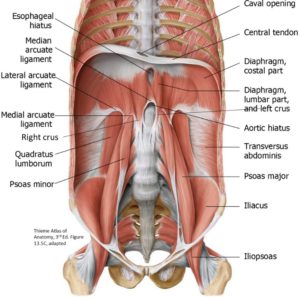
Origin: Lateral bodies, transverse processes of T12–L5;inserts: lessertrochanter of femur (with the iliacus muscle, now called iliopsoas) by a strong tendon
Action: Main thigh flexor, laterally flexes vertebral column
Psoas minor: Thin strip anterior to psoas major; absent in 40% of individuals
Iliacus muscle: Originates in iliac fossa, fuses with the psoas major inferiorly, inserts on lesser trochanter
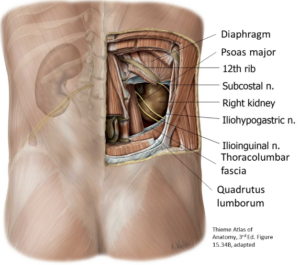
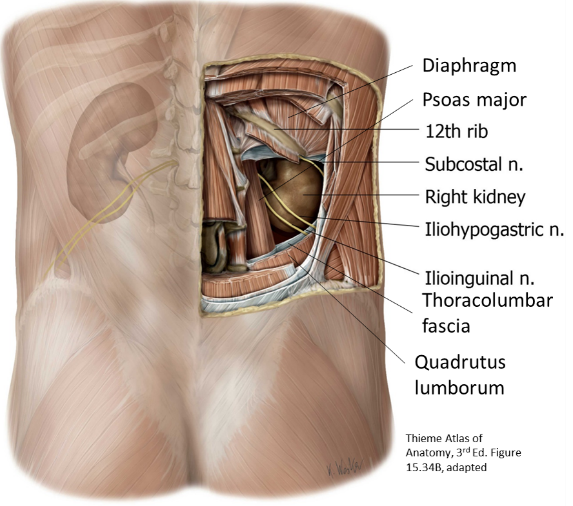
Thick muscular sheet in the PAW; iliac crest up to rib 12 and transverse processes of lumbar vertebrae
Enclosed between two layers of lumbar fascia, which join to form a thick sheet of lumbar fascia lateral to quadratus lumborum
Action: Laterally flexes the vertebral column, as when bending sideways. Stabilizes 12th rib during inspiration.
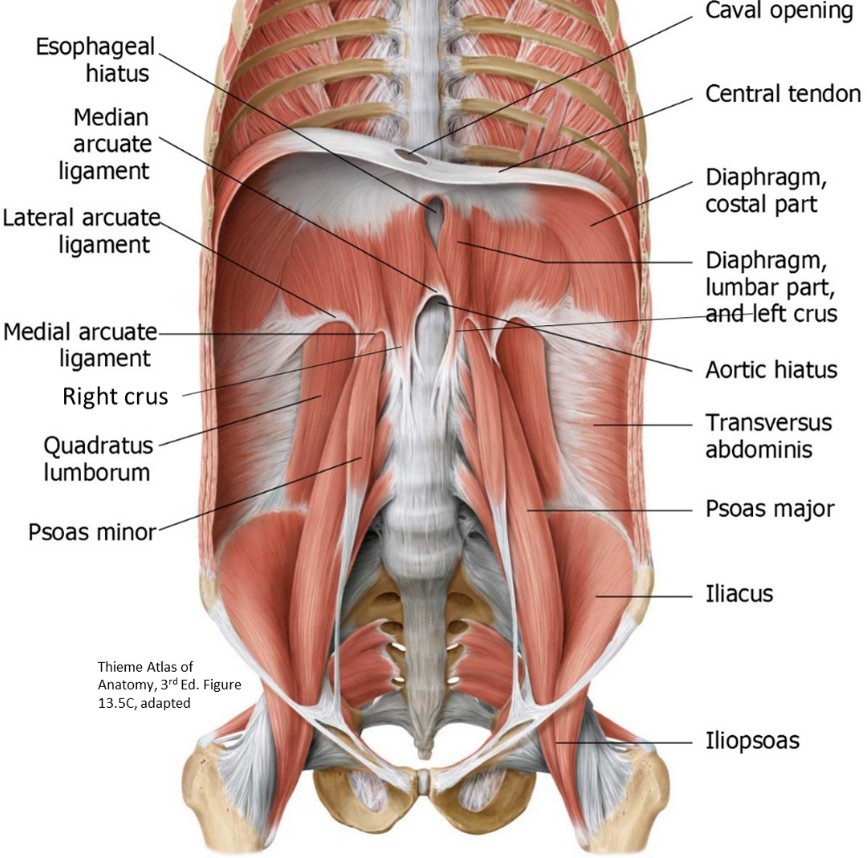
Development of the diaphragm
Figure 2. Development of the diaphragm. LANGMAN’S MEDICAL EMBRYOLOGY, 12TH ED., FIGURE 7.7.
The diaphragm is a composite structure that develops from four embryonic tissue sources:
septum transversum
Somatic mesoderm
dorsal mesentery
pleuroperitoneal membranes
The septum transversum forms the central tendon of the diaphragm. If you don’t remember what the septum transversum is, review folding of the embryo in Week 4 of human development.
Somatic mesoderm from the embryo’s body wall grows inward toward the central tendon, forming the muscular peripheral parts of the diaphragm, where it attaches to the ribs, costal cartilages, and sternum.
The embryonic dorsal mesentery of the esophagus acquires muscle forming cells and gives rise to the crura of the diaphragm.
Two sheets of mesenchyme grow in the center of the “domes” of the diaphragm, to the left and right of the central tendon. These pleuroperitoneal membranes partition the intra-embryonic coelom(remember the IEC?). Above the membranes is the cranial “bicycle handlebars” part of the IEC. Below the membranes are the left and right caudal limbs of the IEC = the coelomic ducts. Formation of the pleuroperitoneal membranes is a crucial step in separating the thoracic cavity from the abdominal cavity.
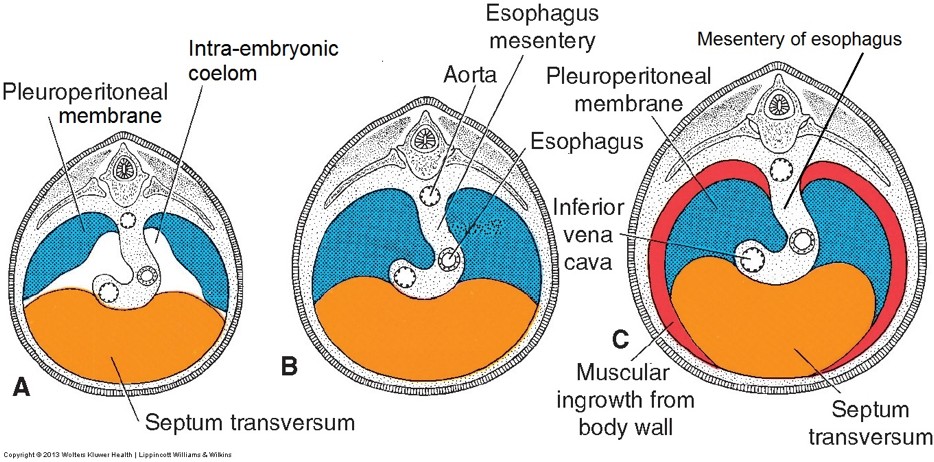
Clinical correlation
Faulty formation of the diaphragm that allows communication between thoracic and abdominal cavities is called congenital diaphragmatic hernia.
The culprit is usually malformation of a pleuroperitoneal membrane. These are much more likely to occur on the left side than on the right, because the left pleuroperitoneal membrane is larger and closes later than does the right. Theprevalence is 1 of every 2,500 live births (Children’s Hospital of Philadelphia). If the hernia is large enough, abdominal organs can bulge into the thoracic cavity, stunting the growth of the lungs (pulmonary hypoplasia). This can be a life-threatening condition.
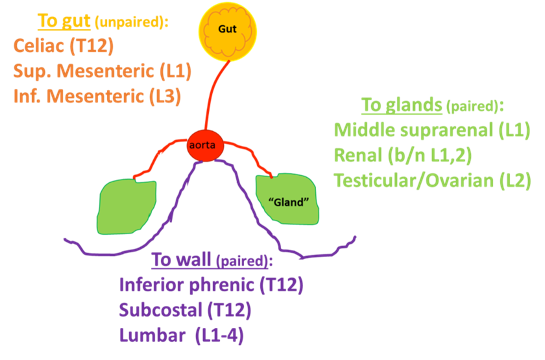
The abdominal aorta spans from T12 to L4, where it bifurcates into the right and left common iliac arteries. It has three types of arterial branches that supply “the gut, glands, and the wall.”
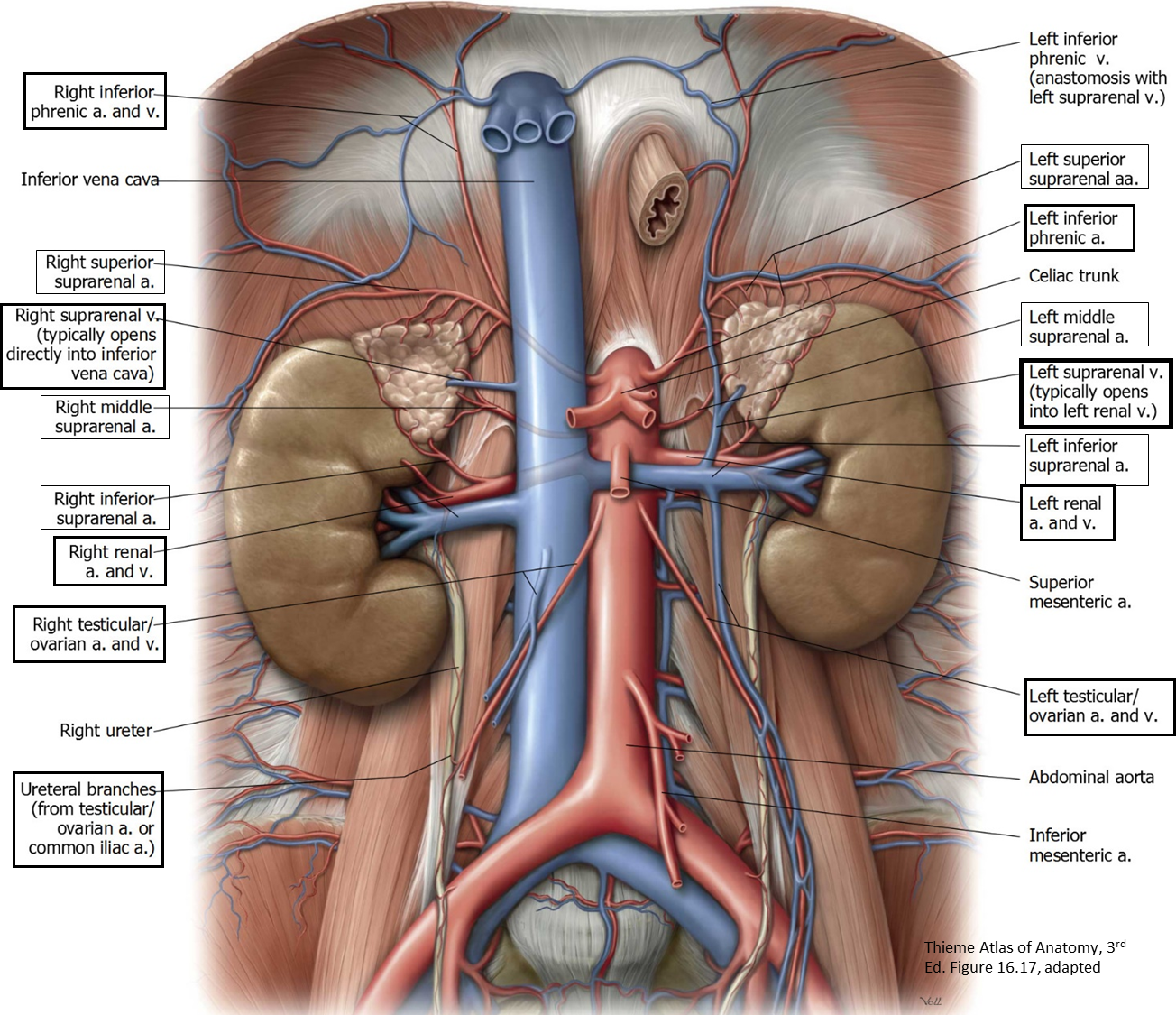
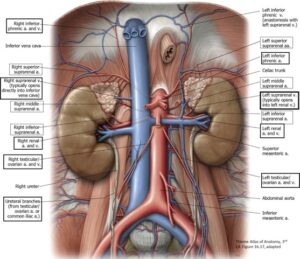
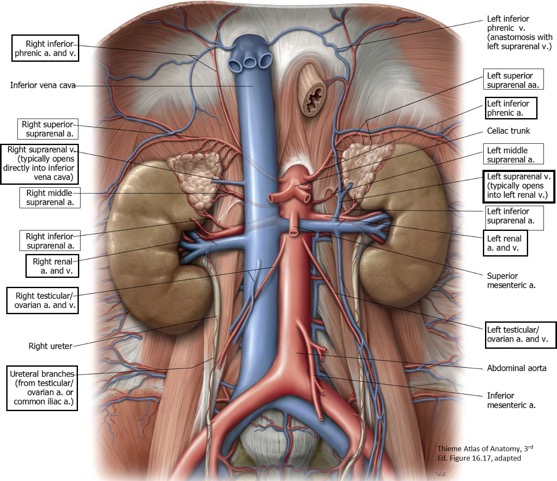
Veins of the posterior abdominal wall
Figure 5.
Common iliac veins join to form the IVC at L5
Inferior vena cava (IVC) and its tributaries; IVC ascends to the caval hiatus in the diaphragm
Lies to the right of the aorta on the vertebral bodies
Tributaries correspond to the paired visceral and parietal branches of the abdominal aorta. (The corresponding unpaired visceral branches from the gut are tributaries of the portal vein.)
exception
LEFT suprarenal and gonadal (testicular/ovarian) veins do notdrain directly into the IVC, but into the LEFT renal vein.
Clinical correlation
The relationship between the superior mesenteric artery (SMA) passing over the left renal vein can have rare consequences. "Nutcracker syndrome" is a vascular compression pathology where the left renal vein is compressed within a "vise" between the SMA and abdominal aorta. This uncommon disorder produces hematuria and left flank pain.
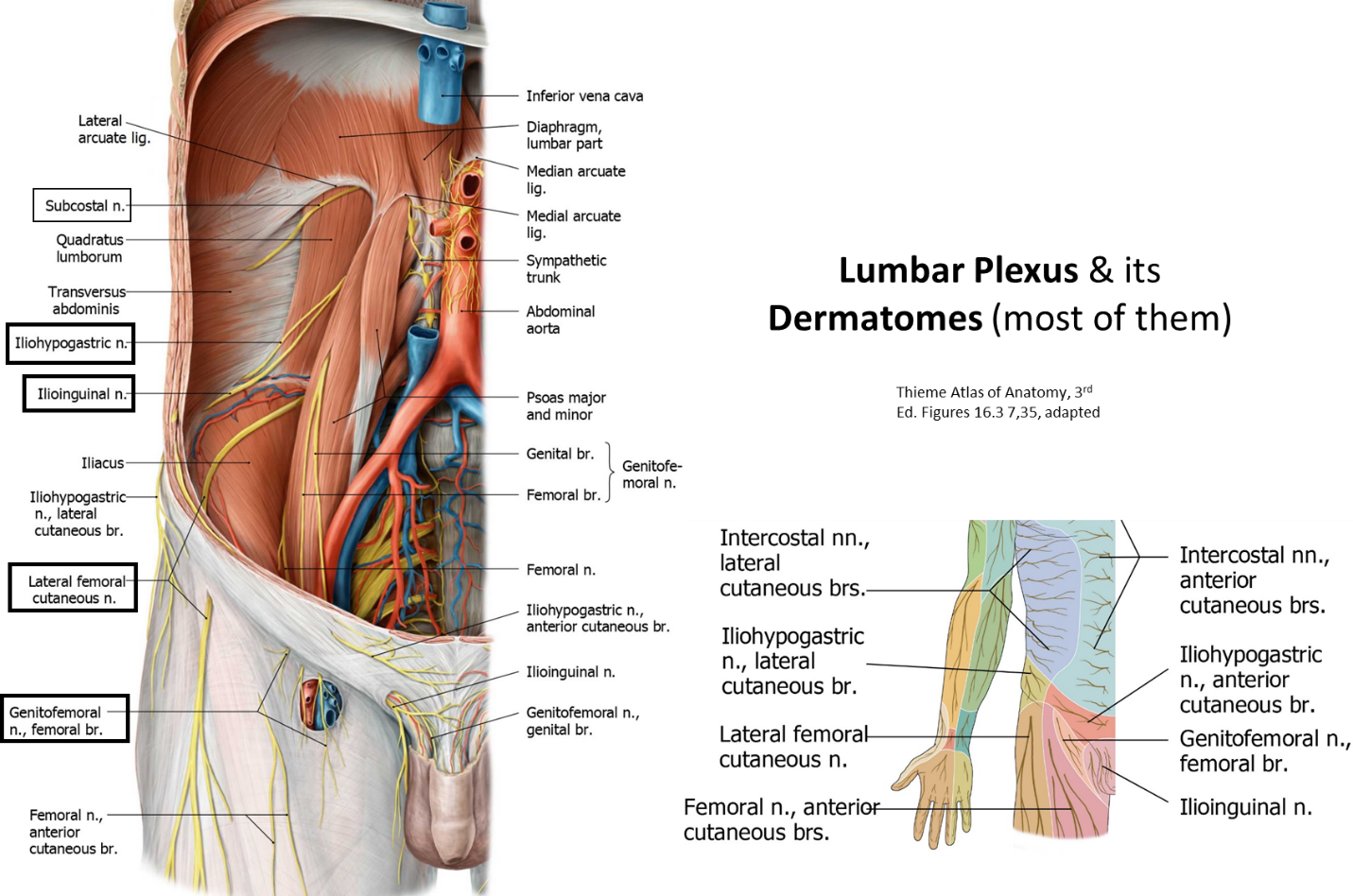
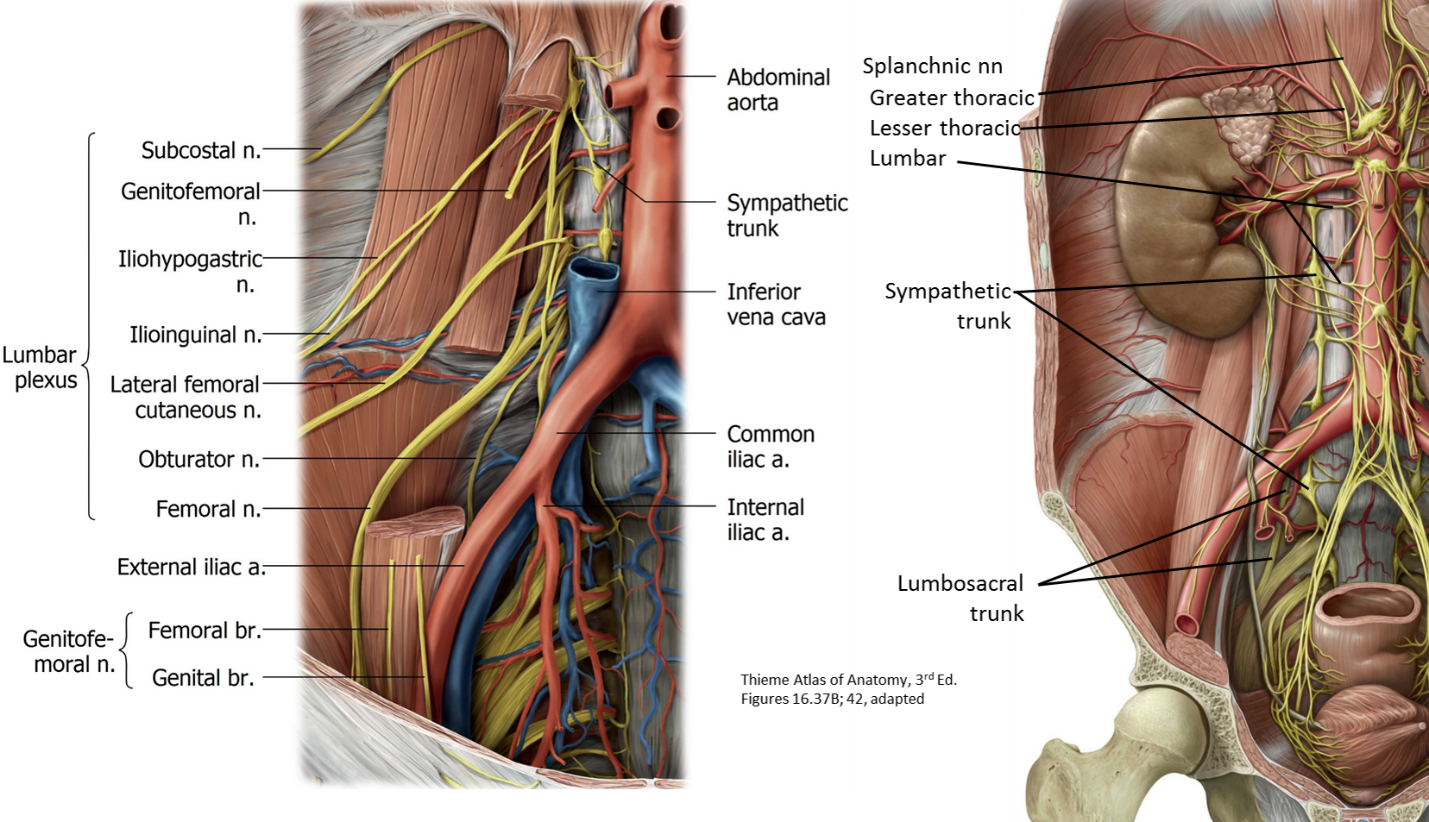
PAW nerves: The lumbar plexus
Located posterior to the posas major muscles
Formed by the ventral rami of the L1 to L4 spinal nerves—SOMATIC
Contributes the L4,5 segments to the sciatic nerve in the pelvis
Best place to find it: Medial to psoas major, on the ala of the sacrum
Aortic plexus
The aortic plexus is the major autonomic nerve plexus in the abdomen. Like the cardiac plexus in the thoracic cavity, the aortic plexus contains:
1
Sympathetic nerve fibers
2
Parasympathetic nerve fibers
3
Visceral afferent nerve fibers
The aortic plexus is located on the surface of the abdominal aorta, from aortic hiatus above to aortic bifurcation below, and extending further into the pelvic cavity along the surface of the sacrum.
The aortic plexus supplies organs of the GI tract, retroperitoneal organs, and pelvic organs with autonomic fibers.
Nerves issued from the aortic plexus follow branches of the abdominal aorta to reach target organs. In doing so, they form “sub-plexuses” = celiac, superior mesenteric, renal, and inferior mesenteric plexuses. The continuation of the aortic plexus below the aortic bifurcation is called the superior hypogastric plexus.
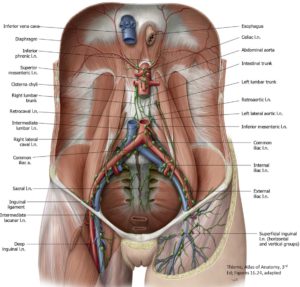
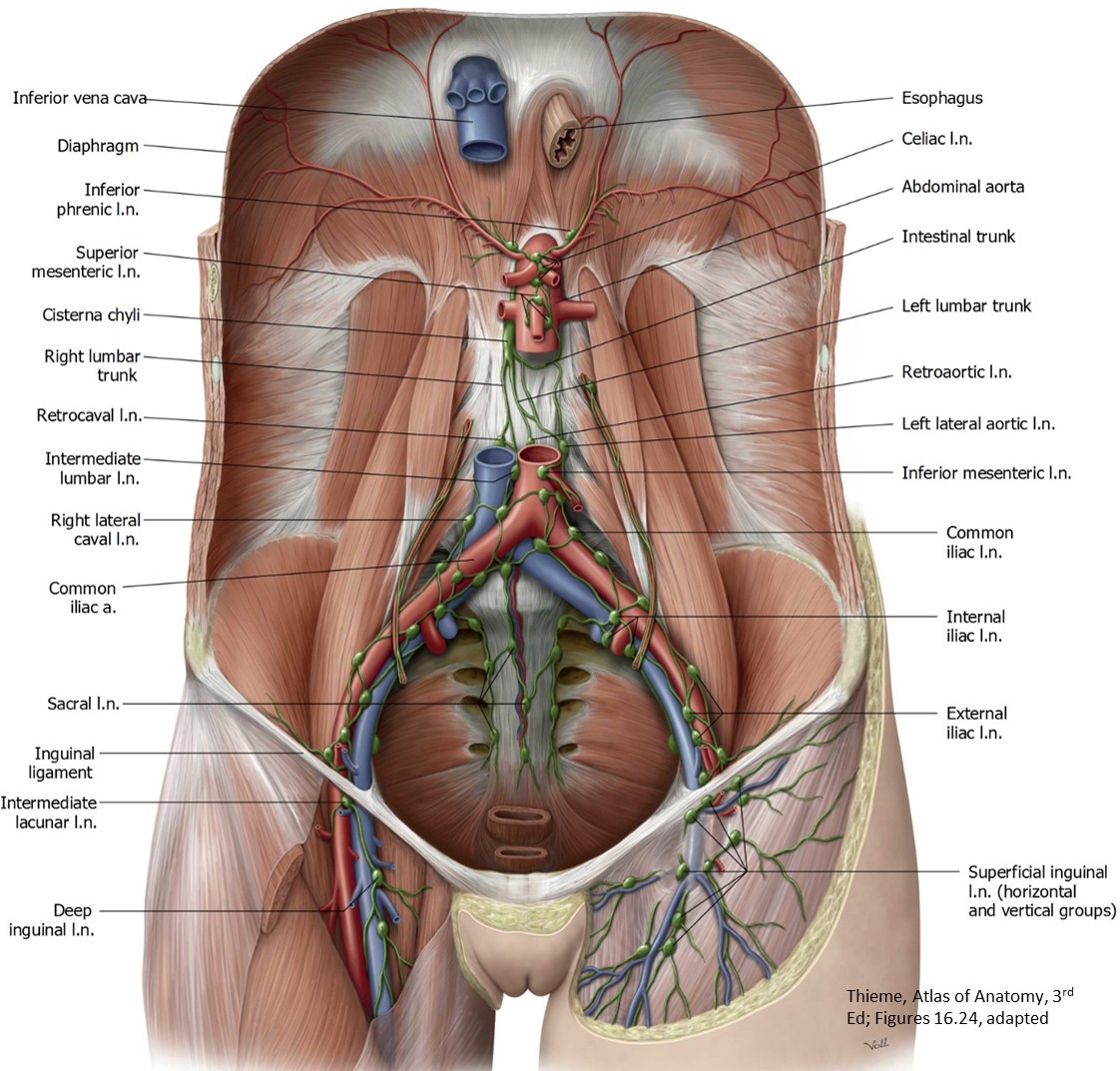
PAW lymph vessels
Figure 8.
Lie along the aorta, IVC, and iliac vessels
Lymph from the muscles and organs of the PAW drains to the lumbar lymph nodes, then to the right and left lumbar trunks, which empty into the cisterna chyli.
Cisterna chyli: Lies near T12, and is the beginning of the thoracic duct, and ascends along the abdominal-vertebral between the right crus of the diaphragm and the aorta, leaving through the aortic hiatus.
All the lymphatic drainage from the lower half of the body converges in the abdomen at the thoracic duct.
Kidneys
Receive ~20% of cardiac output, and is in a key position for regulating blood pressure, the composition of body fluids, and acid-base balance
Remove excess water, salts, and wastes from the blood, and return chemicals/ nutrients
Stimulate the manufacture of new red blood cells
Innervation: Renal plexus of nerves
Gross external anatomy
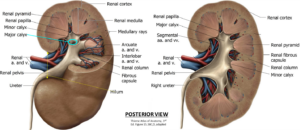
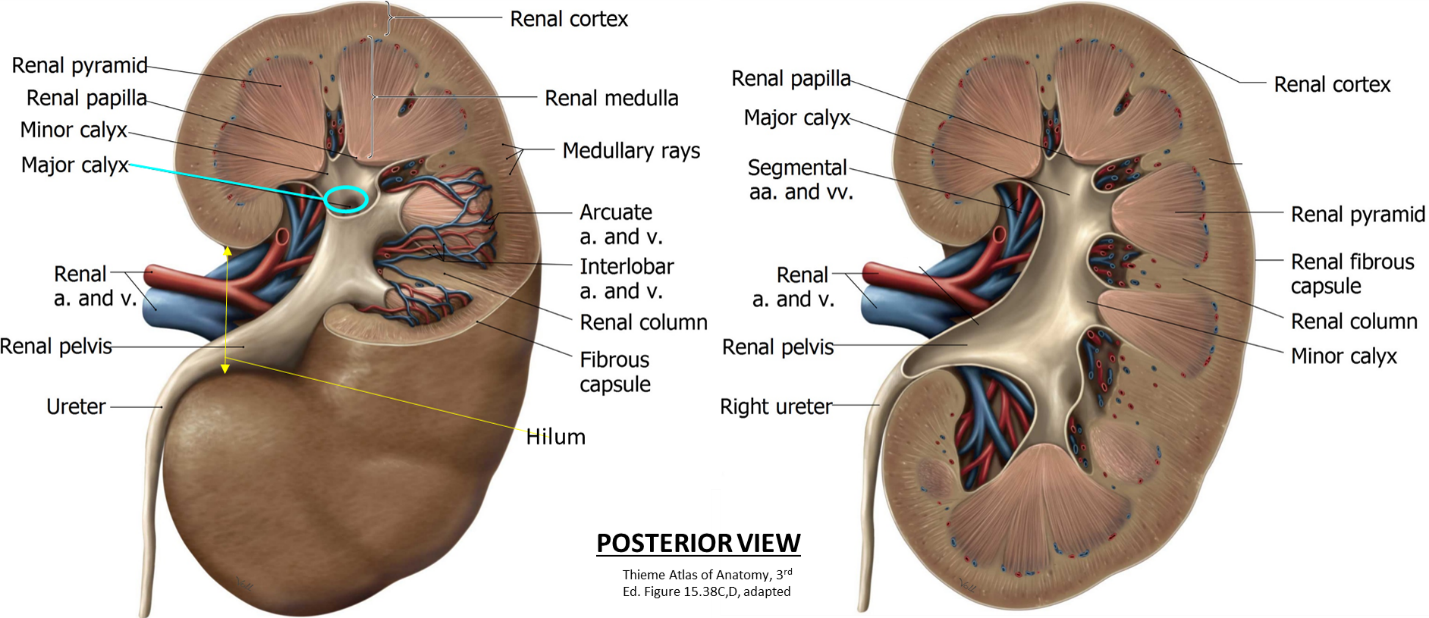
Gross internal anatomy
Figure 9.
Fist-sized and bean-shaped retroperitoneal organs
Lie T12–L3; right kidney is slightly lower than the left (due to the liver)
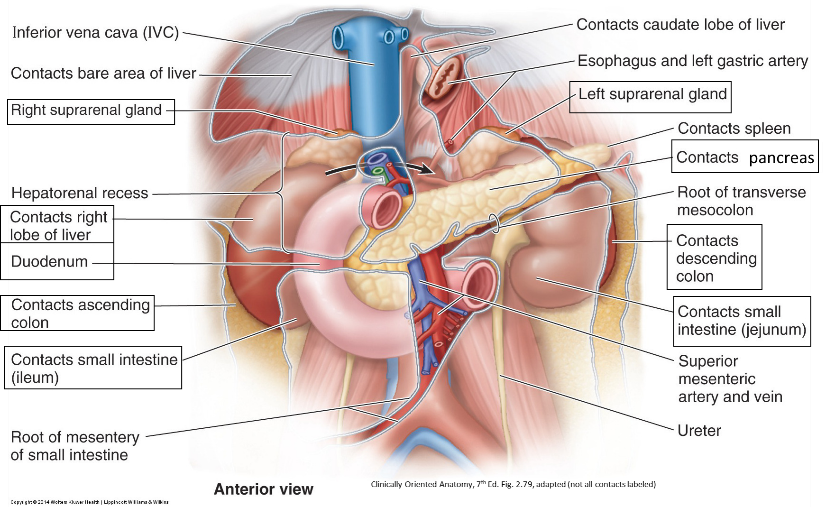
Relationships
Anterior:
Right: Right suprarenal gland, liver, descending duodenum, right colic flexure, small intestine
Left: Left suprarenal gland, stomach, pancreas, small intestine, spleen, left colic flexure, descending colon
Renal hilum and renal sinus (cavity within kidney, accessed via the hilum): Located at IV disc between L1 and L2
Renal vein is anterior to renal artery, which is anterior to renal pelvis (expanded upper part of ureter)
Figure 11.Renal cortex: Receives 90% of blood flow to kidney (receives ~20% of cardiac output!)
Lighter outer part just deep to capsule; where urine is made
Renal columns: Extensions of cortex between renal pyramids
Renal medulla (composed of the dark colored renal pyramids)
Where urine is concentrated, or diluted
Renal papilla: Apex of a renal pyramid; where the urine is excreted.
Minor calices (singular: calyx): Where papilla excretes urine; 2–3 per major calyx
Major calices: 2–3 total; where minor calices coalesce
Renal vessels
Renal artery 5 segmental (arise in the sinus, dividing kidney into distinct vascular segments) lobar interlobar (in renal columns) arcuate (arch over base of pyramid) interlobular (in cortex)
Clinical correlation
About 30 percent of individuals have an accessory renal artery (usually a "polar" artery from development). This is important for surgery!
Thickest posteriorly and an extension of the lumbar extraperitoneal fat; usually lots of it
Clinical correlation
All these layers must be traversed to reach the kidney during surgery. Also, the front and back layers of the renal fascia are not fused very tightly below the kidney, so a kidney can move inferiorly; this can kink the ureter and prevent urine from draining.
Ureter
Figure 12.
Muscular ducts that carry urine from the kidneys to the urinary bladder
In the same sagittal plane as the tips of the transverse processes of the lumbar vertebrae (which helps identify ureters on x-rays).
Blood supply: From renal artery, abdominal aorta, and vessels in the pelvis; is segmental so surgeons must be careful of manipulation or accidental injury causing ischemia.
Clinical correlation
Three narrowings along the course of the ureter, which are important as kidney stones frequently are lodged in these locations:
The ureteropelvic junction (as pelvis of ureter narrows to become ureter proper)
As it crosses over the pelvic brim and common iliac vessels
The right one is pyramid-shaped, the left one crescent-shaped.
Two glands in one: “Stress” hormones
Cortex: From mesoderm and secretes corticosteroids and androgens
Medulla: From neural crest cells and secretes catecholamines
Rich blood supply/many arteries (R/L superior, middle, inferior suprarenal aa); just one vein (the R/L suprarenal vein)
The suprarenal glands are also enclosed by the renal fascia
Have intimate topographic relationships to the kidneys = they rest upon the superior poles of the kidneys. However, developmentally, they have no relationship to kidney embryology. The two organs come from completely separate embryonic tissues!
Keep learning
The other parts of the urinary system (bladder and urethra) are in the Pelvic Viscera chapter.