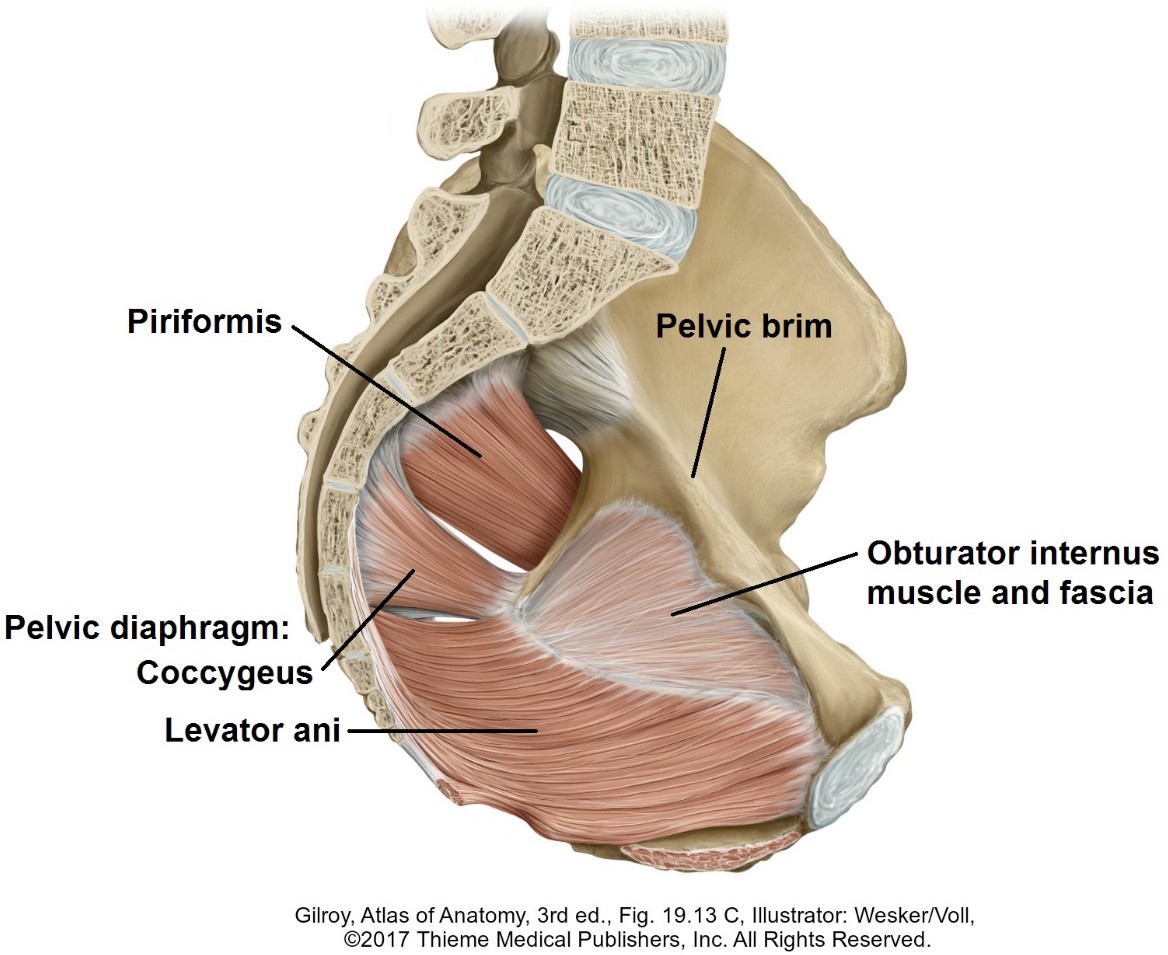
Posterior: Sacrum and piriformis muscles.
Lateral: Obturator internus muscles; posterolaterally are the greater sciatic foramina, filled with vessels, nerves, and the piriformis muscles.
Inferior: The pelvic diaphragm—a composite muscle sloping downward,from lateral to medial.
Superior: Open; communicates with the abdominal cavity above.
remember
The pelvic cavity is contained within the true pelvis, but does not share the same boundaries as the true pelvis (the pelvic cavity is like a sac—open at the top and placed within a larger box = the true pelvis). The inferior boundary of the pelvic cavity (pelvic diaphragm) is located above the inferior boundary of the true pelvis (the pelvic outlet).
Muscles associated with the pelvic cavity
Figure 19.14 GRAY’S ATLAS OF ANATOMY, PAGE 212.
A handy way to describe the skeletal muscles associated with the pelvic cavity is to divide them into two groups: those confined to the walls of the pelvic cavity and those of the pelvic floor. Functionally, this makes sense, too.
Muscles of the pelvic walls
Although these muscles originate from the pelvic walls, their actions produce movements of the lower limb= lateral (external) rotation of the hip.
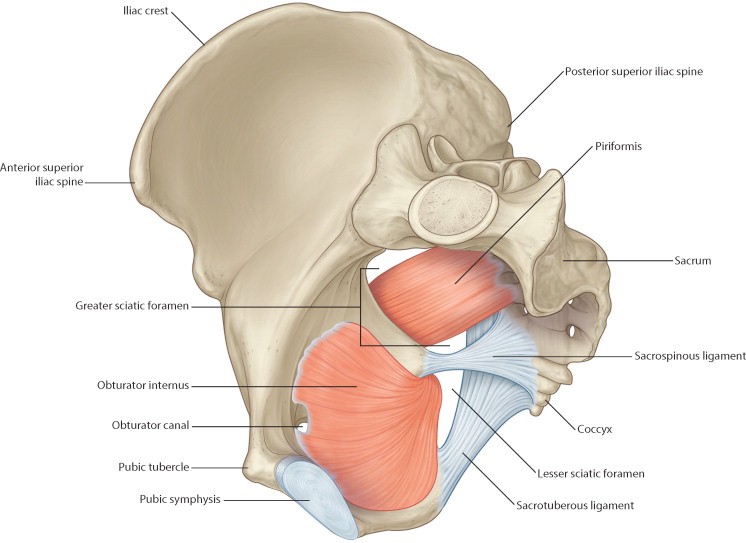
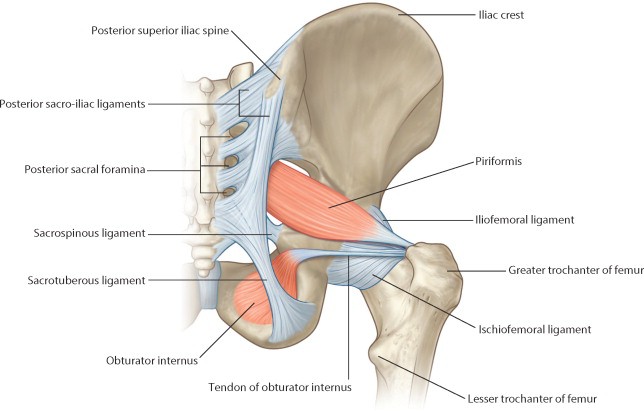
The name describes its appearance = “pear-shaped.” The piriformis originates from the pelvic surface of the sacrum. It tapers as it passes laterally to exit the pelvic cavity through the greater sciatic foramen. The piriformis is a useful landmark when describing the positions of nerves and vessels leaving the pelvic cavity through the greater sciatic foramen (example = the superior gluteal artery passes above the piriformis; the inferior gluteal artery below). The piriformis forms part of the posterior pelvic wall and here it provides a muscular “bed” for the anterior rami of sacral spinal nerves (that form the sacral plexus) to rest upon. Note that the two piriformis muscles don’t touch at their origins—they leave a gap of bare sacral bone in the posterior pelvic wall (BOTH anterior and posterior pelvic walls have bare bone).
The tendon of the piriformis attaches to the greater trochanter of the femur—its contraction rotates the femur outward = lateral (external) rotation.
This hefty muscle originates from the entire anterolateral bony wall of the pelvic cavity and from the internal surface of the obturator membrane. It has an odd shape and odd course— resembling a “fan” with a tendon that makes a 90-degree turn as it leaves the pelvic cavity. The fibers of obturator internus taper down to a thick tendon that leaves the pelvic cavity through the lesser sciatic foramen—turning around the bony margin of the lesser sciatic notch like a rope through a pulley. Like the piriformis, obturator internus inserts on the greater trochanter and is a lateral rotator of the femur at the hip joint.
Note
The piriformis and obturator internus muscles are innervated by ventral rami of sacral spinal nerves.
Muscles in the floor of the pelvic cavity
The pelvic diaphragm forms the fibromuscular pelvic floor. The diaphragm is a paired, composite structure composed of two muscles on each side:
Levator ani
Coccygeus
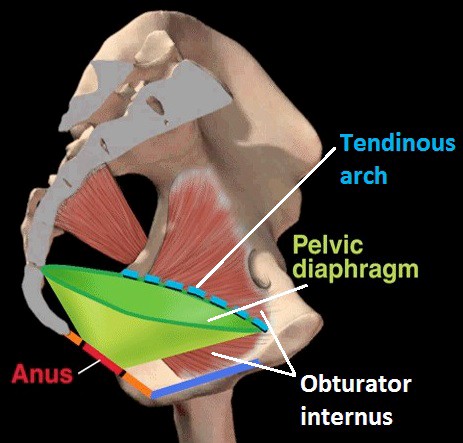
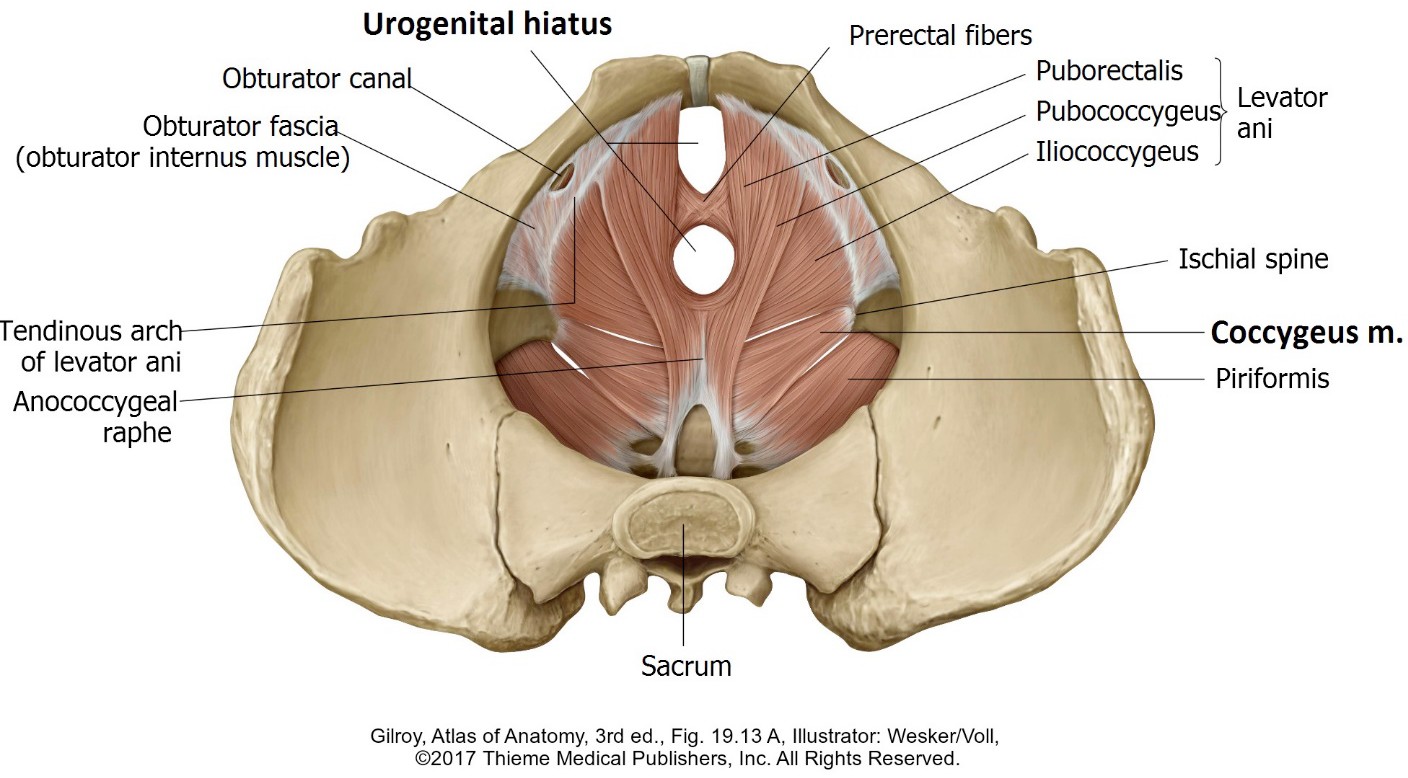
The pelvic diaphragm can be modeled by placing a funnel inside the pelvic cavity. The circular edge of the funnel fits snugly as it wedges up against the pubic bones, the obturator internus muscles, the ischial spines and the sacrum. The pelvic diaphragm slopes inferiorly from these points of origin toward the midline of the pelvic cavity. Here there is a gap in the center of the diaphragm, the urogenital hiatus, that allows the urethra, vagina, and anal canal to leave the pelvic cavity and enter the perineum (the tip of the funnel represents this gap).
As a whole, these muscles (left and right) make up the largest and most important portion of the pelvic diaphragm. The levator ani has a broad origin—stretching from the body of the pubis to the ischial spine. Between these two bony attachments, the fibers of the levator ani originate from an arched thickened band of pelvic fascia on the pelvic surface of the obturator internus called the tendinous arch of the levator ani.
The fibers of the levator ani slope both posteriorly and downward toward the midline to insert into the:
Perineal body, a fibromuscular wedge of tissue that projects upwards from the perineum into the urogenital hiatus
Walls of the organs passing through the urogenital hiatus
Anococcygeal ligament (raphé)
Coccyx.
Figure 19.18
For descriptive purposes, three parts of the levator ani are named—although they are quite difficult to discern in the cadaver (you will need to consult one of the models in lab) and may not function independently.
Pubococcygeus is the largest component of the levator ani. It originates from the body of the pubis and slopes downward and backward to insert into the anococcygeal ligament and coccyx. This muscle borders the urogenital hiatus. In the female, part of the pubococcygeus sweeps posterior to the vagina to insert into the perineal body, and may be important in urinary continence since it also relates to the urethra. The posterior fibers of the pubococcygeus meet in a fibrous midline raphé that runs from the anal canal to the tip of the coccyx = the anococcygeal ligament.
Iliococcygeus is the thinnest part of the levator ani. It arises from the tendinous arch and the ischial spine and slopes medial and posterior to insert into the anococcygeal ligament and coccyx.
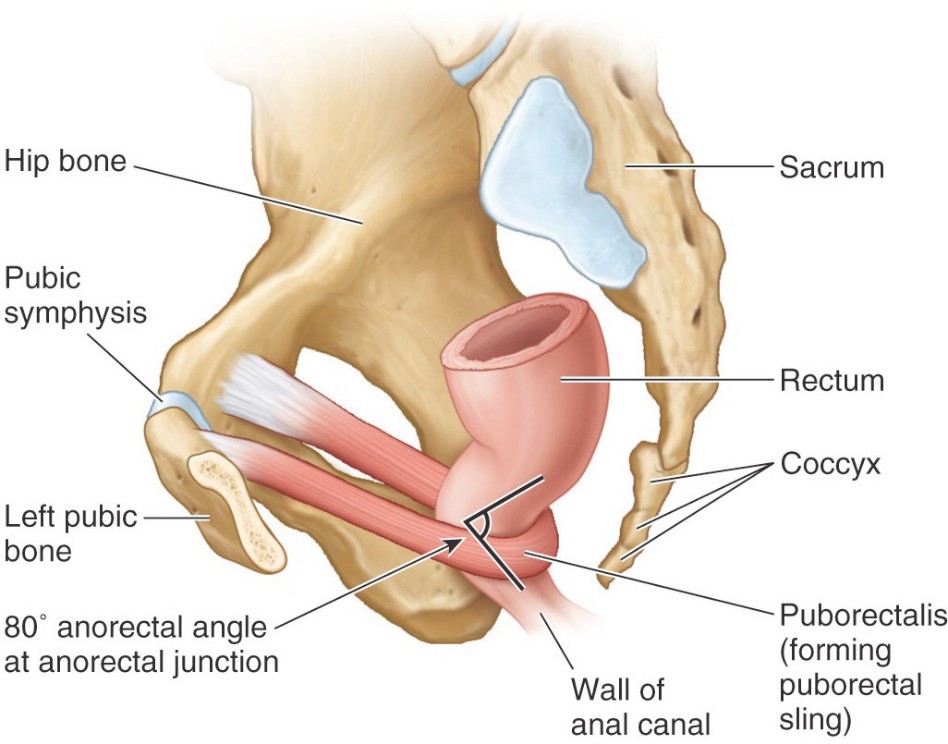
Figure 19.19 MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE 3.12.Puborectalis forms the thickest and most inferior part of the levator ani. It is best seen on the inferior (perineal) surface of the pelvic diaphragm—consult the models in lab. The fibers of the puborectalis originate from the body of the pubis and pass posteriorly. Instead of inserting into the coccyx, the fibers loop around the junction of the rectum and anal canal to join its partner from the other side, effectively forming a muscular “sling” around the anorectal junction. The puborectalis is responsible for the posterior-facing orientation of the anal canal as it angles away from the anterior-facing rectum. This change of direction in the gut tube is the anorectal flexure. Contraction of the puborectalis tightens the sling around the anorectal junction, constricting its lumen. This “pinching” action regulates the size of the feces passed during defecation and is useful for resisting the passage of feces when it is not desired (or until the next highway rest stop). Volitional control of the puborectalis is therefore necessary for maintaining fecal continence.
Coccygeus muscles
These unimportant muscles arise from the ischial spines and fan out to insert into the lateral borders of the coccyx and lower sacrum. They are the most posterior and thinnest parts of the pelvic diaphragm. On their external surfaces the coccygeus muscles fuse with the sacrospinous ligaments.
The pelvic diaphragm is supplied by sacral spinal nerves S-4 and S-5; via direct branches of the ventral rami to its pelvic surface, and via the inferior anal nerve (a branch of the pudendal nerve) to its perineal surface.
What’s the big to-do over the pelvic diaphragm?
Plenty. The pelvic diaphragm is a super-important muscle mass with plenty of clinical considerations:
1
The pelvic diaphragm is in a state of tonic contraction, especially when we stand upright. This supports the pelvic viscera.
2
When intra-abdominal pressure is raised by the action of abdominal wall muscles, contraction of the pelvic diaphragm is increased to resist the inferior push on the pelvic floor. The process of “bearing down” = raising intra-abdominal pressure by taking a deep breath, holding it in, and contracting the abdominal muscles, is called a Valsalva maneuver. It is necessary for carrying out such important and sometimes unpleasant activities as coughing, vomiting (emesis), defecating, and steadying the trunk so that the upper limbs can lift heavy objects.
3
When the pelvic diaphragm fails to support pelvic organs, the uterus and urinary bladder are at risk for prolapse (“falling” of an organ, especially if the organ drops through an orifice like the vagina or anus).
4
Contraction of the pelvic diaphragm helps constrict the urethra and anal canal (puborectalis—described earlier), so it is important for urinary and fecal continence.
5
During the early stages of labor, contraction of the pelvic diaphragm is not productive, so prenatal exercises are recommended for helping the pregnant women consciously relax her pelvic diaphragm. In the end stages of labor, contraction of the pelvic diaphragm (“pushing”) is desirable to expel the fetus from the vagina.
Clinical correlation
As you can see, having a well- conditioned pelvic diaphragm is important. So-called Kegel exercises have been advocated for women (and men) as a means of strengthening the pelvic diaphragm and avoiding organ prolapse and incontinence (fecal and urinary).
Pelvic fascia
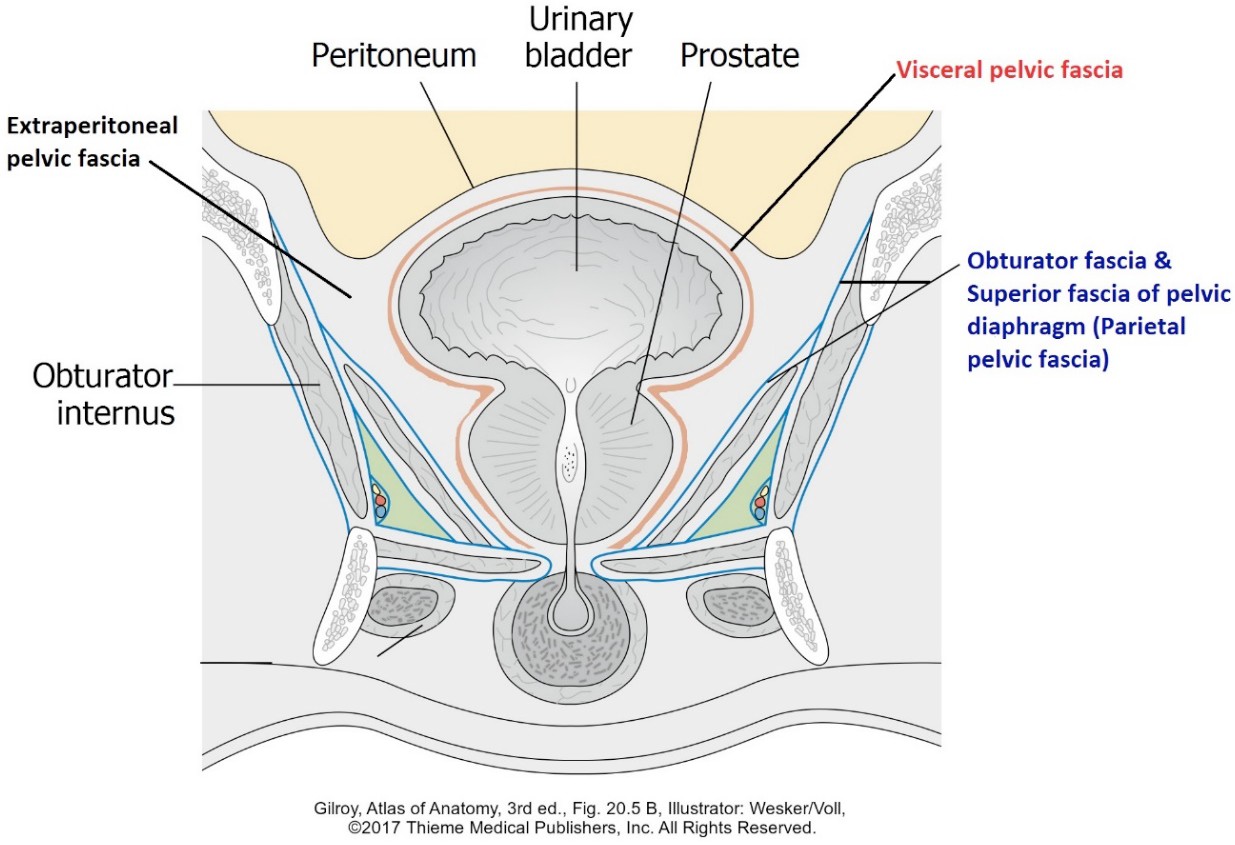
For descriptive and functional purposes, pelvic fascia is organized into three parts:
Parietal pelvic fascia
Visceral pelvic fascia
Extraperitoneal pelvic fascia
Parietal pelvic fascia (endopelvic fascia) is the internal fascia (described in the very first session of this course) of the pelvic cavity—a part of the overall membranous fascia that lines the inner aspect of the abdominal and pelvic walls. It is comparable to the endothoracic fascia in the chest wall.
Parietal pelvic fascia adheres to muscles in the walls and floor of the pelvic cavity. It is incomplete anteriorly and posteriorly as it fuses to theperiosteum of the pubis and sacrum. The named parts of the parietal pelvic fascia are obturator fascia and the superior fascia of the pelvic diaphragm.
The junction of the superior fascia of the pelvic diaphragm with the obturator fascia produces a thickened, curved line of fascia that runs from the body of the pubis to the ischial spine, known as the tendinous arch of the levator ani. A good portion of the levator ani muscle originates here.
Figure 19.20
Visceral pelvic fascia is loose connective tissue that forms tubes around pelvic organs—urinary bladder, rectum, uterus, prostate, and vagina. Except for the prostatic fascia in the male, visceral pelvic fascia is“stretchy”—allowing organs to distend. Parietal pelvic fascia and visceral pelvic fascia are continuous at the urogenital hiatus.
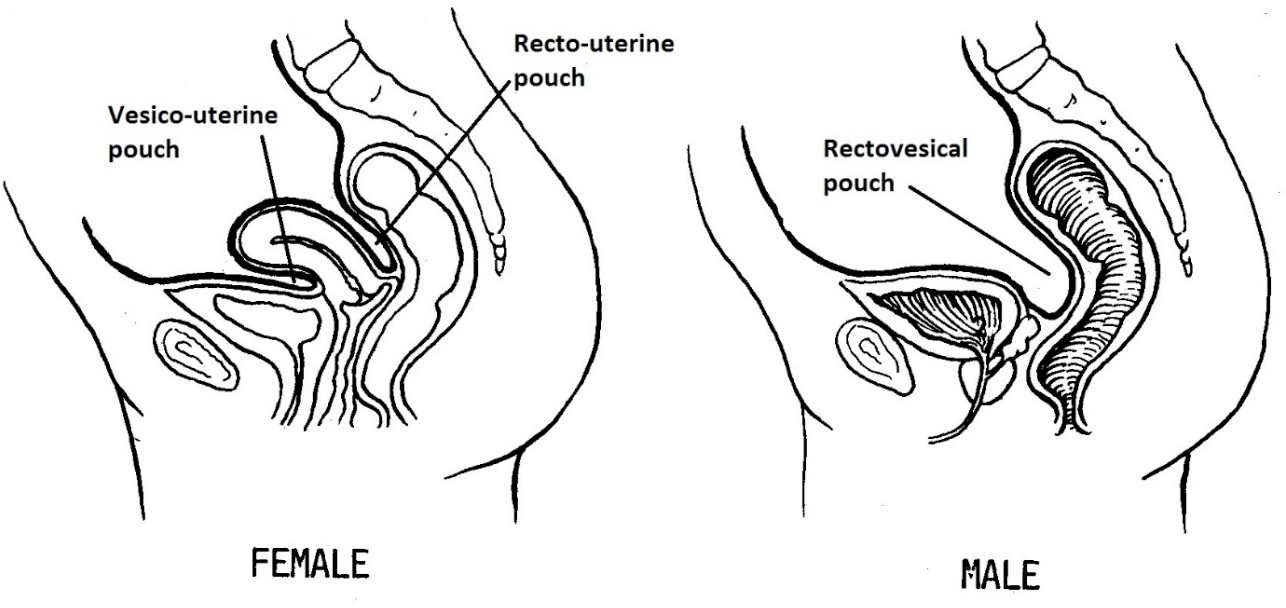
The peritoneum passes inferiorly into the pelvic cavity and drapes like a sheet over the urinary bladder and rectum in the male, and the bladder, rectum, and uterus in the female, fusing with the visceral pelvic fascia where it touches these organs.
Between the organs, the peritoneum dips down further, but does not reach the pelvic floor. These peritoneal indentations are the vesico-uterine and recto- uterine pouches in the female, and the rectovesical pouch in the male.
Pouches have clinical importance as we shall see later, since they are the most inferior extensions of the peritoneal cavity and thus can filled with blood or other fluids under pathologic conditions.
Extraperitoneal (subperitoneal) pelvic fascia is “packing material” that fills the space between parietal pelvic fascia on the walls of the pelvic cavity, visceral pelvic fascia on the organs, and the peritoneum draped over the organs. An analogy—let’s say you order an expensive vase from a fancy-pants store in the mall. It comes in a box filled with Styrofoam pellets.The box represents the walls of the pelvic cavity, the vase is a pelvic organ, and the pellets are the subperitoneal pelvic fascia. It is the equivalent of extraperitoneal fatty fascia (pararenal fat) that is so abundant around the kidneys in the posterior abdominal wall.
Fascial “ligaments”
Figure 19.21
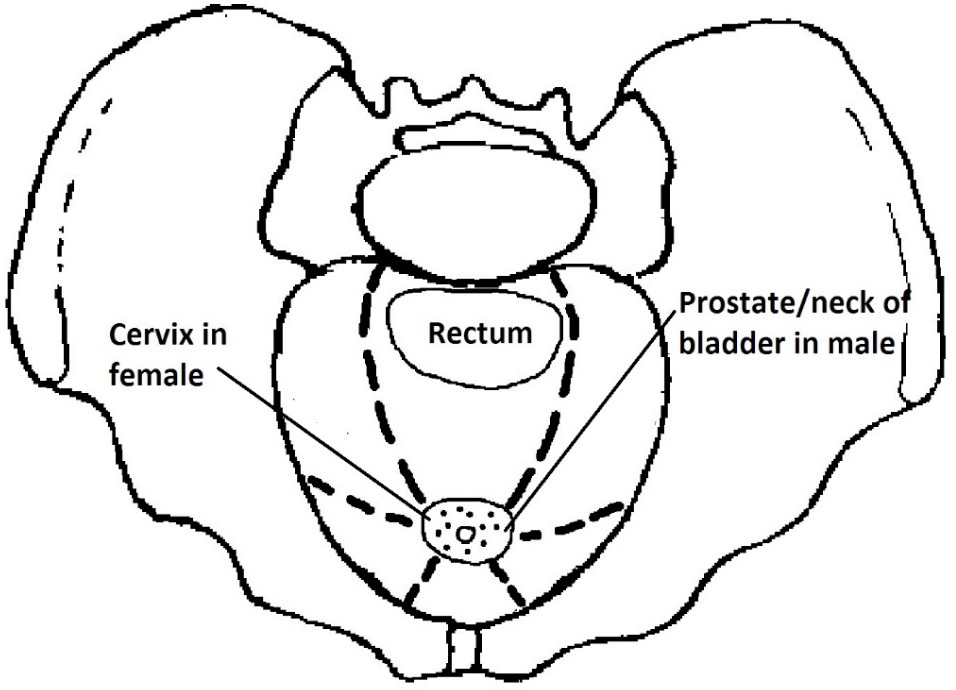
Condensations of the extraperitoneal pelvic fascia form sheaths around blood vessels and nerves that travel from the pelvic wall to the pelvic viscera—acting as supports or conduits. These are described in textbooks as pelvic fascial ligaments. They are extremely difficult to identify in the cadaver, yet they have important clinical relevance. The best way to visualize and describe these ligaments is to imagine them as spokes of a wheel, radiating away from a central “hub” in the pelvic cavity outward toward the pelvic walls. The ligaments connect visceral fascia around the organs with parietal fascia on the pelvic walls.
In the female, the “hub” of the fascial ligaments is the uterine cervix.
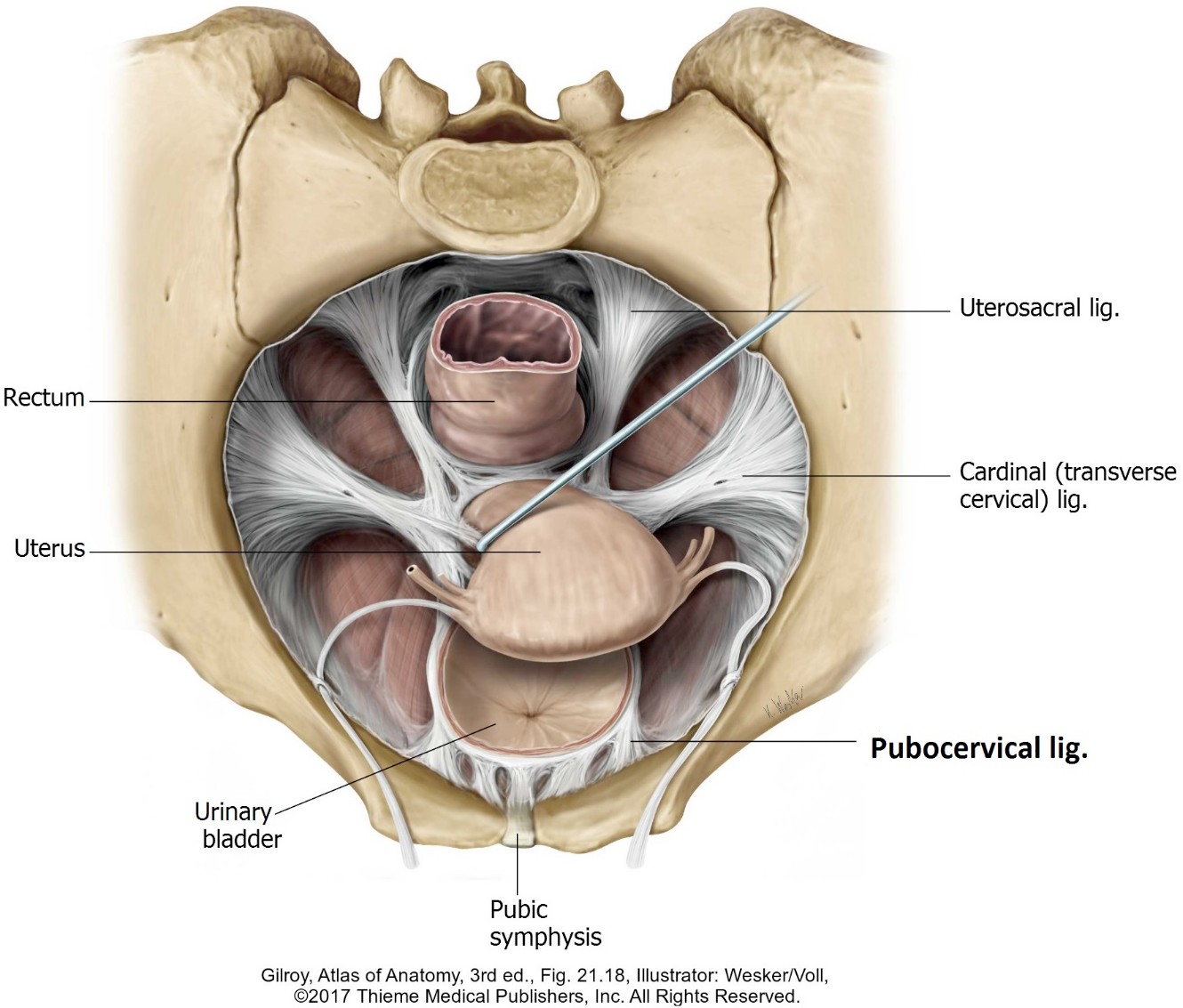
The named ligaments are:
Pubocervical
Cardinal ligament (lateral cervical ligament or Mackenrodt’s ligament) impress the surgeons with this eponym, but don’t forget its real name!
Uterosacral ligament
In the male, the “hub” of the fascial ligaments is the prostate and neck of the bladder.
The ligaments are not as important in males as in females, so we won’t name them.
Figure 19.22 HAND-DRAWN CONLEY- GRAM.
Figure 19.23
Clinical correlation
The cardinal ligaments (named presumably for their purported importance) support the uterine arteries and ureters. The integrity of these ligaments is thought to be of importance in supporting the uterus, too. Weakening of the pelvic diaphragm and cardinal ligaments can lead to prolapse of the uterus (protrusion of the uterus through the pelvic floor into the vagina). Repair of prolapse may involve "cinching up" the ligaments so that they are more taut.