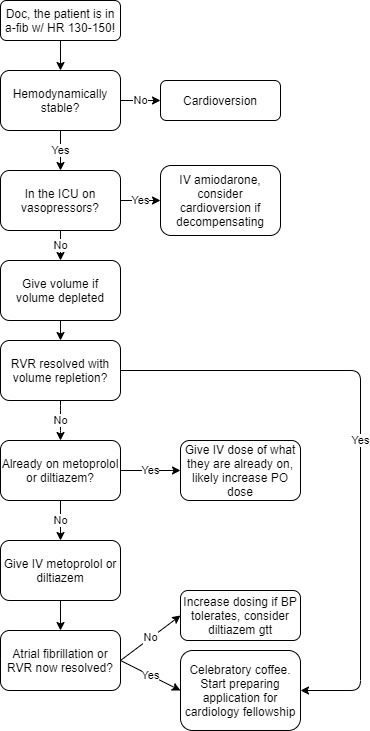
 Atrial fibrillation is a very common arrhythmia in the hospital. Fortunately, it is usually easy to manage. In general, I treat a-fib with RVR in the following way:
Atrial fibrillation is a very common arrhythmia in the hospital. Fortunately, it is usually easy to manage. In general, I treat a-fib with RVR in the following way:
Atrial fibrillation is a very common arrhythmia in the hospital. Fortunately, it is usually easy to manage. In general, I treat a-fib with RVR in the following way: