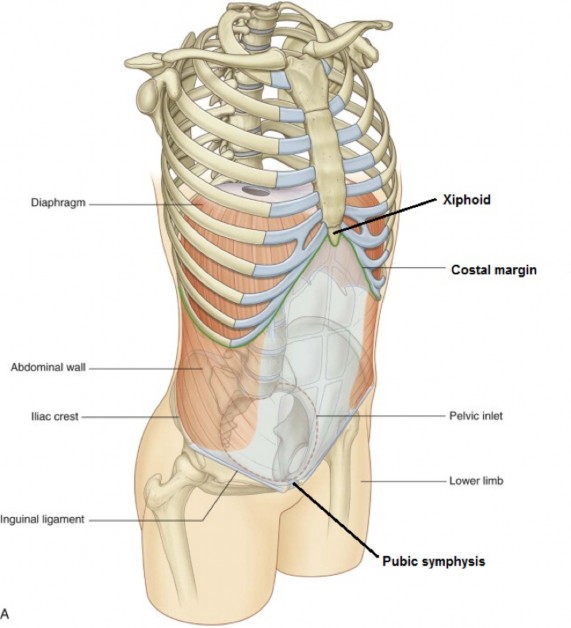
Figure 15.1 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 4.1.
The abdomen is the part of the trunk situated between the thorax above and pelvis below. On the surface of the body, the abdomen is bounded above by the xiphoid process and costal margins and below by the pubic bones, inguinal folds (skin folds between belly and thighs, raised up by the underlying inguinal ligaments) and the iliac crests.
The anterior/lateral and posterior abdominal walls are built quite differently.
Anterolateral abdominal wall
Unlike the thoracic wall, the anterolateral abdominal wall contains no bones. Its musculotendinous construction makes it both contractile and expandable, to raise intra-abdominal pressure and compress the abdominal contents, and to relax and allow for their distension.
Posterior abdominal wall
In comparison, the posterior abdominal wall contains the vertebral column, so it is bony, thick, and rigid, imparting stability and the capacity for weight bearing.
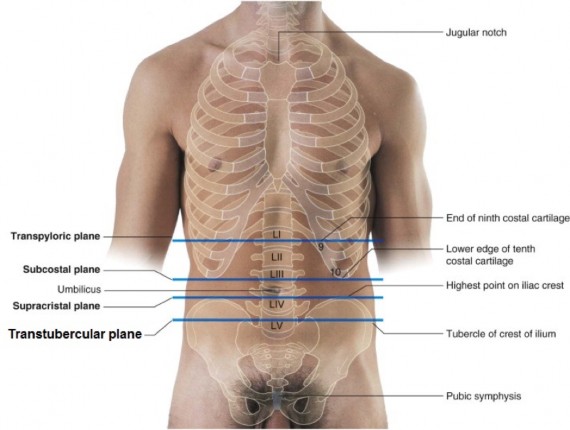
Abdominal planes
Anatomists use horizontal planes of reference on the surface of the body wall for locating abdominal organs.
At the level of L-1 vertebra, it is used to locate the surface projection of the pylorus of the stomach and the gallbladder. The most accurate way of locating it is to measure one hands-breadth below the xiphisternal junction (union of body and xiphoid of sternum).
At the level of L-4, it connects the highest points of the iliac crests. In lean individuals, it passes through the umbilicus and can be used to locate the surface projection of the bifurcation of the abdominal aorta.
Posteriorly, on the back, the supracristal plane can be used to mark a safe place for doing a lumbar puncture to withdraw cerebrospinal fluid from the subarachnoid space, since at this level a needle inserted will miss the spinal cord (do you remember where the spinal cord ends inferiorly?).
At the level of L-5, it connects the tubercles of the two iliac crests.
Figure 15.2 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 4.165.
Abdominal quadrants and regions
Clinicians use defined regions of the abdominal wall when locating organs and when describing pathologies or a patient’s pain.
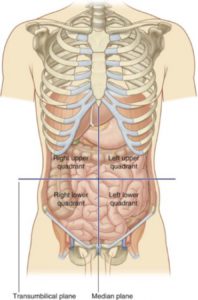
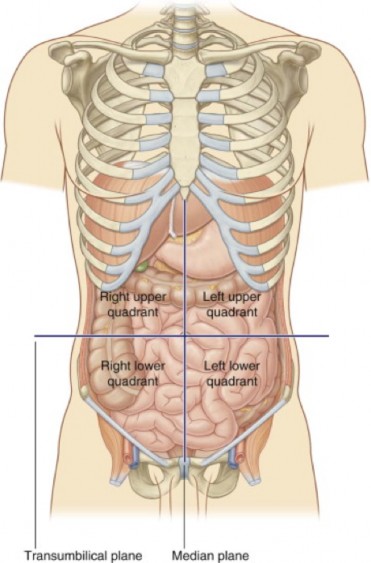
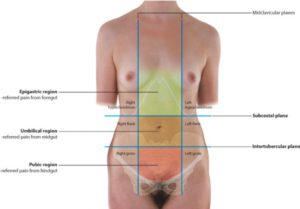
Figure 15.3 GRAY’ S ANATOMY FOR STUDENTS, 3RD ED., FIG. 4.22.
The four quadrants are the easiest to describe and the most commonly used. They are defined by the intersection of the vertical median plane and a horizontal plane passing through the umbilicus (often this is the supracristal plane).
The quadrants defined are: Right upper quadrant (RUQ), Left upper quadrant (LUQ), Right lower quadrant (RLQ), and Left lower quadrant (LLQ).
Figure 15.4 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 4.169.
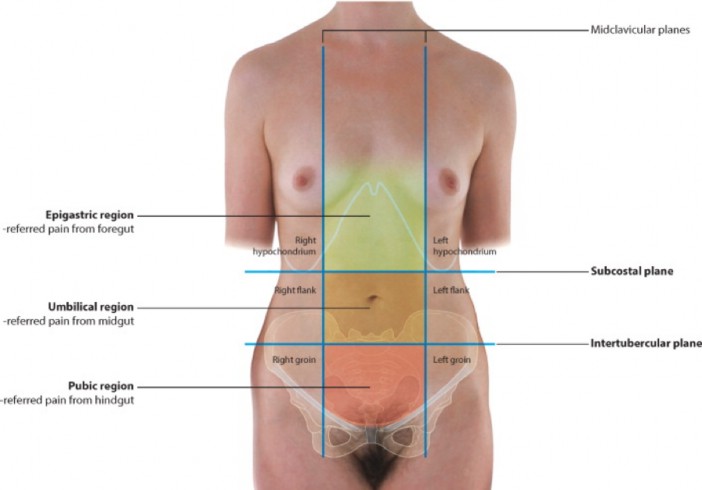
Another method divides the abdominal wall into nine regions. The vertical planes used are the midclavicular lines. The horizontal planes are the subcostal and transtubercular planes. The regions thus defined produce a “checkerboard” on the abdominal wall and are shown in Figure 15.4.
The three most important of these regions form the center column of the checkerboard: the epigastric, umbilical, and pubic regions. The pubic region is also called the “supra-pubic” or “hypogastric” region. These regions should be remembered, as they are important for describing referred pain from abdominal organs.
Clinical correlation
In a clinical setting, the most common way to describe the abdominal region is the “quadrant” system. Abbreviated: RUQ, LUQ, RLQ, LLQ
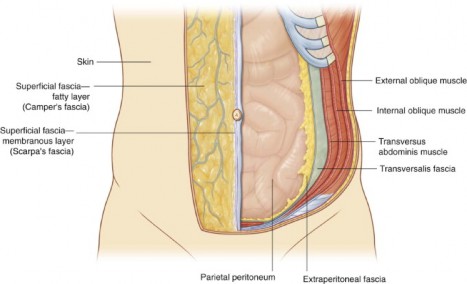
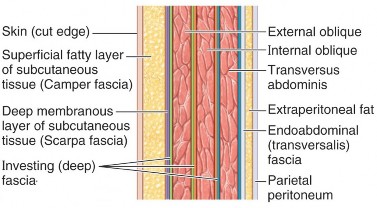
1. Outer: fatty layer of superficial fascia (“Camper’s” fascia). This layer is a favorite storehouse in the body for fat—it can be several inches thick.
2. Inner: membranous layer of superficial fascia (“Scarpa’s” fascia). When the fatty layer is well developed, the membranous layer can be demonstrated as a white sheet of collagenous tissue. It can be thick enough to be seen on CT scans and to put sutures in.
Surrounds all muscles of the anterolateral abdominal wall. Bound tightly to the fleshy muscles, it is difficult to remove.
A cleavage plane exists between the superficial fascia and deep fascia. This can be demonstrated by separating the layers with blunt dissection in the gross lab. This plane allows the skin and superficial fascia to glide on the underlying muscles and be pinched up and moved easily.
This is internal fascia—as defined in the Introduction to Anatomy. Transversalis fascia is the anterior part of a continuous fascial sheath (the endo-abdominal fascia) that lines and defines the abdominopelvic cavity. Subparts of the endo-abdominal fascia are given separate names according to nearby structures—in this case, the transversalis fascia lines the internal surface of the transversus abdominis muscle.
The three layers of body wall muscles in the abdomen have a unique construction.
Laterally
Laterally, where they attach to bony structures, they are fleshy.
Medially
Medially, where they converge on the midline of the abdominal wall, they are aponeurotic. An aponeurosis is a flat muscle tendon.
This construction allows the muscles of the anterolateral abdominal wall to distribute the forces they generate over a wide area, so that the contracted muscles can compress the abdominopelvic cavity and its contents and withstand pressures generated from within.
The aponeuroses of all three muscle layers fuse in a midline vertical tendon, that can be seen on the surface of the abdomen in lean individuals = the linea alba (“white line”).
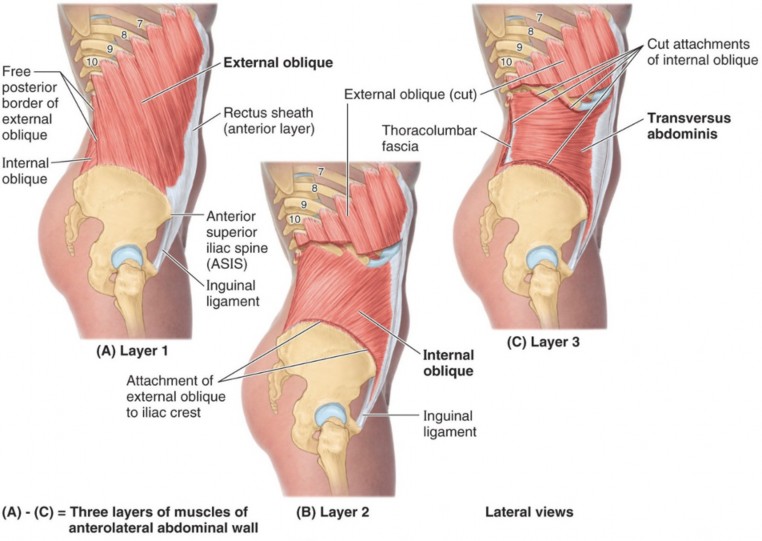
Figure 15.7 Three flat muscles of anterolateral abdominal wall. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 2.5.
Origin: Muscular fibers attach to the external surfaces of ribs 5–12, interdigitating with the serratus anterior. The muscle becomes aponeurotic about halfway across the abdominal wall.
Insertion: The posterior-most part of the muscle is fleshy. This part inserts on the anterior half of the iliac crest. The anterior-most part of the muscle is aponeurotic and inserts into the linea alba and on the pubic tubercle (pubic bone).
Fibers run inferior and medial (like the external intercostal muscles): Modeled by putting “hands in your front pockets.”
The external oblique has two free (un-attached) margins.
The posterior margin is fleshy and runs vertically between the ribs and iliac crest.
The inferior free margin is aponeurotic and stretches between the anterior superior iliac spine (ASIS) and the pubic tubercle. This thickened, J-shaped (in cross-section) margin of the aponeurosis is called the inguinal ligament. In lean individuals, it produces a ridge in the overlying skin = the inguinal fold.
Origin: From the thoracolumbar fascia in the back (this attaches medially to the vertebral column), anterior 2/3 of iliac crest, and lateral half of inguinal ligament.
Insertion: inferior borders of ribs 10-12, linea alba, and pubic bone (fusing with the aponeurosis of the transversus abdominis). The rib attachments are fleshy; the others are aponeurotic.
Fibers spread out like a “fan.” Most fibers run upward and medially (like the fibers in the internal intercostal muscles) at right angles to the external oblique, but the fibers that originate most anteriorly have a horizontal orientation.
Figure 15.8 CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 2.7.
Long, strap-like, paired, vertical muscles. Separated in the midline by the linea alba.
Origin: Pubic symphysis and pubic bones.
Insertion: Xiphoid process and 5th–7th costal cartilages.
The muscle fibers do not traverse the entire muscle length. Instead, the rectus abdominis is separated into segments (3 or 4), divided by horizontal bands called tendinous intersections. When seen on the body surface, these produce the famous “six-pack”!
The aponeuroses of the external oblique, internal oblique, and transversus abdominis surround and encase the rectus abdominis. This aponeurotic envelope is the rectus sheath. It functions to prevent the rectus abdominis from “bow- stringing” when the trunk is flexed (as in “sit ups”).
The surface landmark (in lean folks) along the lateral edge of the rectus abdominis is the linea semilunaris. There are two of these.
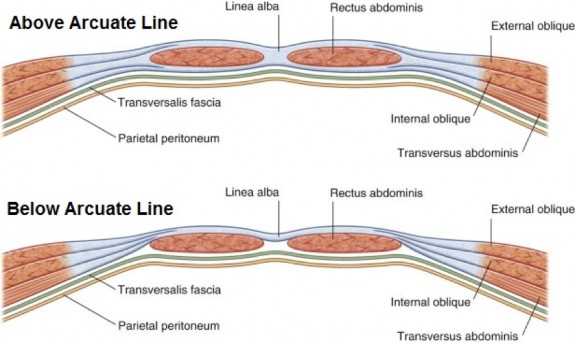
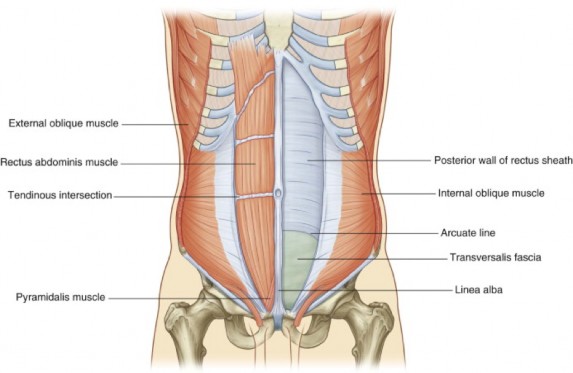
Strong, fibrous sheath of the rectus abdominis formed by the aponeuroses of the flat abdominal muscles (EO, IO, and TA).
Divides into an anterior layer and a posterior layer.
Throughout most of the length of the rectus abdominis, the aponeurotic layers of the rectus sheath are symmetrical.
The anterior layer is formed by the aponeurosis of the external oblique and half of the aponeurosis of the internal oblique (1.5 layers). The internal oblique aponeurosis splits—half passes anterior to the rectus abdominis and half passes posterior.
The posterior layer of the rectus sheath also contains 1.5 layers = half of the internal oblique aponeurosis and the aponeurosis of the transversus abdominis.
About midway between the umbilicus and pubic symphysis, the symmetry of the rectus sheath changes. Here, all three layers of aponeuroses suddenly pass anterior to the rectus abdominis muscle. This abrupt change produces a sharp, curved, aponeurotic line behind the rectus abdominis which demarcates the lower limit of the posterior layer of the rectus sheath = this is called the arcuate line.
Superior to the arcuate line, the internal oblique aponeurosis splits to envelope the rectus abdominis muscle, joining the external oblique aponeurosis in the anterior rectus sheath and transversus abdominis aponeurosis in the posterior rectus sheath.
Inferior to the arcuate line, all three muscle aponeuroses are anterior to the rectus abdominis. There is no posterior layer of rectus sheath here. Only the thin transversalis fascia covers the rectus abdominis muscle posteriorly.
Figure 15.9 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 4.33.Figure 15.10 Rectus sheath and arcuate line. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 4.32.
Six-pack review
Tendinous intersections are horizontal—they separate the rectus abdominis into segments.
Linea alba is vertical, from xiphoid to the pubic symphysis.
Formed by fusion of all three flat muscle aponeuroses in the midline.
Common site of surgical entry to the abdomen (median incision).
Linea semilunaris is a vertical curved tendinous line at the lateral border of the rectus abdominis (another fusion of all three aponeuroses).
Functions and actions of the anterolateral abdominal wall musculature
Support abdominal organs
This is accomplished by the three flat muscles (EO, IO, and TA). The rectus abdominis has little visceral support function.
All muscles of the anterolateral wall contribute to this function, an action that is important for many reasons:
Coughing and sneezing (rapid and forceful expulsion of air).
Forced expiration during respiration. These muscles are not active during quiet respiration.
Vomiting.
Valsalva maneuver (“bearing down”), used when emptying the bowels or bladder or for delivering a child through the vagina.
Movements of the trunk
(but only when working against gravity or resistance.) The rectus abdominis and oblique muscles can flex the trunk (bring the rib cage toward the pelvis). The oblique muscles can also twist the trunk to one side.
Clinical correlation
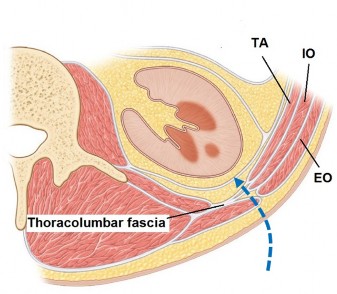
Surgical access to the retroperitoneum (area behind the peritoneal sac, adjacent to the posterior abdominal wall) can be gained through the common attachment of the internal oblique and transversus abdominus muscles to the thoracolumbar fascia in the flank region. See Figure 15.11. Although open surgeries have been replaced in most cases by laparoscopic transabdominal approaches, sometimes retroperitoneal exposures are preferred for nephrectomies or abdominal aortic aneurysm repairs.
Innervation and blood supply of anterolateral abdominal wall
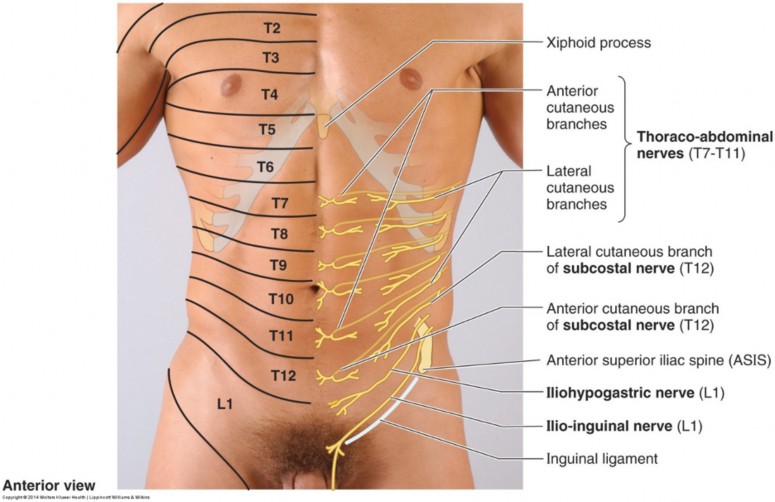
The muscles of the anterolateral abdominal wall are innervated segmentally by the ventral rami of spinal nerves T-6 to T-12. T-7 to T-11 nerves are known as thoraco-abdominal nerves, since they have left the intercostal spaces and can no longer be called intercostal nerves. T-12 is the subcostal nerve. Sometimes the ilioinguinal nerve (L-1) also contributes to the innervation.
The sensory innervation of the skin and subcutaneous tissues is supplied by the ventral rami of spinal nerves T-6 to L-1. The dermatomes of these nerves form “stripes” around the abdomen. T-6 is just below the xiphoid process. T-10 crosses the umbilicus. L-1 crosses the pubic bones.
Knowledge of abdominal wall dermatomes is useful for understanding referred pain from abdominal organs.
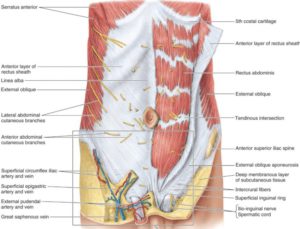
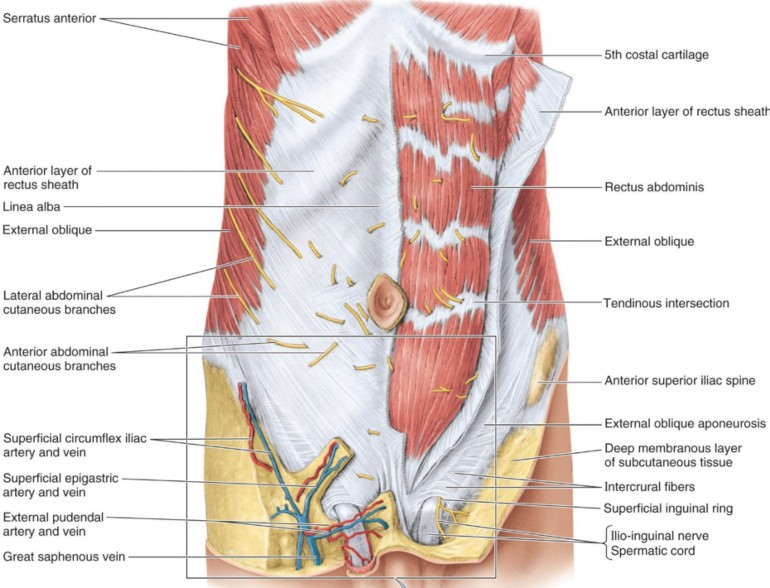
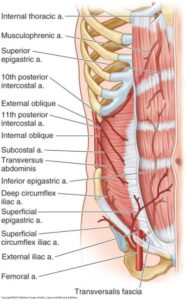
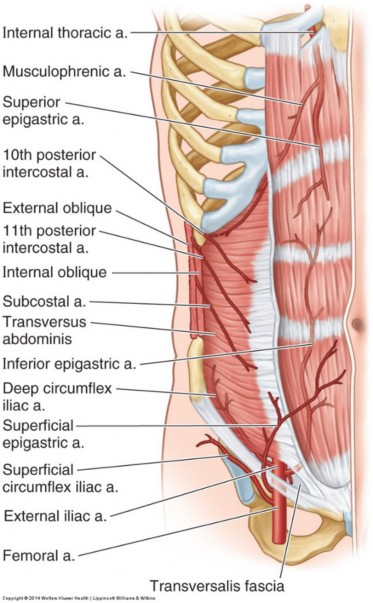
Figure 15.13 Blood supply of anterolateral abdominal wall. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIG. 2.12.
The blood supply is via the lower intercostal arteries, subcostal artery, and superior and inferior epigastric arteries. The inferior epigastric artery is a branch of the external iliac artery. It ascends behind the rectus abdominis muscle. The superior epigastric is a terminal branch of the internal thoracic artery. It descends behind the rectus abdominis muscle. Both epigastric arteries enter the rectus sheath, where they anastomose within the rectus abdominis muscle.
Neurovascular plane of abdominal wall. Like the thoracic wall, the segmental nerves (thoraco-abdominal nerves) and vessels of the abdominal wall pass between the second and third muscles layers = between the internal oblique and transversus abdominis. The epigastric vessels are not in the neurovascular plane, since they course within in the rectus sheath with the rectus abdominis.
Inguinal region
The inguinal region is the “groin region”: the area where the anterior abdominal wall meets the thigh. This area has clinical importance as it is a relatively weak region where abdominal contents can protrude through the body wall and present to the clinician as a hernia. The most important landmark in this region is the inguinal ligament.
Not a true ligament—it is the inwardly rolled (J-shaped) inferior margin of the aponeurosis of the external oblique muscle. It connects to the anterior superior iliac spine laterally and the pubic tubercle medially. Below, its curved margin fuses with the deep fascia of the thigh. Above, it is continuous with the flat aponeurosis of the external oblique muscle.
As it approaches the pubic tubercle medially, some of the fibers of the inguinal ligament pass downwards onto the superior ramus of the pubic bone. These fibers produce a sharp, crescent-shaped ridge called the lacunar ligament. This will be important later when we discuss femoral hernias.
The inguinal canal is a short passageway (~2 inches long) through the abdominal wall, oriented obliquely and parallel with the inguinal ligament. Both males and females have inguinal canals. In the male, it connects the abdominopelvic cavity with the scrotum. In females, it connects distally to the labium majus.
Openings of inguinal canal
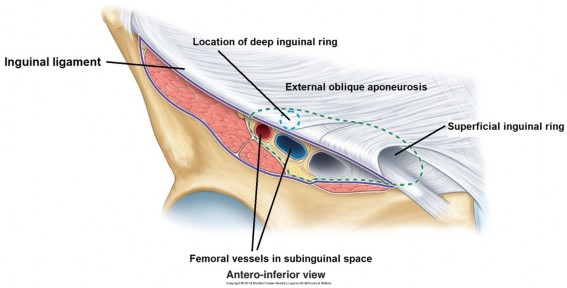
Internally, the inguinal canal begins at the deep inguinal ring. This opening is located just lateral to the origin of the inferior epigastric artery from the external iliac artery. On the surface of the body, the deep ring can be located above the inguinal ligament at the mid-inguinal point = halfway between the anterior superior iliac spine and the pubic tubercle. The femoral vessels are directly inferior to the deep ring at the mid-inguinal point. When viewed from within the body cavity, facing forward, and with the peritoneum removed, the deep ring resembles a “rabbit hole”—an oval opening in the transversalis fascia.
Externally, the inguinal canal terminates at the superficial inguinal ring. This is a triangular opening in the external oblique aponeurosis, located just medial to the pubic tubercle.
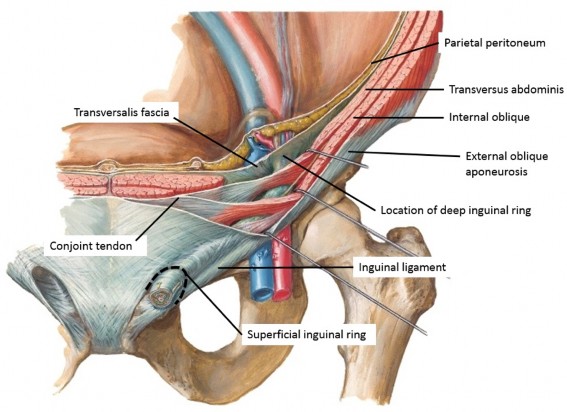
Walls of inguinal canal
Anterior: The external oblique aponeurosis.
Posterior: The transveralis fascia laterally and the conjoint tendon (merged aponeuroses of the transversus abdominis and internal oblique muscles) medially.
Inferior (floor): A fibrous trough, formed by the inwardly-rolled (J-shaped) margin of the external oblique aponeurosis.
Superior (roof): The inferior margins of the internal oblique and transversus abdominis muscles, arching over the deep inguinal ringand inguinal canal.
Internal oblique and transversus abdominis muscles in the inguinal region
Figure 15.15 Course of inguinal canal through abdominal wall. NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 263 ( ADAPTED).
The lower borders of the IO and TA muscles are unlike that of the external oblique = the IO and TA do notcontribute to the formation of the inguinal ligament nor do they produce a similar structure that parallels the inguinal ligament internally.
Instead, the lower (inguinal) borders of the IO and TA arch over the deep inguinal ring and the inguinal canal—probably a consequence of the development of the inguinal canal and the descent of the gonads (discussed in the next chapter). After arching over the deep inguinal ring, the aponeuroses of the IO and TA fuse medially. Most of this fused tendon passes in front of the rectus abdominis, contributing to the anterior layer of the rectus sheath (described earlier). The portion of the fused aponeuroses that is lateral to the rectus abdominis muscle inserts into the superior ramus of the pubic bone. This common attachment of the IO and TA on the pubic bone is referred to as the conjoint tendon (clinicians call it the “inguinal falx”). It is in the posterior wall of the inguinal canal, directly posterior to the superficial inguinal ring. It will figure into our discussion of direct inguinal hernias.
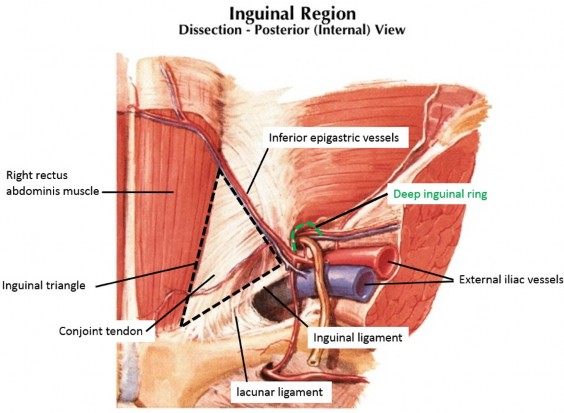
This clinically important area related to the inguinal canal has these borders (see Figure 15.16):
Medial: The lateral border of the rectus abdominis muscle
Lateral: Inferior epigastric vessels
Inferior: Inguinal ligament
Note that the inguinal canal passes across the lower part of the inguinal triangle and the structures that make up the posterior wall of the inguinal canal (conjoint tendon and transversalis fascia) fill the inguinal triangle.
take-home message
The inguinal triangle, containing the transversalis fascia and conjoint tendon, is poorly reinforced and a potentially weak area of the anterior abdominal wall.
Atrophy of abdominal wall muscles that further weakens this area is a predisposing factor for <b?direct inguinal hernia (discussed here).
Figure 15.16 Posterior aspect of anterior abdominal wall/ Inguinal region. Internal view. NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 262 (ADAPTED).
Contents of the inguinal canal
Spermatic cord in males; round ligament in females
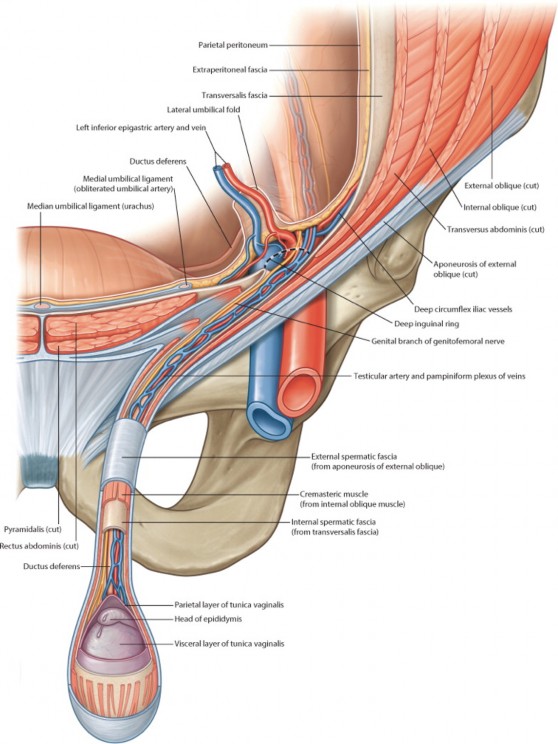
Figure 15.17 Contents of spermatic cord. GRAY’S ATLAS OF ANATOMY, 2ND ED.
The spermatic cord contains structures that run to and from the testes, surrounded by fascial coverings. The spermatic cord suspends the testes within the scrotum, like the rod that supports the pendulum in a grandfather clock. The major contents of the spermatic cord are:
Ductus deferens (vas deferens): The sperm carrying tube. It connects the epididymis (in the scrotum) to the ejaculatory duct (in the pelvic cavity—within the prostate). The ductus deferens is thick and can be easily identified by palpation within the spermatic cord as a firm, wire-like cord. In cross-section, it has a thick, muscular wall with a tiny lumen, the walls being filled with layers of smooth muscle. Sympathetic stimulation causes contraction of the muscle and propels the sperm toward the prostate.
Artery of the ductus deferens: A small branch of the internal iliac artery, it enters the deep inguinal ring from the pelvic cavity. It supplies the ductus deferens and distally, the epididymis.
Testicular artery: A long, thin, graceful branch of the abdominal aorta originating at L-2. It passes downward behind the peritoneum to the deep inguinal ring and traverses the inguinal canal. It’s origin high in the lumbar region is a reminder of the developmental origin of the testes (they descend).
Pampiniform plexus (pampiniform = shaped like a vine or tendril): a network of thin veins that surround the testicular artery in the spermatic cord. These ascend into the inguinal canal where they merge to form a testicular vein. The testicular vein ascends in the posterior abdominal wall alongside the testicular artery. On the right side, it is a tributary of the inferior vena cava. The left testicular vein drains to the left renal vein. The function of the pampiniform plexus is presumably to cool the blood within the testicular artery. Blood at core body temperature is too warm for spermatogenesis to occur properly in the testes.
Fascias of the spermatic cord: Three layers of fascia surround the contents of the spermatic cord and distally they also surround the testis and epididymis. These are derived from layers of the anterior abdominal wall during the process of testicular descent (described in the next chapter). From the external to internal:
External spermatic fascia: Derived from the fascia of the external oblique muscle.
Cremasteric fascia: Derived from the fascia of the internal oblique muscle. Contained within the cremasteric fascia are loops of skeletal muscle fascicles that produce the cremaster muscle. Its function is to elevate the testes and bring them closer to the trunk—a heat preserving function.
Internal spermatic fascia: A thin layer derived from the transversalis fascia (not the transversus abdominis muscle—it has no contribution to the coverings of the spermatic cord).
This is a fibrous, vestigial structure: a remnant of the female gubernaculum (an embryonic “guide-wire” that guides the descent of the ovary—discussed in the Descent of the Gonads). It leaves the uterus and travels under the peritoneum to the deep inguinal ring, traverses the inguinal canal, then leaves the superficial inguinal ring. In the perineum, it merges with dense connective tissue in the labium majus. As it passes through the body wall it acquires the same fascial coverings as the spermatic cord—they fuse to the round ligament and cannot be discerned separately.
A branch of the lumbar plexus, it is derived from the ventral ramus of L-1 spinal nerve. Like the other segmental nerves of the abdominal wall, it passes through the neurovascular plane and then drops down into the inguinal canal between the internal oblique and transversus abdominis (thus, this sneaky nerve does not enter the deep inguinal ring). The ilioinguinal nerve exits the superficial inguinal ring (outside the spermatic cord, not within it) to supply the skin of the upper thigh and anterior scrotum/labia majora.
Clinical correlation
Vasectomy is a form of birth control in which a segment of the ductus deferens is removed and the resulting proximal and distal ends of the transected tube are sealed shut with stitches, clips, or cautery. The ductus deferens is accessed through the upper scrotum, below the superficial inguinal ring, by incising the skin or via a “no-scalpel” technique with a special punch tool.
The scrotum
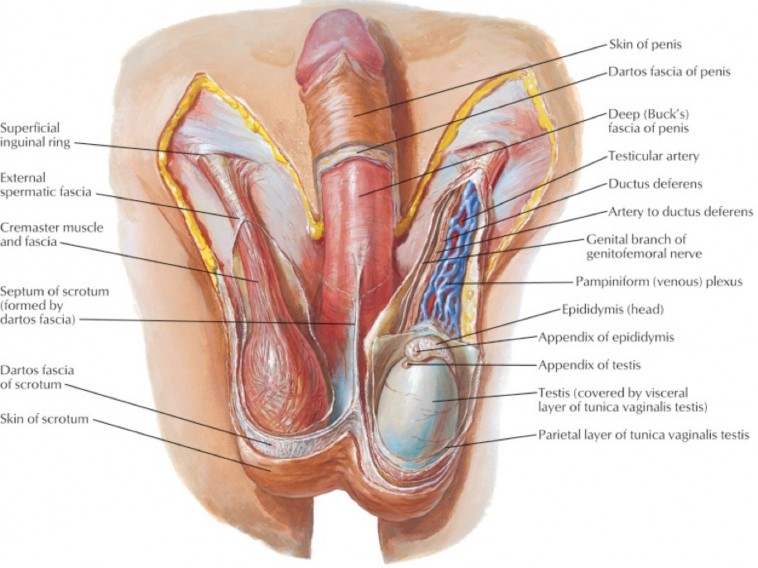
Figure 15.18 Scrotum and its contents. NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 369.
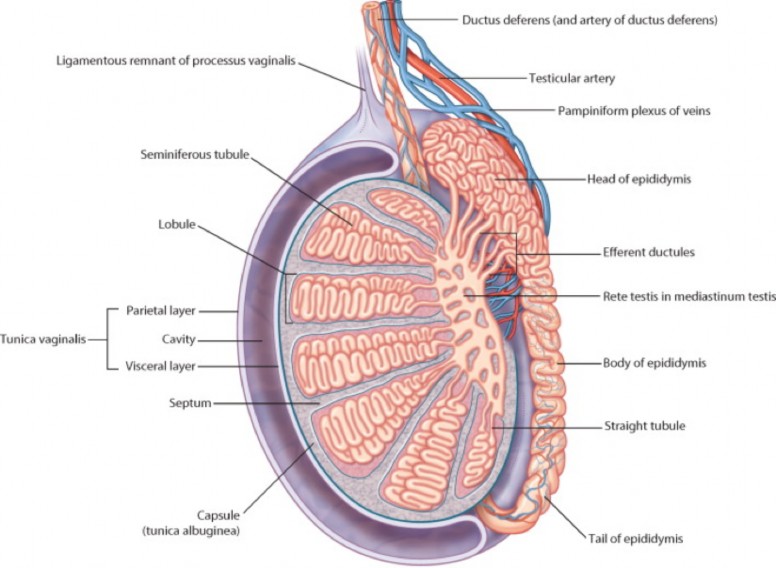
Figure 15.19 Cross section of testis and epididymis. GRAY’ S ATLAS OF ANATOMY, 2ND ED.
The scrotum is a sac made from skin and superficial fascia that hangs from the perineum (the region between the thighs). It is part of the male external genitalia.
Scrotal skin
The appearance of the scrotal skin varies depending on the state of the smooth muscle deep to the skin. This produces either a smooth or wrinkled texture. The scrotal raphé is the midline ridge in the skin that indicates the site of fusion of the embryonic tissues that form the scrotum.
Superficial fascia
The superficial fascia of the scrotum is called the dartos. It is continuous above with the membranous layer of superficial fascia (Scarpa’s fascia) in the abdominal wall. The scrotum has no fatty layer of superficial fascia (that would make things too warm!). The dartos muscle consists of smooth muscle fascicles that insert into the dermis of the skin. Sympathetic stimulation causes the dartos to wrinkle the scrotal skin when the temperature drops. This along with elevation of the testes by the cremaster muscle keeps the testes close to the trunk, reducing heat loss.
Contents of the scrotum
Testes
The male gonads. They function to make the male gametes (reproductive cells) called spermatozoa and the hormone testosterone. Each testis is oval—presenting round superior and inferior poles. Vessels, nerves, and sperm ducts enter and leave the testis through a portal on its posterior surface called the mediastinum of the testis. The testis is surrounded by a thick, fibrous capsule—the tunica albuginea (Latin = white coat).
Epididymis
(Greek = next to the testis): A C-shaped convoluted tube located posterior and lateral to each testis, it has a head, body, and tail. The head is located next to the superior pole of the testis. It receives sperm ducts (efferent ductules) from the mediastinum of the testis. These unite in the head to form a single duct of the epididymis. The duct is highly coiled as it passes through the body to the tail. The tail of the epididymis, located near the inferior pole of the testis, is continuous with the ductus deferens. Sperm mature in the epididymis and become motile.
Tunica vaginalis
A serous sac located on the anterior surface of each testis and epididymis. The tunica vaginalis is derived from the processus vaginalis—a diverticulum of the peritoneal cavity that grows into the scrotum during embryonic development.
Visceral layer of the tunica vaginalis
The visceral layer of the tunica vaginalis is applied to the anterior surface of the testis (and epididymis), where it is glued to the tunica albuginea.
Parietal layer of tunica vaginalis
The parietal layer of tunica vaginalis is fused to the internal spermatic fascia. The mesothelial surfaces of the two layers of the tunica vaginalis essential touch each other, separated by a thin layer of serous fluid. Sound familiar? It should!
Clinical correlation
The tunica vaginalis normally does not communicate with the peritoneal cavity (since the proximal part of the processus vaginalis normally obliterates).
If the tunica vaginalis in the scrotum remains connected to the peritoneal cavity, this is called a patent processes vaginalis. This is a predisposing factor for indirect inguinal hernia (discussed here).
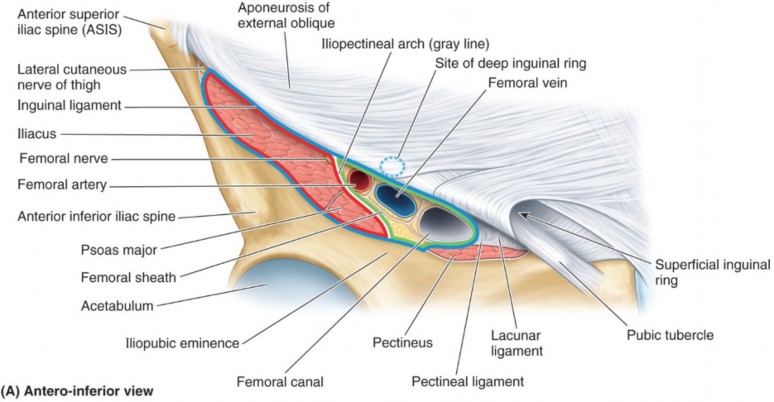
The subinguinal space is a passageway behind the inguinal ligament that connects the abdominal cavity and lower limb. Through it pass muscles, nerves, and vessels that convey both blood and lymph.
The lateral part of the subinguinal space is occupied by the iliopsoas muscle and femoral nerve.
The medial part contains the femoral vessels and a “potential space” filled with loose connective tissue and a few lymph nodes. This is called the femoral canal. This is a potentially weak area that is the site of femoral hernias (discussed below).
A handy mnemonic
for remembering the structures in the subinguinal space, from lateral to medial, is “NAVEL” (like the orange, or your “belly button”):
Nerve
Artery Vein Empty Space with Lymphatics
The nerve, artery, and vein are all named “femoral.” The “empty space” refers to the femoral canal, medial to the femoral vein.
Realize that the femoral artery and vein are continuous proximally with the external iliac artery and vein—they are the same vessels; only the names have changed.
Hernias associated with the inguinal region
A hernia is defined as: the protrusion of a structure through an opening it normally does not pass through. Hernias in the groin region above the inguinal ligament are inguinal hernias—those below the inguinal ligament are femoral hernias. The important thing to understand is that these hernias occur in areas where the body is inherently weak due to embryology (congenital weakness) or becomes weak through aging and disease (acquired weakness), or perhaps due to both.
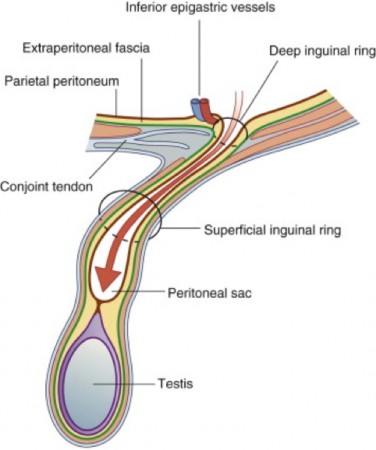
Inguinal hernias are the most common type of abdominal hernias. They can occur in both sexes but are much more common in males due to the size of the inguinal canal. Inguinal hernias are of two types: indirect and direct. In both cases, the herniating tissue is either bowel or mesenteric fat, surrounded by a sac made of parietal peritoneum.
Herniating tissue enters the abdominal wall lateral to the inferior epigastric vessels.
Hernia enters the inguinal canal through the deep inguinal ring. This is considered “indirect” access to the inguinal canal.
Hernia exits inguinal canal through superficial inguinal ring, within the spermatic cord.
Can be congenital (due to a patent processus vaginalis) or acquired (body wall weakness—without patent processus vaginalis).
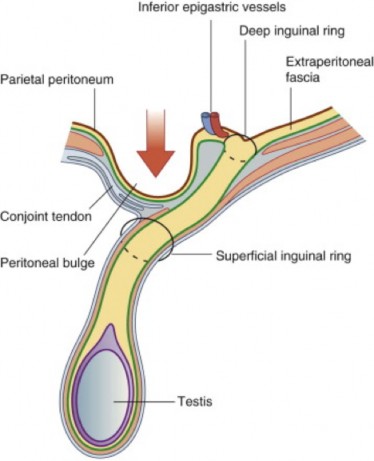
Figure 15.22 Direct inguinal hernia. Gray’s Anatomy for Students, 3rd ed., Fig. 4.49.
Less common than indirect.
Herniating tissue enters the abdominal wall through the inguinal (Hesselbach’s) triangle, medial to the inferior epigastric vessels. The hernia pushes into the inguinal canal though its posterior wall.This is considered “direct” access to the inguinal canal. A “DIRECT HIT”!
Hernia exits inguinal canal through the superficial inguinal ring, but outside (next to) the spermatic cord, not within it.
Direct inguinal hernias are always acquired, due to weakening of tissues in the inguinal triangle.
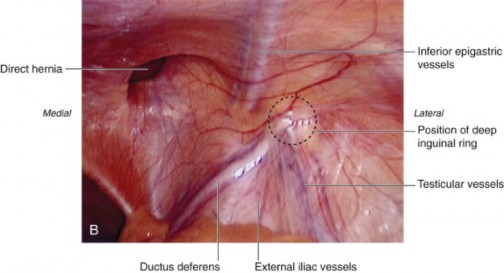
Figure 15.23 Laparoscopic view of direct inguinal hernia. Internal view: Posterior surface of anterior abdominal wall. Gray’s Anatomy for Students, 3rd ed., Fig. 4.50.
Summary table: Direct vs. indirect inguinal hernias
Both types of inguinal hernias present as lumps in the inguinal region and both types can emerge through the superficial inguinal ring. Additional terms used to classify inguinal hernias:
Complete
Hernia exits superficial inguinal ring; may extend into the scrotum.
Incarcerated
Hernia cannot be returned to the abdominal cavity (irreducible).
Reducible
Hernia can be pushed back into the abdominal cavity manually.
Strangulated
Blood supply of herniated bowel pinched off. Medical emergency.
Table 15.1
Characteristics
Direct (Acquired)
Indirect (Congenital)
Predisposing factors
Weakness of anterior abdominal wall in inguinal triangle(e.g., owing to distended superficial ring, narrow conjoint tendon, or attenuation of aponeurosis in males >40 years of age)
Patency of processus vaginalis (complete or at least of superior part) in younger persons, the great majority of whom are males
Frequency
Less common (one third to one fourth of inguinal hernias)
More common (two thirds to three fourths of inguinal hernias)
Coverings at exit from abdominal cavity
Peritoneum plus transversalis fascia (lies outside inner one or two fascial coverings, parallel to cord)
Peritoneum of persistent processus vaginalis plus all three fascial coverings of cord/round ligament
Course
Usually traverses only medial third of inguinal canal,external and parallel to vestige of processus vaginalis
Traverses inguinal canal (entire canal if it is sufficient size) within processus vaginalis
Exit from anterior abdominal wall
Via superficial ring, lateral to cord; rarely enters scrotum
Via superficial ring inside cord, commonly passing into scrotum/labium majus
FROM MOORE ET AL., CLINICALLY ORIENTED ANATOMY, TABLE 4.3.
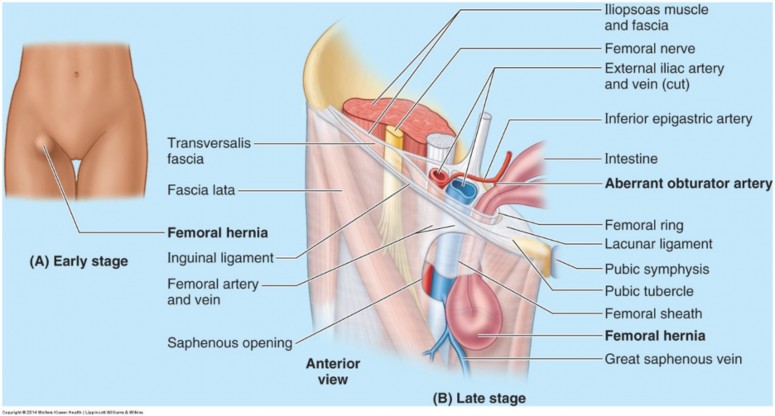
Femoral hernias
Occur below inguinal ligament, in the subinguinal space, within the femoral canal.
More common in women, due to the larger size of the femoral canal (wider hips) and smaller size of inguinal canal.
Are always acquired.
Can be distinguished from inguinal hernias by their location below the superficial inguinal ring.
Can be at risk for strangulation due to sharp margin of the lacunar ligament (described earlier), which is adjacent and medial to the femoral canal.