

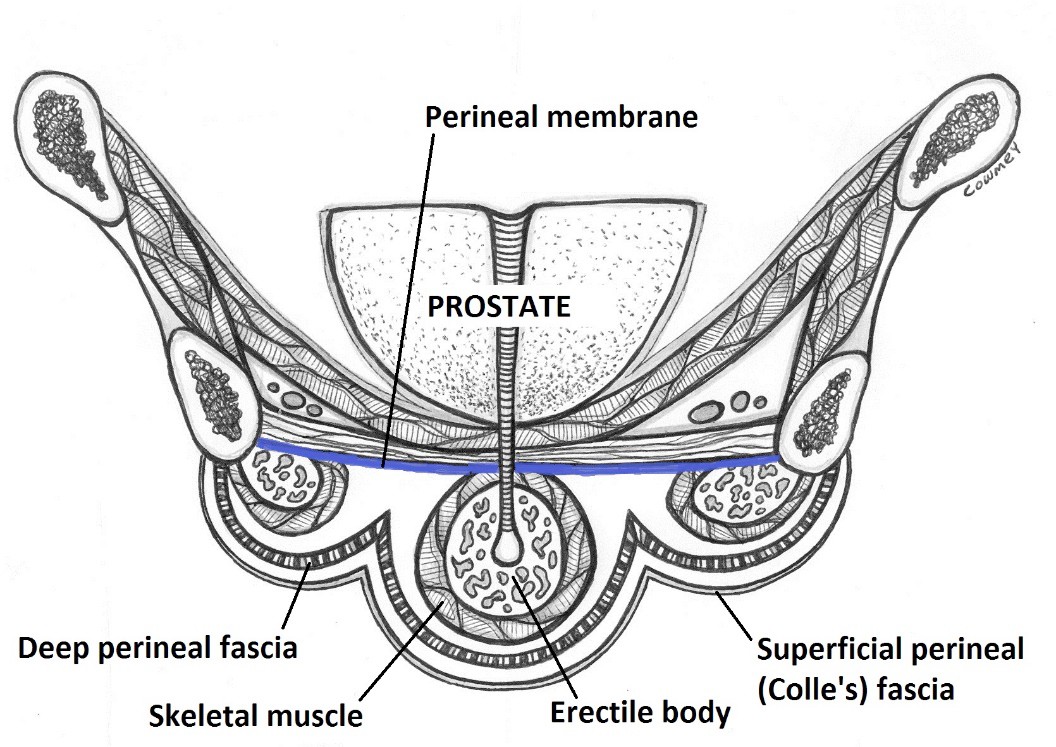


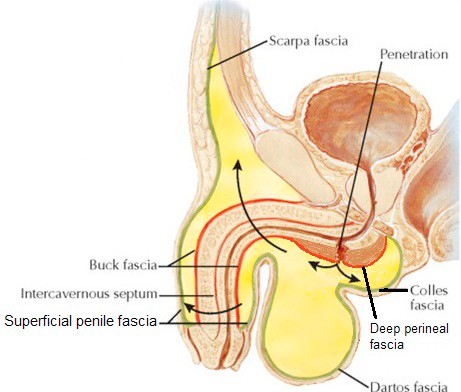
Likewise, damaged blood vessels can bleed into this space. Thus, urine or blood could collect in the penis and scrotum and pass superiorly into the abdominal wall if the volume is large enough. Do you see how?

Blood supply
Blood supply is via the deep and dorsal arteries of the clitoris, terminal branches of the internal pudendal arteries. Venous drainage is via dorsal veins of the clitoris.
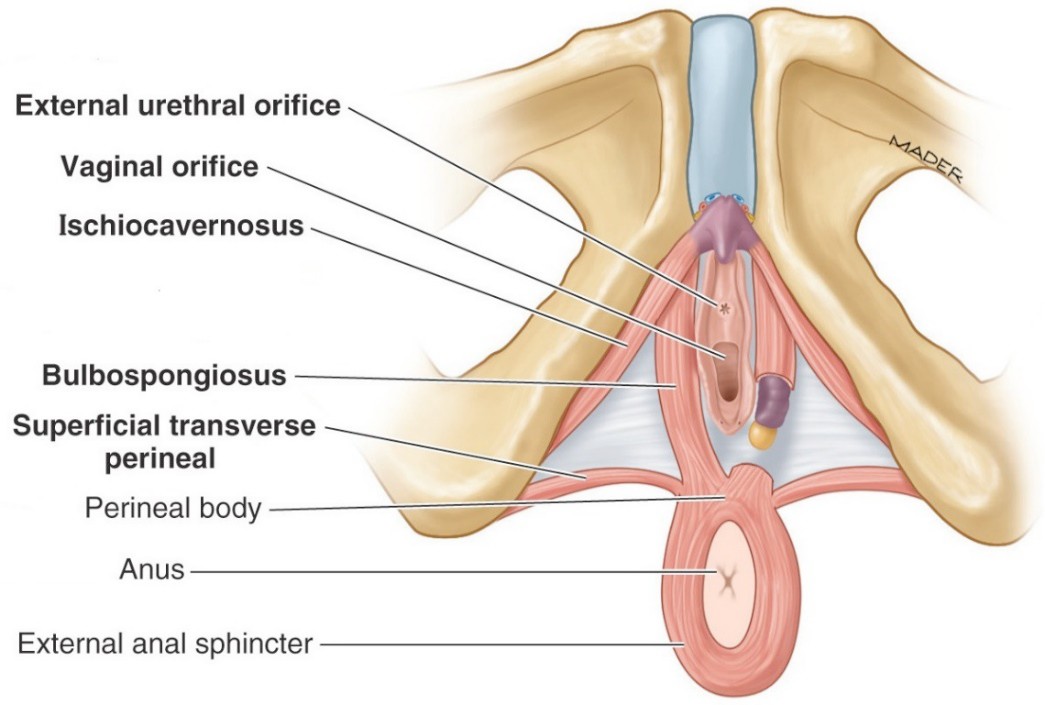
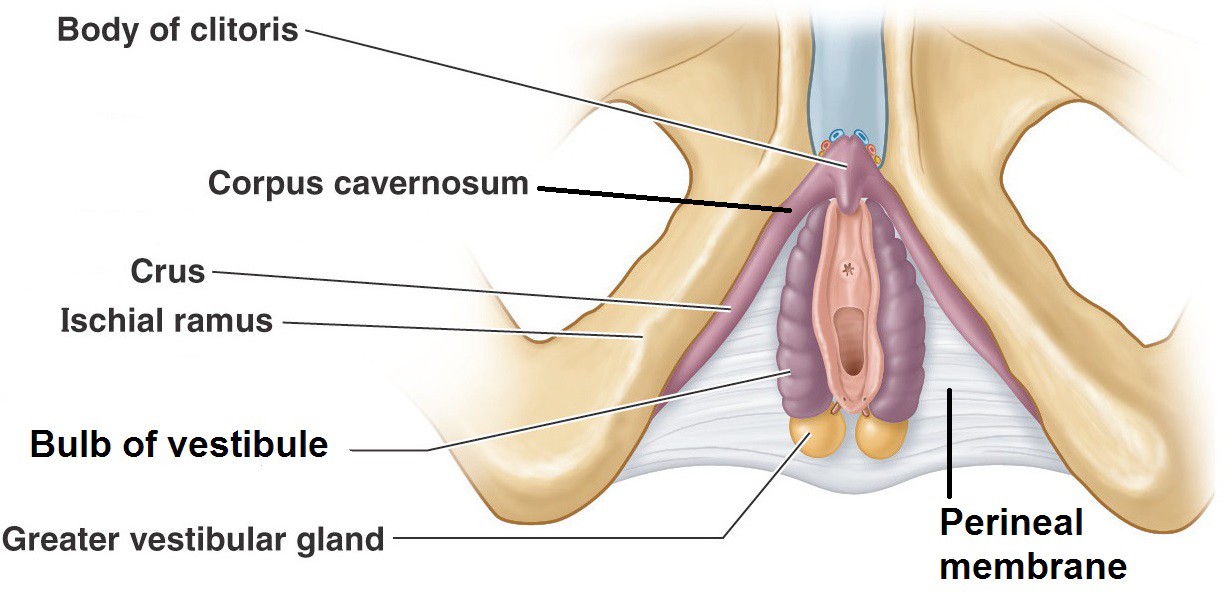
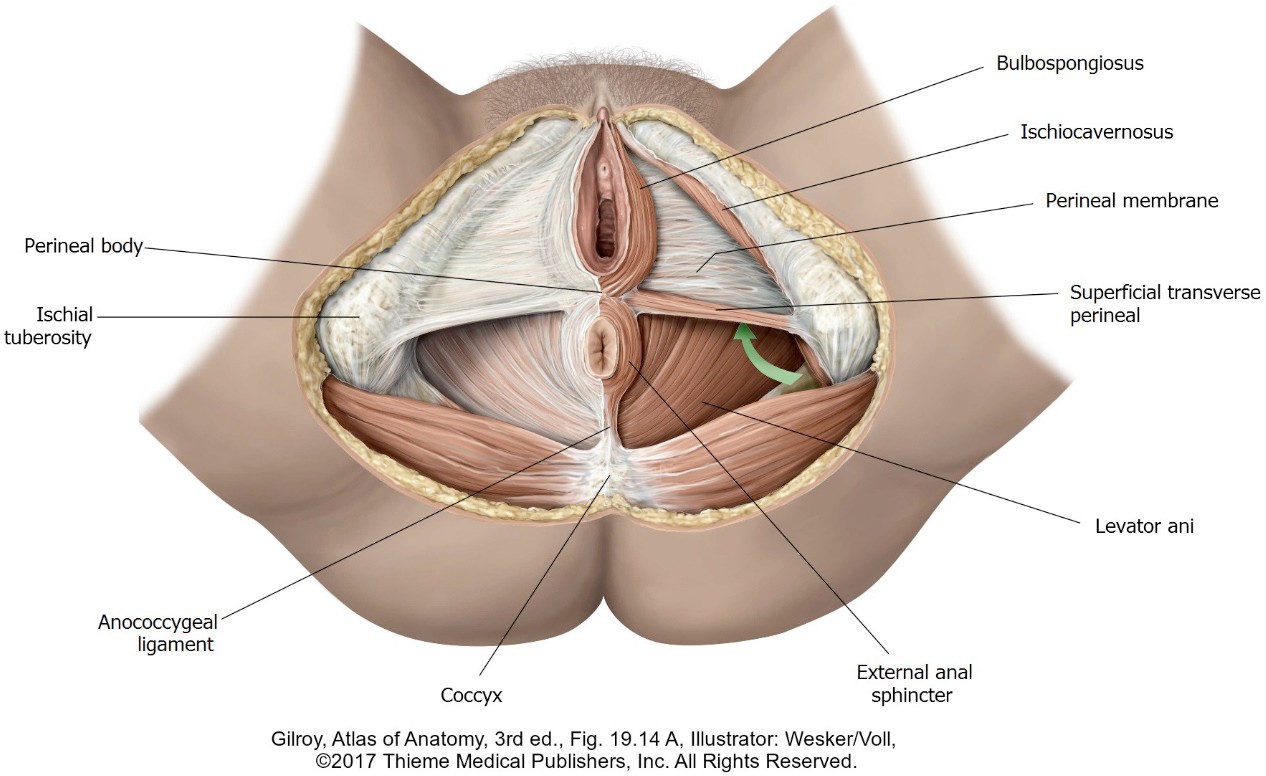
In addition to the clitoris, bulbs of the vestibule, and greater vestibular (Bartholin’s) glands, which have already been discussed, the superficial pouch in females contains skeletal muscles (paired = left and right):
-
- Ischiocavernosus muscles: Insert into the crura of the clitoris. These muscles are thought to support the erect clitoris and maintain erection by compressing veins to restrict outflow of blood.
- Bulbospongiosus muscles: Cover the bulbs of the vestibule. They function to constrict the orifice of the vagina (closing the vagina to protect it), support the clitoris, and compress Bartholin’s glands to empty them.
- Superficial transverse perineal muscles: Insert into the perineal body (described later) in the midline of the perineum and act to produce tension to support the perineum and pelvic viscera.
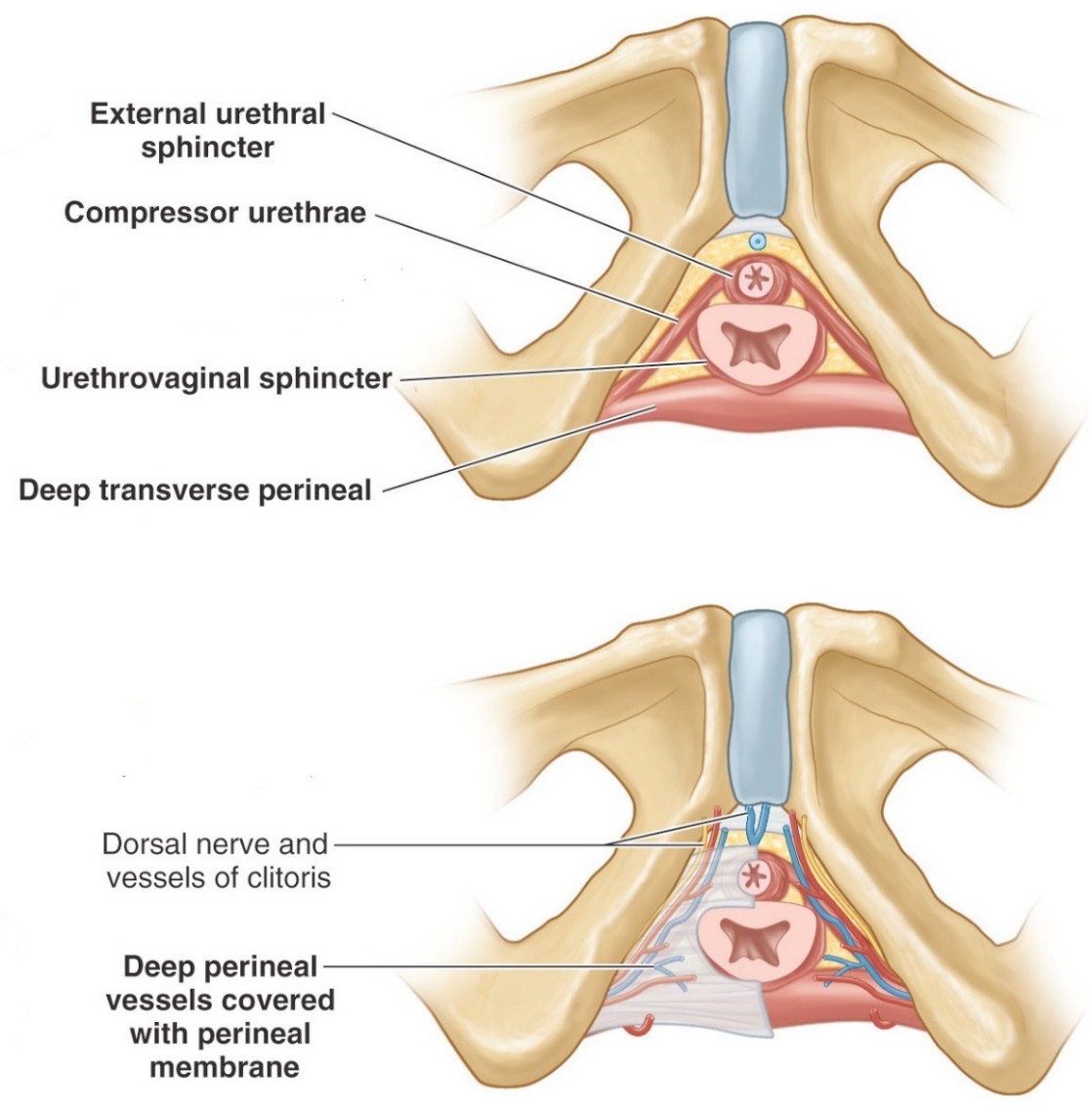
(See Figure 10.) This poorly defined compartment above the perineal membrane contains the urethra and vagina and two muscles, also innervated by the pudendal nerve:
-
- Deep transverse perineal muscles: Contains a mix of skeletal and smooth muscle. Functions similar to the superficial transverse perineal muscles in supporting the perineum and pelvic viscera.
- External urethral sphincter: Surrounds the urethra above the perineal membrane and compresses it to maintain urinary continence. Contraction can also interrupt the stream of urine during micturition. Children learn to control this voluntary sphincter through “toilet training”. Some of its muscle fibers encircle the vagina and function to constrict the vaginal lumen.
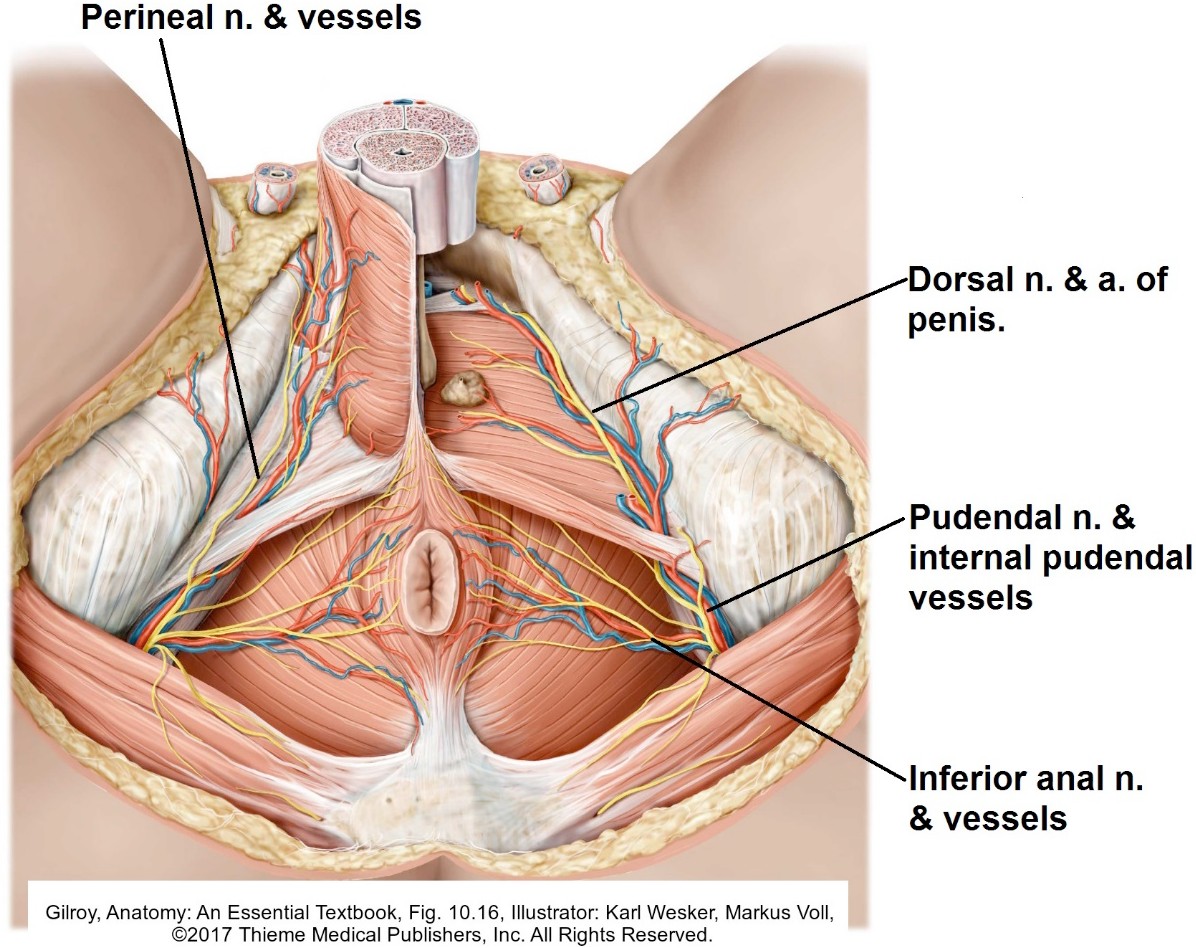
- The dorsal nerves and arteries of the clitoris, terminal branches of the pudendal nerves and internal pudendal arteries, course through the deep pouch on their way to the dorsal surface of the clitoris.
Blood supply
The blood supply is via deep and dorsal arteries of the penis. These are the terminal branches of the internal pudendal arteries. Dorsal veins of the penis drain the blood.
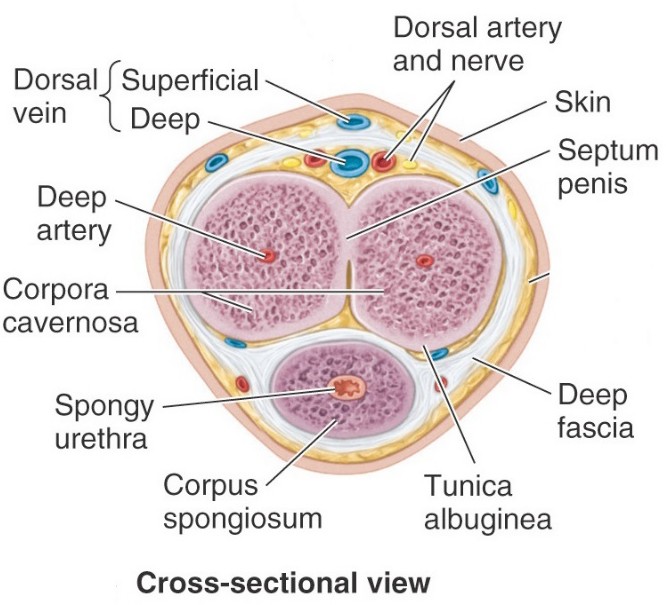
The erectile bodies of the penis and clitoris contain a meshwork of fibrous trabeculae derived from the tunica albuginea. Between the trabeculae are spaces resembling tiny collapsed veins. These cavernous spaces fill with blood during sexual arousal. The erectile bodies receive their blood supply from tiny corkscrew- shaped helicine arteries, branches of the deep and dorsal arteries of the penis/ clitoris. In their coiled configuration, there is little blood flow through the arteries.
Parasympathetic stimulation relaxes smooth muscle in helicine arteries. As they fill with blood they “straighten out” and blood flows into the cavernous spaces and distends the erectile bodies. Swelling of the penis and clitoris (technical term = tumescence) compresses the veins draining the erectile bodies, mainly the deep dorsal vein of the penis/clitoris. This helps maintain the erection.
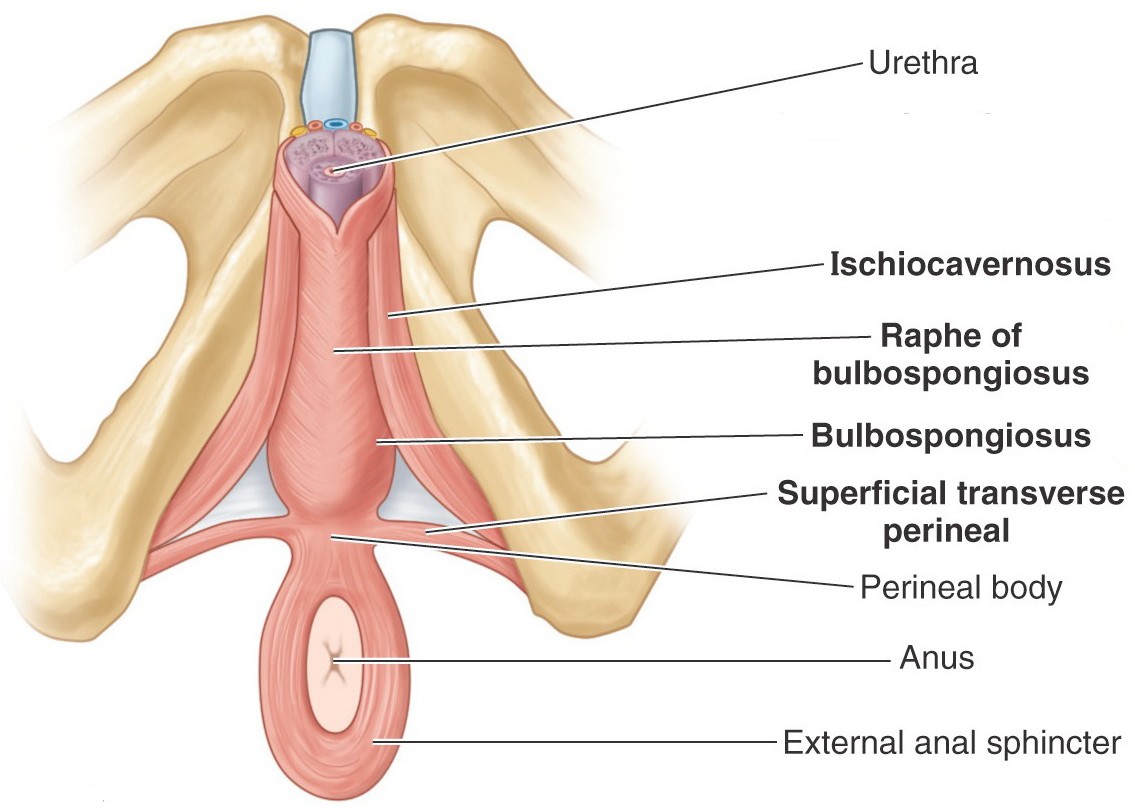
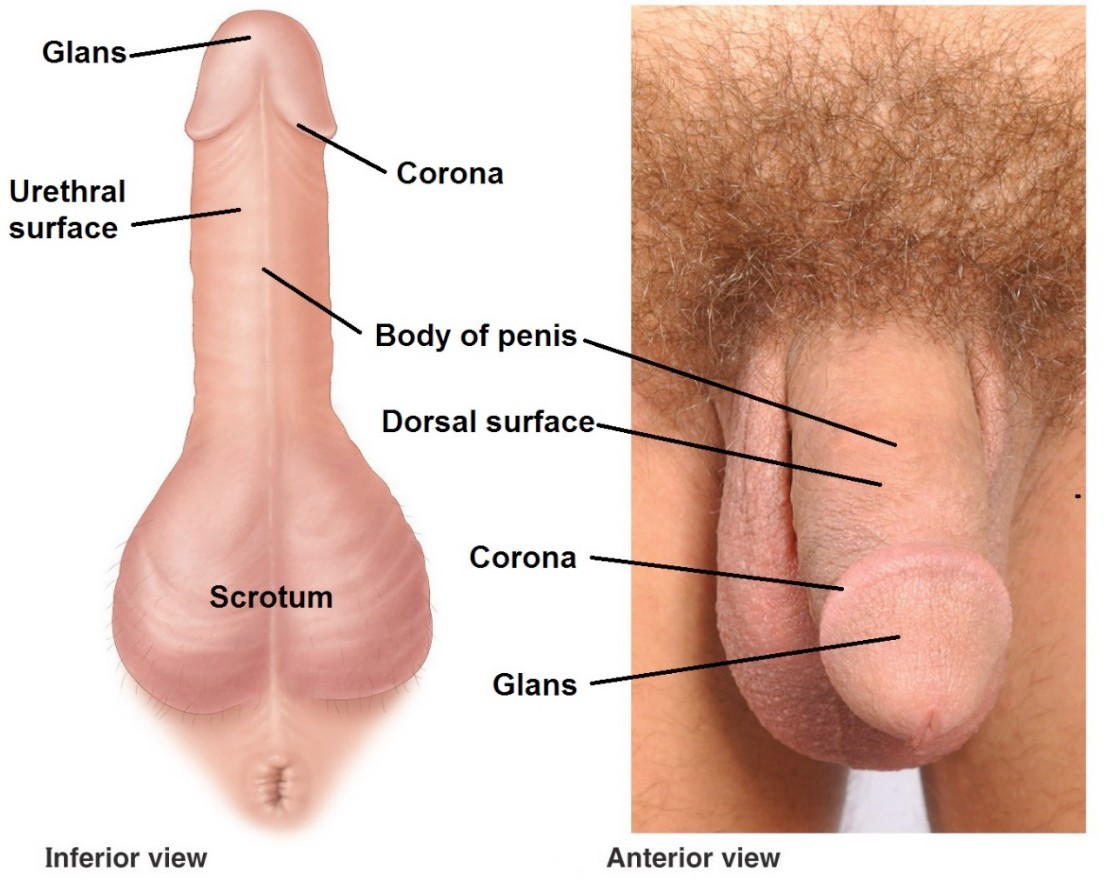
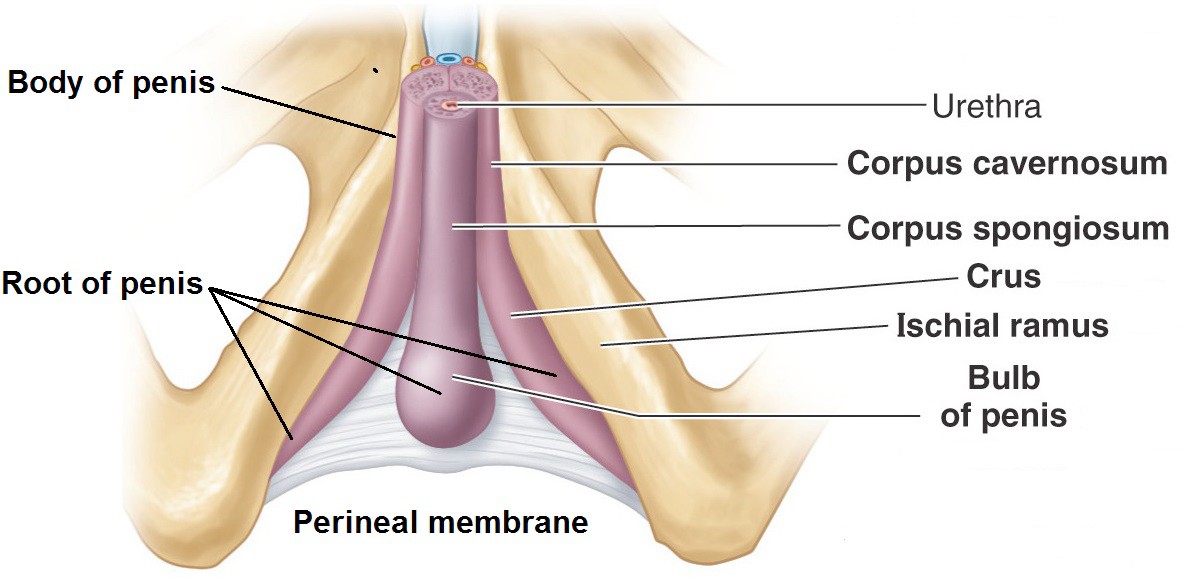
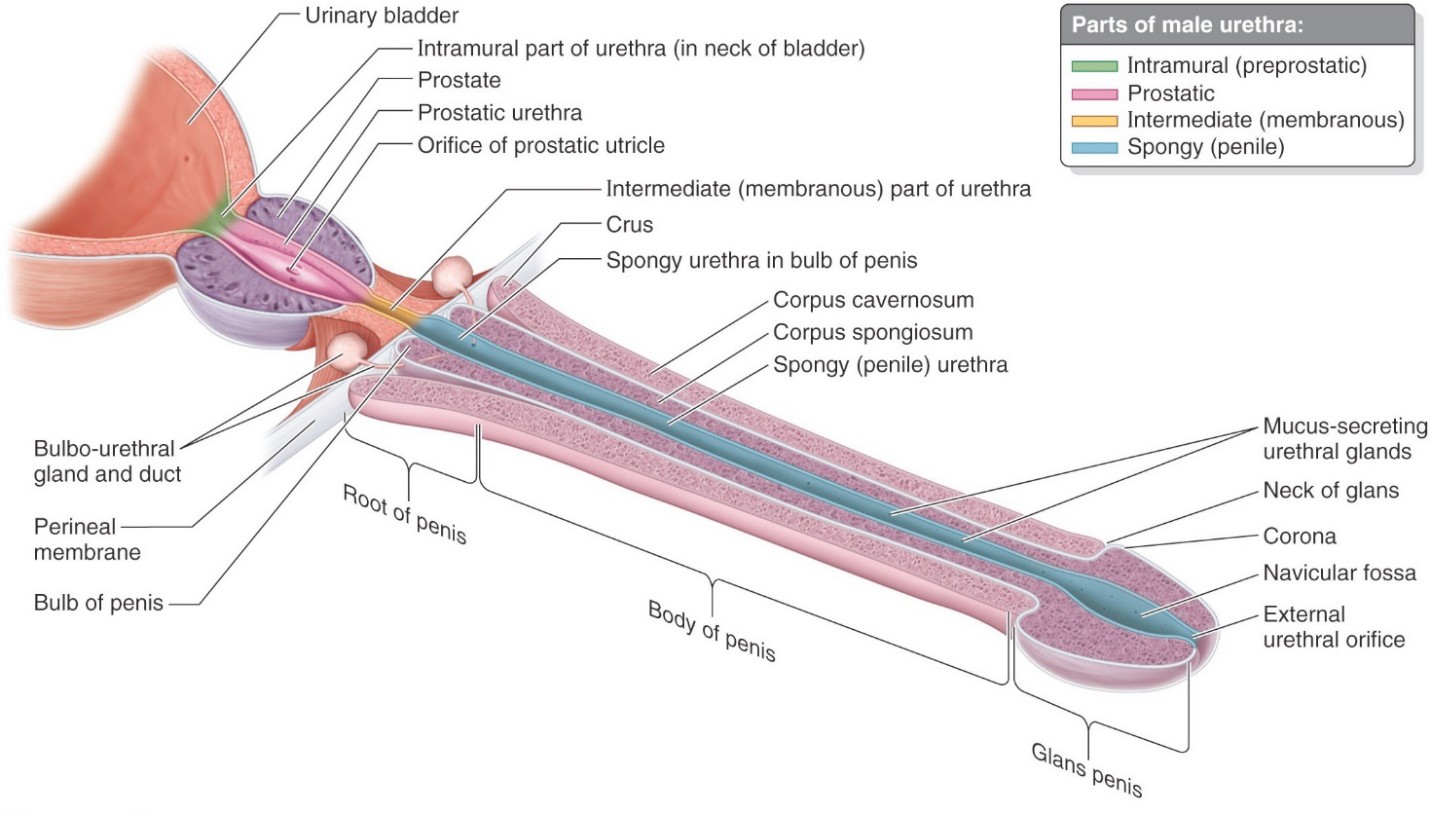
Contains the root of the penis (discussed earlier), proximal part of the spongy urethra (called the bulbar part by clinicians),and skeletal muscles. The pendulous part of the penis hangs down away from the perineum, so only its “root” is technically contained in the superficial pouch. The muscles in the superficial pouch have the same names as those in the female, but are generally more robust. See Figure 14.
-
- Ischiocavernosus muscles: Originate from the ischiopubic rami and insert on the crura of the penis. They support the erect penis and maintain the erection by compressing veins to restrict the outflow of blood.
- Bulbospongiosus muscles: The left and right muscles unite in the midline (in a tendinous raphé) over the bulb of the penis. They function in the male to support the penis and compress the bulb—this squeezing action ejects the last few drops of urine or semen from the urethra.
- Superficial transverse perineal muscles: Originate from the ischial tuberosities and insert into the perineal body in the midline of the perineum. They support the perineum and pelvic viscera.
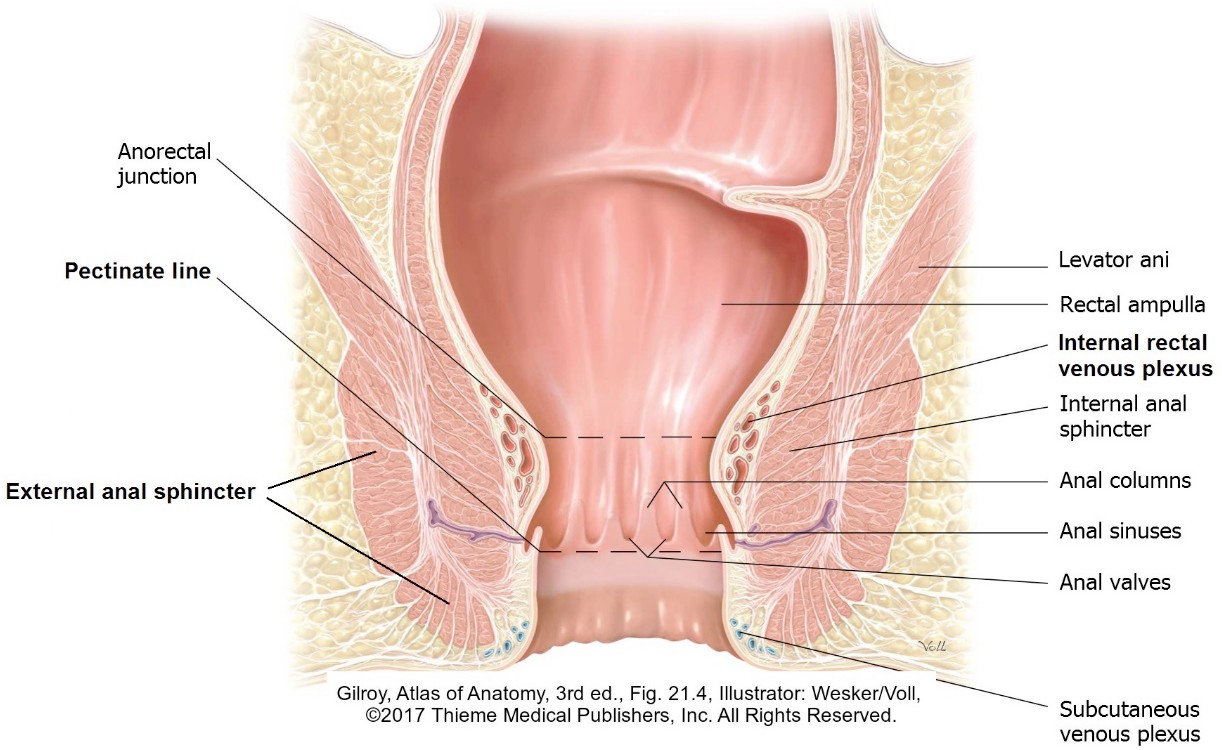
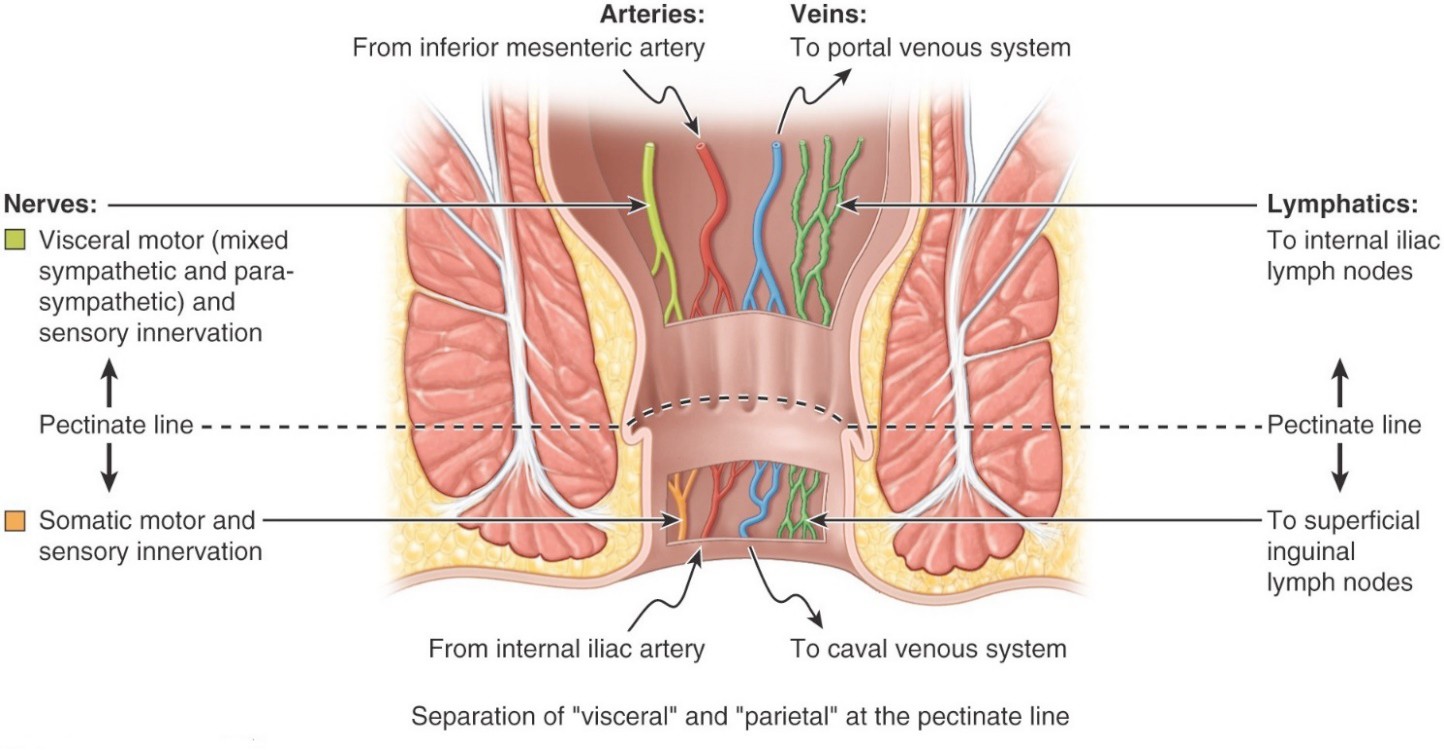
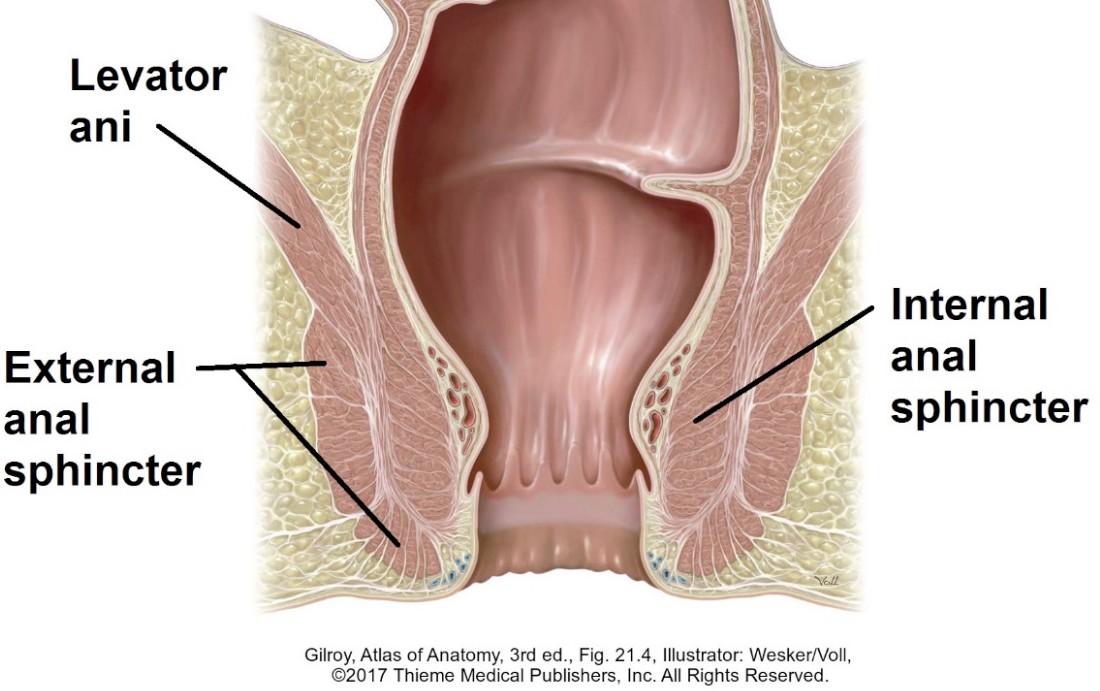
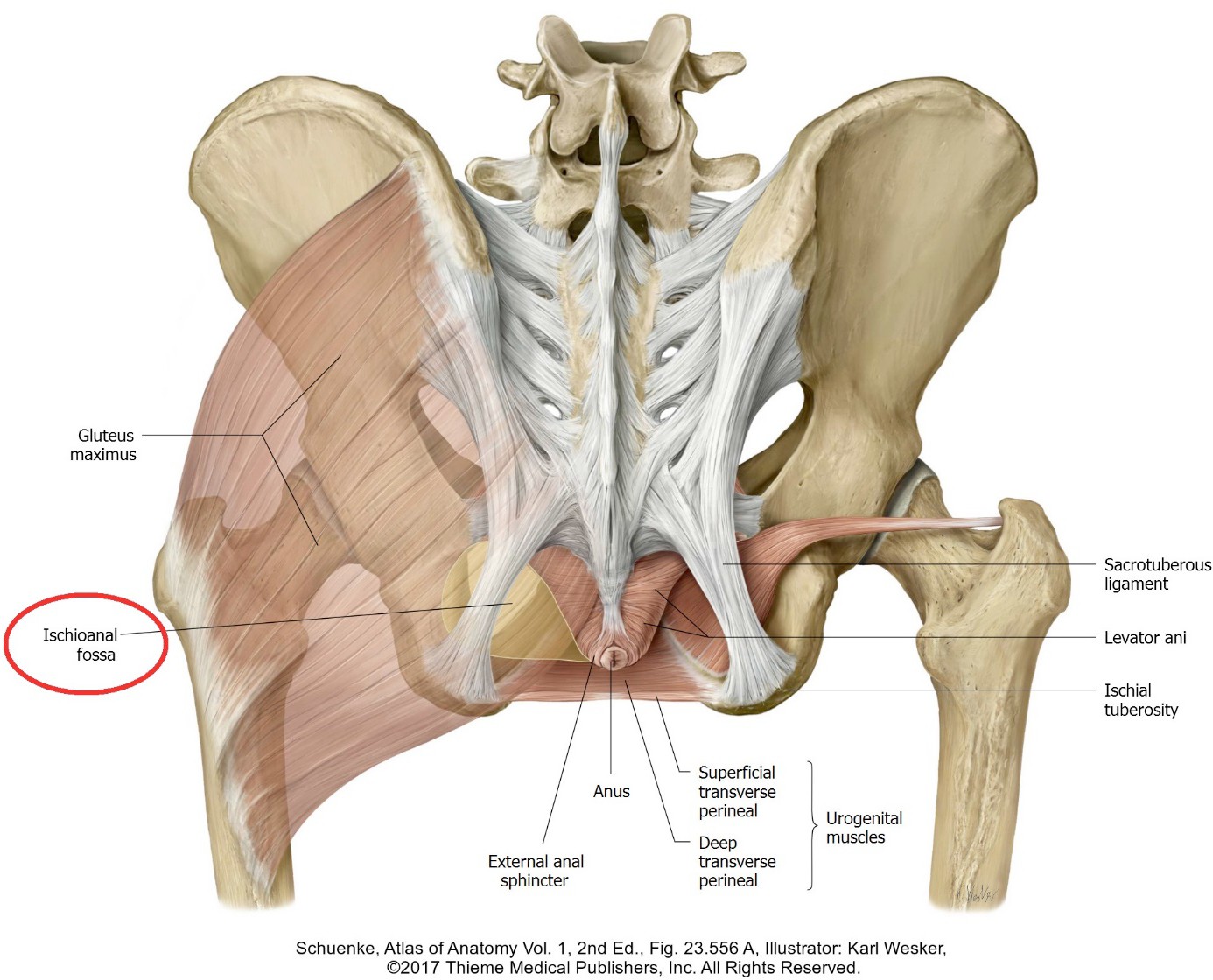
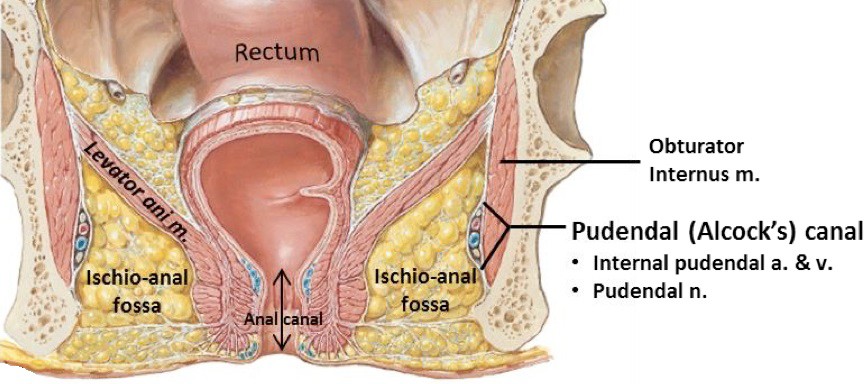
Contains the anal canal, external anal sphincter, and the left and right ischio-anal fossae. The anal canal opens at the center of the anal triangle at the anus. The anus is within the intergluteal cleft, also called the natal cleft. The roof of the anal triangle is the pelvic diaphragm. The external surface of the anal triangle is covered by skin. There are no pouches in the anal triangle (thank goodness!).

Lymph from the testes follows blood vessels upwards to the nodes in the posterior abdominal wall near the origin of the testicular artery = lumbar (para-aortic) nodes. Treatment of testicular cancer targets nodes in the posterior abdominal wall!