 Briefly, unless the patient has a specific condition that requires blood pressure management (acute stroke, aortic dissection, etc.) or a change in their clinical status, hypertension in the hospital should not be treated quickly. This runs counter to the old dogma that significantly elevated BP (systolic over 180), needs to be urgently lowered. I would even argue that “hypertensive urgency” is not a real diagnosis (although hypertensive emergencies certainly exist). The difference is that a hypertensive emergency involves end organ damage.
Briefly, unless the patient has a specific condition that requires blood pressure management (acute stroke, aortic dissection, etc.) or a change in their clinical status, hypertension in the hospital should not be treated quickly. This runs counter to the old dogma that significantly elevated BP (systolic over 180), needs to be urgently lowered. I would even argue that “hypertensive urgency” is not a real diagnosis (although hypertensive emergencies certainly exist). The difference is that a hypertensive emergency involves end organ damage.
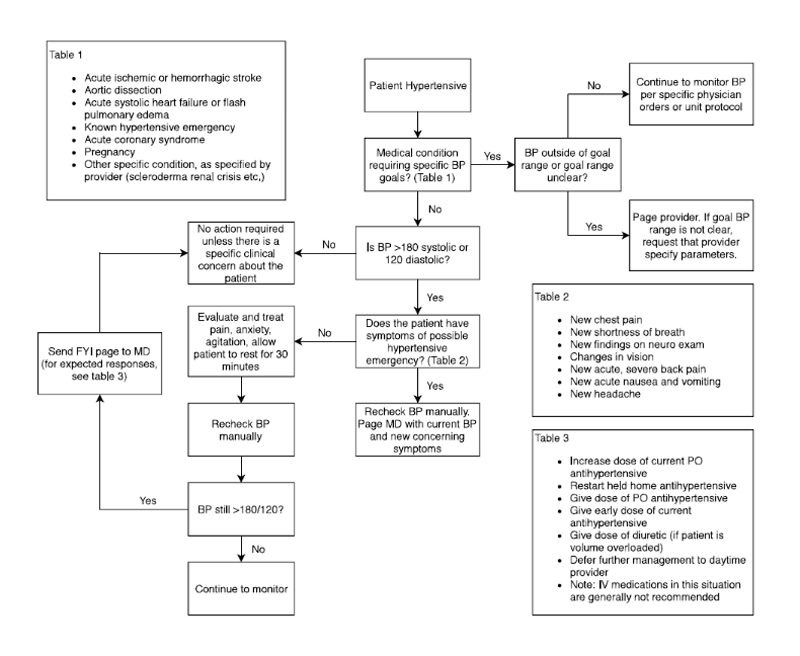
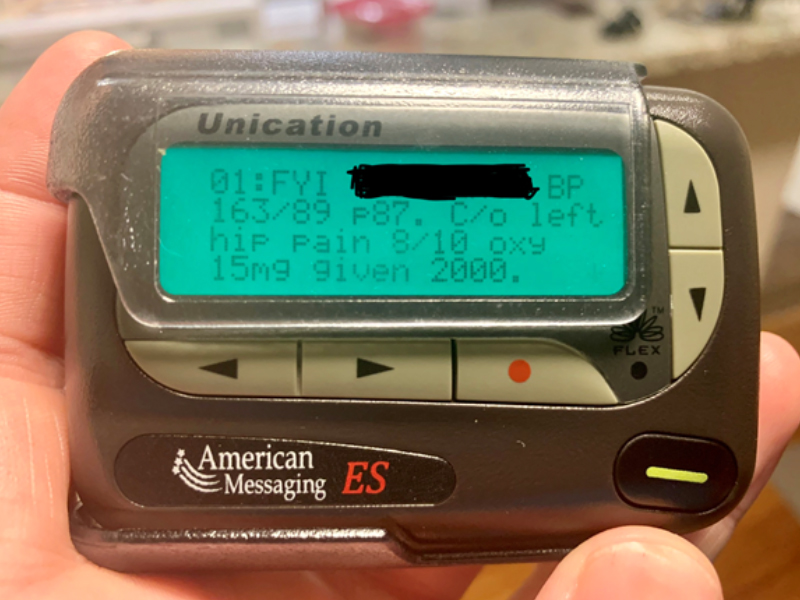
Blood pressure may be elevated in the hospital for many reasons (pain, anxiety, or the stress of getting woken up for a vital sign check). If the patient is asymptomatic, overnight we generally do not treat the number. Of course, new severe hypertension may have a treatable underlying cause, so seeing and evaluating the patient is a good idea. Certain new symptoms should be evaluated for a possible hypertensive emergency. Below is an algorithm I made for the nurses that represents the current standard of care.