- For patients without cardiogenic pulmonary edema, escalation of oxygen therapy should be as follows: nasal cannula high flow nasal cannula (HFNC, may need a non-rebreather mask until HFNC is in place) intubation.
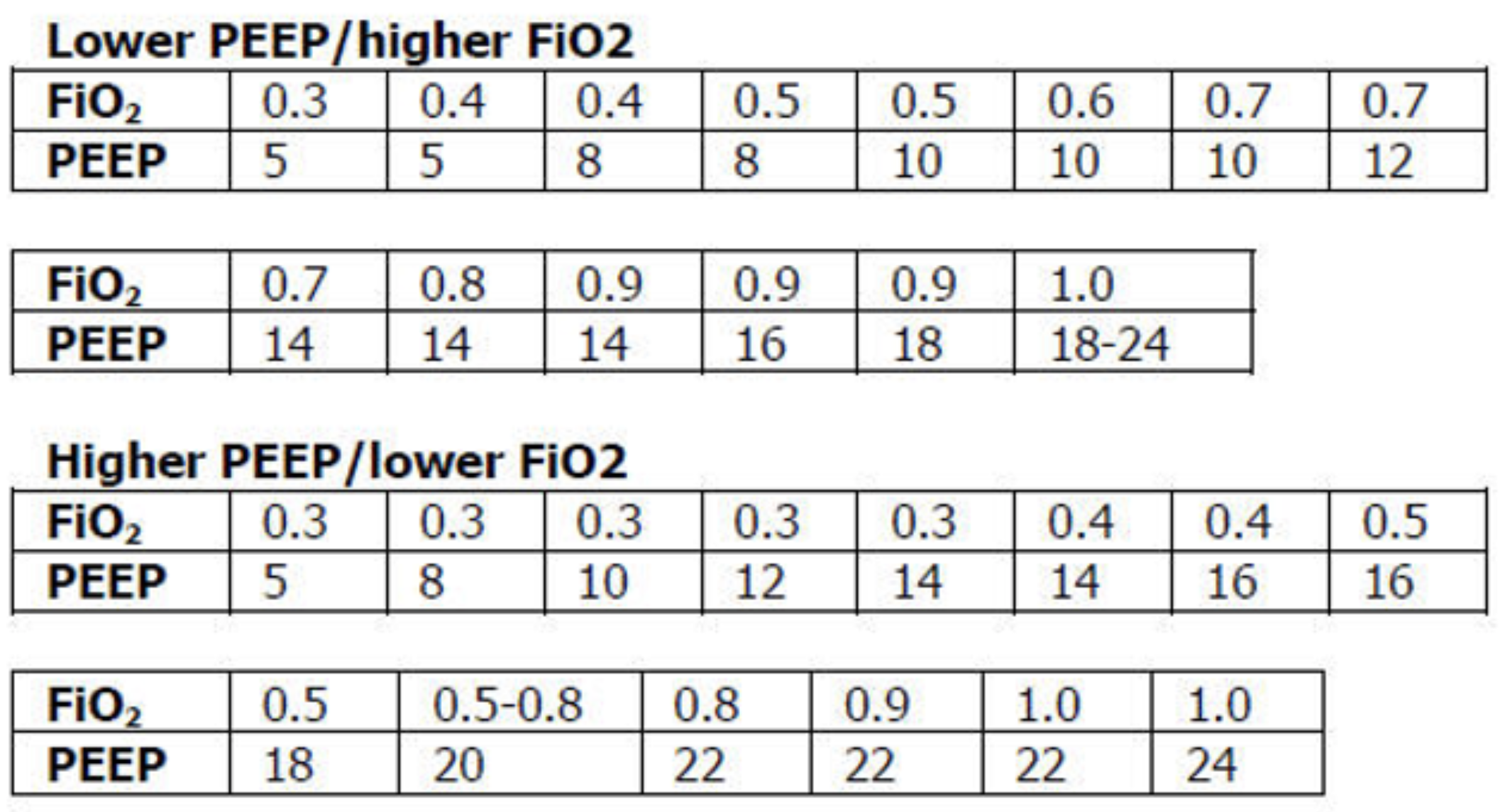
- If your patient needs to be intubated for ARDS and they are persistently hypoxemic, escalate their PEEP and oxygen using the “PEEP ladder” (below), and consider prone positioning and neuromuscular blockade if they have severe ARDS or refractory hypoxemia.
- For patients with cardiogenic pulmonary edema, escalation of oxygen therapy should be nasal cannula CPAP intubation.
- Don’t over-oxygenate the patient. Keep the oxygen level above >92% and <98% in most cases.
- To improve hypercarbia, the patient needs to breathe a greater total volume of air per minute to “blow off” their CO2. This can be done with BiPAP or mechanical ventilation.
- If BiPAP is not lowering the CO2, try troubleshooting by increasing the driving pressure (inspiratory pressure minus expiratory pressure, this is often done by increasing the inspiratory pressure), respiratory rate, or improving mask fit. Work with the RT on this.