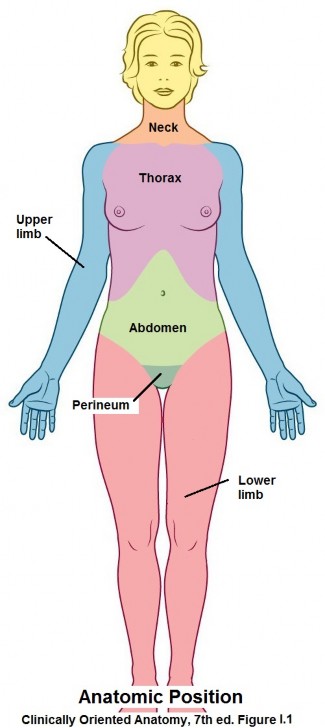
The anatomic position (Figure 1.1) is used as the reference for all of the terms of description in gross anatomy. You will have to place yourself in this position or imagine yourself assuming this position in order to understand anatomic terminology.
It’s imperative that you gain a handle on the terms of relationship, terms describing movements, and anatomic planes used in anatomy fairly quickly (see Table 1.1, Table 1.2, and Table 1.3 for a list of terms). Anatomy is a descriptive science, so the accurate use of anatomic terms is important in order to avoid confusion and to communicate effectively with your colleagues and associates.
The head and neck
The trunk
The limbs: Upper and lower
A single layer of cells called a mesothelium lines the inside of the body wall and also covers the outer surfaces of many of the visceral organs contained within the thoracic and abdominopelvic cavities. The mesothelium and the supporting connective tissue underlying it make up what is called a serous membrane. Serous comes from the term “serum”—which means “whey” = a clear watery fluid. Indeed, serous membranes secrete serous fluid, which makes them slippery. Serous membranes allow visceral organs and the body wall to move about without producing friction when they rub against one another.
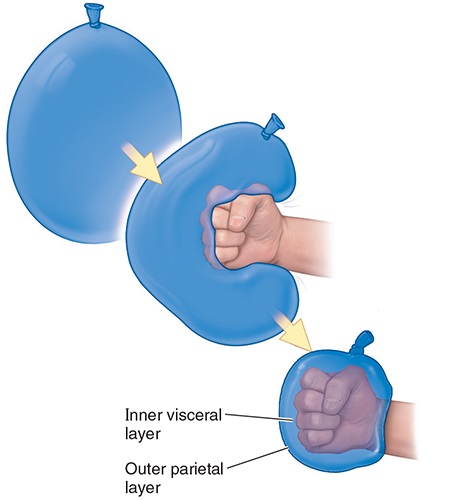
The arrangement of the serous sacs within the thoracic and abdominopelvic cavities can be modeled with an inflated balloon and your fist pushed into the balloon (Figure 1.4). The balloon is the serous membrane while the fist represents a visceral organ (lung or heart for example)—note that the part of the balloon’s surface that is away from the fist is curved and is the serous membrane that lines the inside of the body wall, while the part of the serous membrane in contact with the fist (i.e., the organ) conforms to the shape of the fist—the important point is that these two parts of the serous membrane are continuous and have a small space between them.
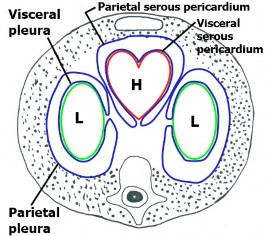
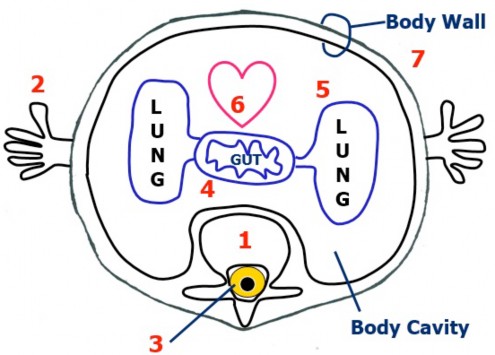
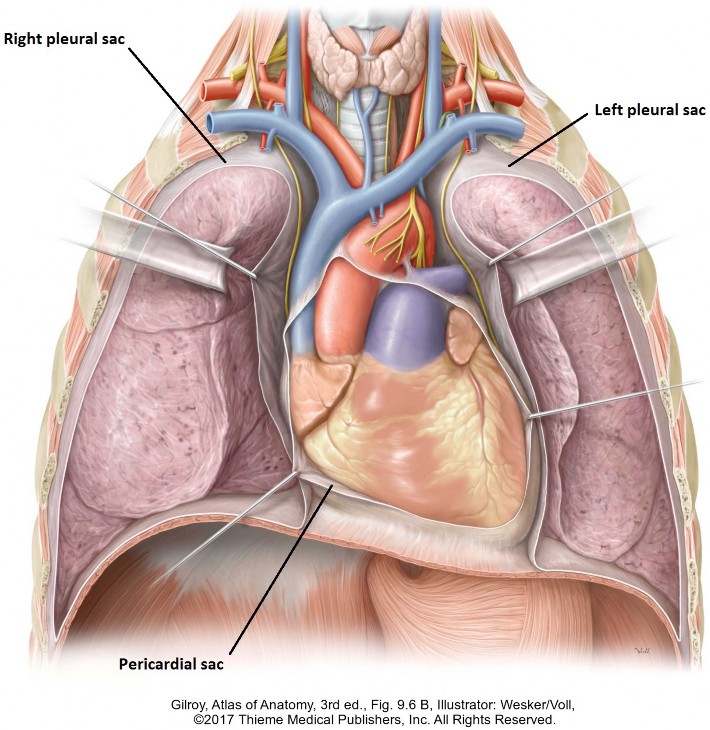
The thoracic cavity contains three serous sacs: two associated with the lungs and one with the heart. (See Figures 1.5 and 1.6.)
-
- The pleural sacs are serous sacs that surround the left and right lungs (pleur: a term denoting a relationship to the ribs or “the side” of the body). Note that there are two separate pleural sacs = right and left. Each pleural sac has a serous membrane called pleura and a cavity called the pleural cavity. The parietal pleura lines the inside of the thoracic body wall. The visceral pleura is the outer layer of the lung. The pleural cavity is a narrow space between the parietal and visceral layers of pleura, containing serous fluid. Do you see that the parietal and visceral layers of pleura face each other?
- The serous pericardium is the serous sac around the heart. It has parietal and visceral layers, separated by a pericardial cavity. More on this when we discuss the heart.
The serous membrane here is called peritoneum (periteino– = to stretch over). The parietal peritoneum lines the inside of the abdominal body wall. The visceral peritoneum is the serous membrane on the outer surface of abdominal organs. The peritoneal cavity is between the parietal and visceral layers of peritoneum, containing serous fluid. Later on, you will see that the arrangement of peritoneum is much more complex than the serous membranes associated with the heart and lungs—BUT THE CONCEPT IS THE SAME!
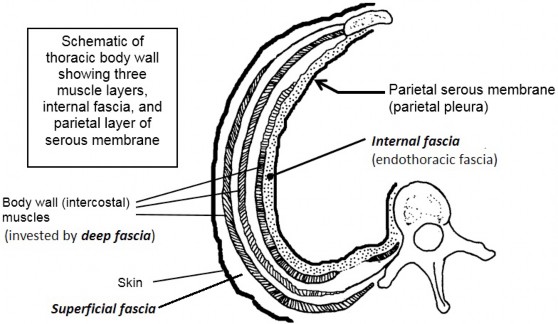
- Fascia is dense connective tissue arranged in sheets and tubes throughout the body. It functions to bind together and support tissues and organs. Fascia serves to organize and compartmentalize the body into layers, forming “planes” that allow parts and layers to glide over one another. You will observe this layering when you dissect the cadaver. Fascia is a friend, allowing the dissector to separate layers of muscles and define planes containing nerves and blood vessels.
- Fascia has great importance to the surgeon in dividing and reflecting layers. Some fascia is thick enough to place sutures in. Fascia has clinical implications in walling-off or restricting the spread of infections and confining the growth of tumors.
- Fascia is is ubiquitous. It attaches to bones and cartilage and encloses visceral organs and muscles. The problem lies in the naming = anatomists love to name things, and sometimes naming schemes are inconsistent. Worse, different authors have different interpretations and thus different names for fascial layers, including using eponyms (e.g., Scarpa’s fascia) instead of descriptive names (e.g., membranous layer of superficial fascia). We will try to be consistent and keep things as simple as possible.