 The kidneys tend to be innocent bystanders that suffer secondary to systemic illness or failure from another organ system. Acute kidney injury is extremely common in the hospital.
The kidneys tend to be innocent bystanders that suffer secondary to systemic illness or failure from another organ system. Acute kidney injury is extremely common in the hospital.
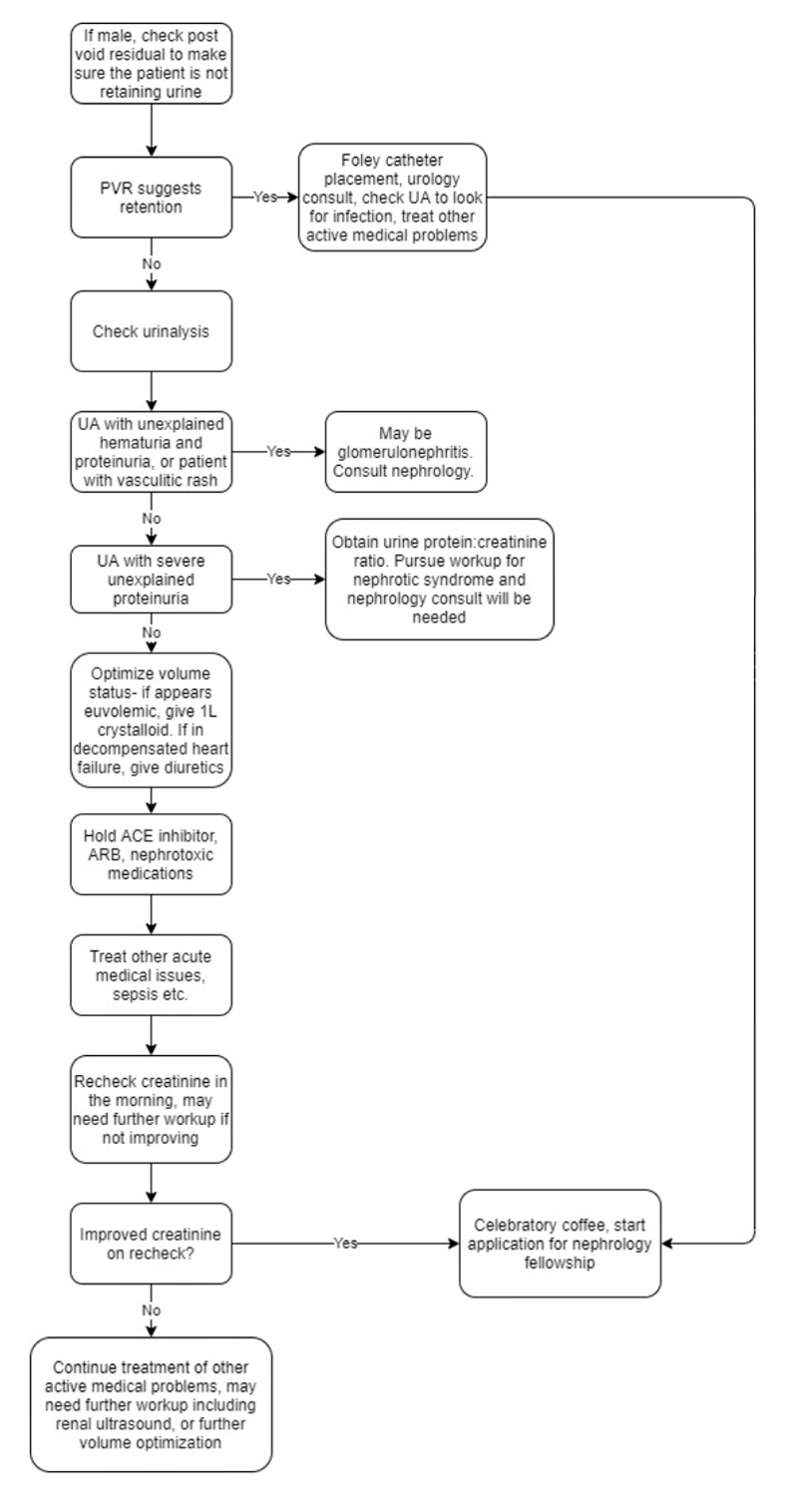
The first question to ask yourself is whether or not the patient needs emergent dialysis. The answer is almost always No. Here is a helpful mnemonic to help you decide if a patient needs emergent dialysis.