The gonads are the organs that produce gametes (reproductive cells). In the female the gonads are the ovaries. They produce oocytes (ova). The male gonads are testes. They produce sperm.
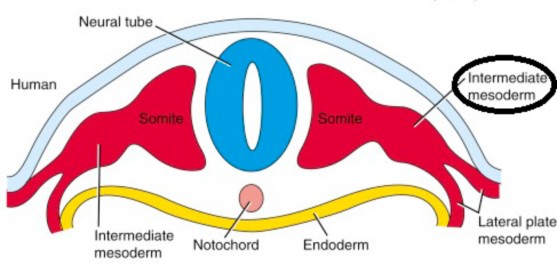
The gonads form from intermediate mesoderm in the upper lumbar region of the posterior abdominal wall.
Both male and female gonads descend from their original position during development. However, the testes descend much further, out of the body cavity and into the scrotum. The reason: sperm maturation can’t occur at core body temperature (37°C). In the scrotum, testicular temperature is about three degrees cooler (34°C).
Descent of the testes
Figure 16.2
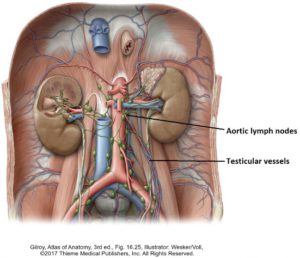
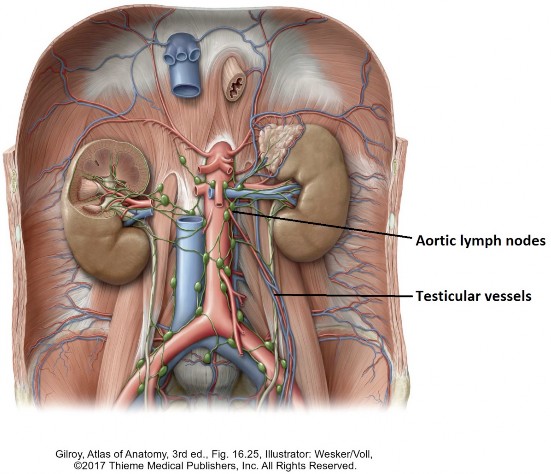
The testes acquire their blood supply, innervation, and lymphatic drainage prior to their descent. They also become associated with the mesonephric ducts. The mesonephric duct will give rise to the ductus deferens, the sperm-carrying duct. Therefore, when the testes descend, they bring with them the elements of the spermatic cord (ductus deferens, vessels, and nerves). This is why the testicular vessels (arteries and veins) are so long and delicate, extending from L-2 through the inguinal canal and in to the scrotum.
An important concept
The lymphatic drainage of the testes follows the blood vessels retrograde—thus the lymph nodes associated with the testes are on the posterior abdominal wall and NOT in the vicinity of the scrotum.
Clinical correlation
Testicular cancer is the most common cancer of males ages 18–40, and also one of the most curable cancers. It usually arises as tumors of the germ cells = the cells that will go on to become sperm. Testicular cancer spreads via lymphatic vessels to the aortic nodes on the posterior abdominal wall. This is why staging of testicular cancer is done with imaging of the abdomen (CT or MRI).
Figure 16.3 LARSEN’ S HUMAN EMBRYOLOGY, FIGURE 16-25.
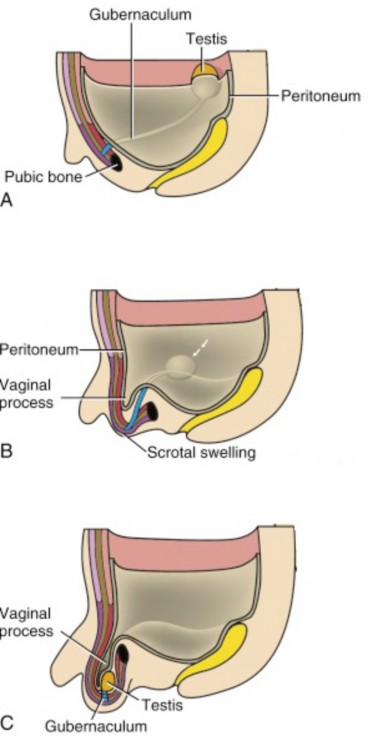
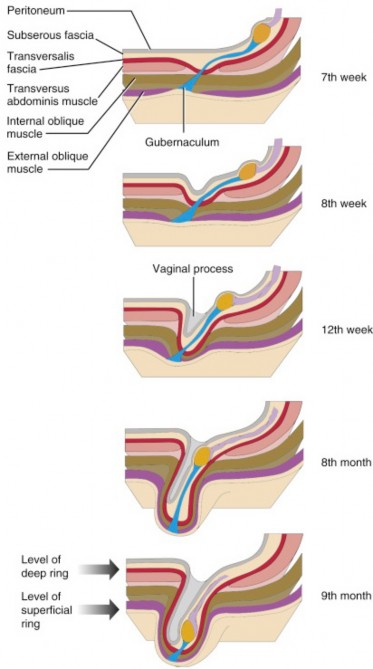
and they reach the area of the deep inguinal ring by Week 12. They stay there for quite some time, finally moving into the scrotum by the 9th month of development.
The gubernaculum (Latin = helm), a ligamentous cord located in the fascia of the posterior abdominal wall external to the parietal peritoneum, is thought to be a guide for testicular descent. There is some debate on whether or not the gubernaculum actively shortens in order to move the testes. Some authors believe this is so. Proximally the gubernaculum attaches to the caudal pole of the testis. Distally it attaches to the scrotal swelling. Let’s be clear that the testes and gubernaculum are retroperitoneal—they are located behind the peritoneal sac.
Clinical correlation
Failure of the testis to descend into the scrotum is called cryptorchidism. If a testis remains in the abdomen, it leads to sterility. This affects 3% of full term and 30% of preterm male infants. The majority spontaneously correct by 3 months of age. Orchiopexy (fixing the testis to the scrotum surgically) is performed if descent doesn’t occur by 4 months of age. This is to preserve fertility and to decrease the risk of testicular cancer in adulthood. The risk of cancer in an undescended testis is much higher than the general population (5–10 times higher). Cryptorchidism may be caused by insufficient androgen production.
This is the processus vaginalis (vaginal process). Its development precedes testicular descent and carves out the inguinal canal and its deep and superficial inguinal rings. See Figure 16.4. Thus, a passageway in the abdominal wall is ready and waiting for the testes as they move into the scrotum. After the testes descend, the inguinal canal shrinks.
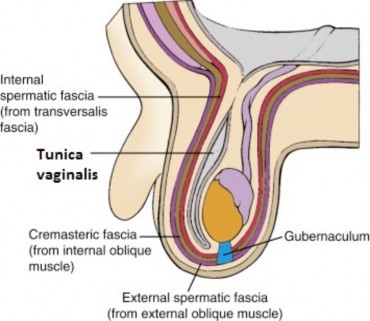
closing the connection to the peritoneal cavity. See Figure 16.5. Distally, the processes vaginalis remains as a sac on the ventral surface of the testis. This is the tunica vaginalis. The part of the tunica vaginalis applied to the outer surface of the testis is the visceral layer. Deep to the visceral layer is the capsule of the testis itself (tunica albuginea). The part of the tunica vaginalis not applied to the testis is the parietal layer. This should sound familiar since the tunica vaginalis is a serous sac. Note that after descent is completed, the testis is in the same relative location as it was on the posterior abdominal wall, since the tunica vaginalis is the equivalent of the peritoneal sac and the testis is dorsal to it.
it causes the layers of the abdominal wall to follow suit and be drawn out into the scrotum, forming the fascial layers of the spermatic cord, as well as the cremaster muscle. The layers of the abdominal wall and their counterparts in the scrotum and spermatic cord are summarized in Figure 13.1, from superficial to deep.
Table16.1
Anterior abdominal wall
Counterpart in scrotum/spermatic cord
Skin
Skin of scrotum
Membranous layer of superficial fascia (Scarpa’s)
Dartos fascia and muscle (in scrotum)
Fascia of external oblique muscle
External spermatic fascia
Internal oblique fascia and muscle
Cremasteric fascia and cremaster muscle
Transversus abdominis muscle
None
Transversalis (internal) fascia
Internal spermatic fascia
Peritoneum
Tunica vaginalis
Additional notes
The fatty layer of the superficial fascia (Camper’s) and the transversus abdominis muscle
of the abdominal wall are not represented by equivalent layers in the scrotum or in the spermatic cord.
The cremaster and dartos muscles protect the testis from excessive cold:
the cremaster by pulling the testis up toward the warm body, and the dartos by crinkling (thus thickening) the scrotal skin. Note that the dartos is smooth muscle innervated by sympathetic fibers, whereas the cremaster is skeletal muscle, innervated by the genital branch of the genitofemoral nerve (from the lumbar plexus, spinal nerves L-1 and L-2).
The cremasteric reflex is elicited by stroking the inside of the thigh proximally, near the scrotum.
Afferent signals are sent to the CNS via L-1. Efferent signals are sent to the cremaster muscle via the genito-femoral nerve (L-1 and L-2). This elevates the testes in response to the stroking. Young boys may have an over-active cremasteric reflex that raises the testis into the inguinal canal, giving a false impression of an undescended testis.
Figure 16.4 LARSEN’ S HUMAN EMBRYOLOGY, FIGURE 16-25.
Figure 16.5 LARSEN’ S HUMAN EMBRYOLOGY, FIGURE 16-27.
Clinical correlation
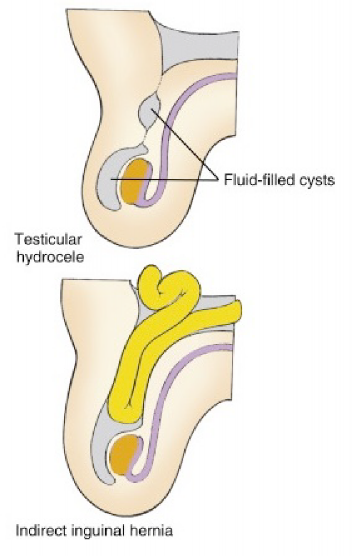
Normally the lumen of the tunica vaginalis is collapsed with only a small amount of lubricating serous fluid present. Under pathologic conditions (inflammation, irritation, or injury) it may fill with fluid, forming a hydrocele.
If the connection between the processus vaginalis and the peritoneal cavity does not close after birth, a patent processus vaginalis is present. This can predispose one to herniation of bowel or mesentery into the scrotum, called a congenital indirect inguinal hernia.
Figure 16.6 LARSEN’ S HUMAN EMBRYOLOGY, FIGURE 16-26.
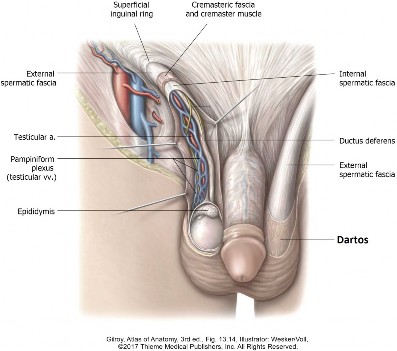
Review: Contents of the spermatic cord
Figure 16.7
Ductus deferens (vas deferens)
The sperm-carrying duct. Enters the pelvis from the inguinal canal via the deep inguinal ring. Ends at the prostate, where it joins with the duct of the seminal vesicle to form the ejaculatory duct. Its walls are thick and muscular to propel the sperm.
Testicular artery
Supplies blood to the testis and epididymis. Arises from the abdominal aorta at the level of L-2. Enters the deep inguinal ring and becomes a part of the spermatic cord.
Pampiniform plexus (Latin = tendril, like a vine)
Tributaries of the testicular vein. Consists of many tortuous veins that wrap around the testicular artery. Acts to extract heat from the blood in the testicular artery, so it’s not too hot when it reaches the testis.
Autonomic nerves
Sympathetic nerve fibers derived from the lesser splanchnic nerves (T-10 and T-11) lie along the ductus deferens. They fire during ejaculation and stimulate the muscle wall of the ductus to propel the sperm toward the pelvic cavity. Sympathetic nerve fibers also control the blood flow of the testicular artery.
Pain sensations from the testis are carried by visceral afferent fibers that run with the autonomics. The testes are very sensitive to pressure – pain is localized in the scrotum or referred to the lower back.
Lymphatic vessels
in the spermatic cord travel with the testicular vessels to drain into the aortic lymph nodes at the level of L-2.
Clinical correlation
Enlarged, varicose veins of the pampiniform plexus are called a varicocele. Patients describe it as a heavy sensation in the scrotum and upon physical exam it feels like a “bag of worms.” Although they are often harmless, they can cause sterility, presumably because they interfere with testicular thermoregulation. They are more common on the left side since the left testicular vein drains to the left renal vein and not the IVC. Thus, it is more vertical in orientation, so the blood is more likely to pool in the pampinform plexus on that side. An isolated right sided varicocele should be investigated, as it could be due to an obstruction by tumor or mass!
Clinical correlation
Testicular torsion occurs when a testis rotates, twisting the spermatic cord within the scrotum. This is most likely to occur in adolescents. It causes sudden, severe pain and a testis that is positioned higher than normal. Testicular torsion is a medical emergency requiring prompt attention, since it constricts the testicular artery and can lead to ischemia and possibly permanent damage and loss of the testis. Risk factors are age, previous testicular torsion, and family history of testicular torsion.
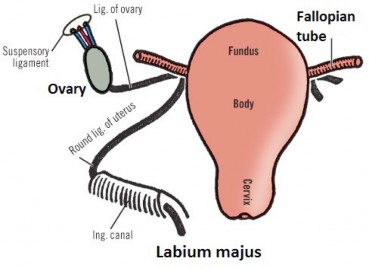
As the vaginal process grows into the body wall, it carves out the inguinal canal, which contains the gubernaculum. Proximally the gubernaculum attaches to the ovary; distally it attaches to connective tissue within the labium majus (the female structure homologous to the scrotum in males).
Here their descent is arrested as the gubernacula become tethered to the primordia of the uterus (the paramesonephric ducts) and get caught up in the broad ligament of the uterus. The part of the gubernaculum between ovary and uterus becomes the fibrous ovarian ligament in the adult. The part of the gubernaculum passing from uterus to inguinal canal to labium majus becomes the round ligament of the uterus.
(arising from the abdominal aorta way up at L-2), the blood supply to the ovaries is from two sources, presumably because their descent is arrested in the pelvis and their development is associated with other organs there. The ovaries receive blood via (1) the ovarian arteries, which arise from the abdominal aorta and descend along the posterior abdominal wall (like the testicular arteries), then reach the ovaries through a layer of peritoneum called the suspensory ligament of the ovary, and (2) an ovarian branch of the uterine artery (the uterine artery arises from the internal iliac artery in the pelvic cavity).
so it follows a couple of pathways (unlike the testes): to aortic nodes in the posterior abdominal wall (like the testes) and to internal iliac nodes in the pelvis. This is a consideration when treating ovarian cancer.
Clinical correlation
Stretching of the round ligament by the growing uterus in pregnancy can cause significant pain in the groin and pelvis that can mimic uterine contractions. It is a diagnosis of exclusion (i.e., no other causes—such as preterm labor, appendicitis, etc.) and is managed symptomatically.