

From exposure to disease

Air pollutants enter the body through inhalation, triggering an inflammatory response cascade that affects multiple organ systems. Understanding these pathways— from molecular mechanisms to population health patterns—is essential for clinical practice.
Particle size determines where pollution goes in your body
- PM10 (≤10 μm): Deposits in upper airways (nose, throat, large bronchi); causes irritation and coughing.
- PM2.5 (≤2.5 μm): Penetrates to deep lung (small bronchi and alveoli); where gas exchange occurs.
- Ultrafine particles (<0.1 μm): Can cross alveolar-capillary barrier into bloodstream; systemic effects.
Key principle
Smaller particles = deeper penetration = greater health impact
Respiratory system impacts
Asthma: Acute exacerbations and chronic worsening
- Inflammatory Cascade:
- Oxidative stress: PM2.5 and ozone generate reactive oxygen species (ROS) in airway lining fluid.
- Cytokine release: ROS triggers release inflammatory mediators from epithelial cells and alveolar macrophages.
- Airway inflammation: Inflammatory mediators recruit neutrophils and eosinophils to airways.
- Result: Bronchial hyper-responsiveness increases.
- Bronchoconstriction:
- Direct irritant effects on airway smooth muscle.
- Inflammatory mediators trigger smooth muscle contraction.
- Parasympathetic nerve stimulation.
- Result: Acute narrowing of airways → Wheezing, shortness of breath.
- Mucus hypersecretion and impaired clearance:
- Goblet cell hyperplasia and metaplasia.
- Increased mucus production.
- Ciliary dysfunction impairs mucociliary clearance.
- Result: Mucus plugging → Cough, further airway obstruction.
- Direct epithelial cell damage:
- Ozone damages airway epithelial cells directly.
- PM2.5 disrupts epithelial barrier integrity.
- Increased permeability to allergens and irritants.
- Long-term: Airway remodeling with chronic exposure.
- Emergency department visits for asthma increase 20–35% on high pollution days.
- Symptoms develop within hours of exposure to elevated PM2.5 or ozone.
- Particularly pronounced during wildfire smoke events (PM2.5–dominant).
- Effects seen even at PM2.5 levels below current EPA standards.
Patients with asthma should be counseled to:
- Check AirNow.gov daily.
- Keep rescue inhalers accessible during high pollution.
- Limit outdoor activity when AQI >100 (orange or worse).
- Consider preemptive increase in controller medication during prolonged poor air quality.
Long-term exposure to traffic-related air pollution increases risk of asthma development in children:
- Children living <300m from major roads: 25% higher asthma incidence.
- Dose-response relationship: Closer proximity = Higher risk.
- Critical exposure window: Early childhood (birth to age 5).
Chronic obstructive pulmonary disease (COPD)
Air pollution accelerates the natural decline in lung function that characterizes COPD.
- Chronic inflammation: Persistent oxidative stress and cytokine production.
- Protease-antiprotease imbalance: Pollution shifts balance toward enzymes that break down lung tissue.
- Small airway remodeling: Fibrosis and narrowing.
Among patients with COPD exposed to chronic air pollution:
- FEV1 decline accelerated by 10–15 mL/year per 10 μg/m³ PM2.5.
- Exacerbation frequency increases 25–40% with chronic exposure.
- Hospital admissions for COPD spike during high pollution episodes.
- PM2.5 and ozone trigger acute COPD exacerbations.
- Lag time: Effects peak 0-5 days after exposure.
- Baseline airway inflammation amplifies response to pollution.
- Reduced respiratory reserve means smaller insults cause clinical symptoms.

Clinical implications
Joe is a 68-year-old patient with COPD who asks "Why should I check AQI?" What do you tell him?
Your chronically inflamed airways are primed to respond more severely to pollution. What causes minor irritation in healthy individuals triggers exacerbations requiring ED visits or hospitalization in COPD patients. Monitoring AQI and limiting exposure during poor air quality is as important as taking your medication.
Lung Cancer: PM2.5 as a Carcinogen
- Classification:
International Agency for Research on Cancer (IARC)- PM2.5 classified as Group 1 carcinogen; carcinogenic to humans (2013).
- Same category as:
- Tobacco smoke.
- Asbestos.
- Radon.
- Mechanisms of Carcinogenesis
- Genotoxic effects: Polycyclic aromatic hydrocarbons (PAHs) in PM cause DNA damage.
- Chronic inflammation: Inflammatory mediators promote tumor development.
- Epigenetic changes: Alteration of gene expression patterns.
- Impaired DNA repair: Oxidative stress overwhelms repair mechanisms.
- Dose-Response Evidence—large cohort studies demonstrate:
- Each 10 μg/m³ increase in long-term PM2.5 exposure = 10-15% increase in lung cancer risk.
- Risk persists even at low PM2.5 levels (below current EPA standards).
- Never-smokers also show increased risk with air pollution exposure.
- Adenocarcinoma subtype most strongly associated.
- Magnitude of Impact:
- Air pollution estimated to cause 15–20% of lung cancer cases in never-smokers.
- Population attributable fraction: 5–10% of all lung cancers in developed countries.
- Higher proportions in high-pollution regions.
Question 1: Respiratory pathophysiology
A 68-year-old patient with COPD asks why their physician recommended they check the Air Quality Index every day and limit outdoor activity when AQI is in the orange range or higher. Which of the following BEST explains the pathophysiological basis for this recommendation?
Patients with COPD have baseline chronic airway inflammation. When exposed to air pollution (PM2.5, ozone), the inflammatory cascade is amplified in already-inflamed airways through oxidative stress and cytokine release, significantly increasing the risk of COPD exacerbations. The recommendation to monitor AQI and limit outdoor activity during orange (101–150) or higher levels is based on this pathophysiological mechanism.
Why other options are incorrect:
- While ozone causes bronchoconstriction, it doesn’t affect everyone equally. COPD patients are particularly vulnerable due to baseline inflammation.
- Air pollution affects both cardiovascular and respiratory systems significantly.
- Air pollutants significantly affect adults with chronic lung disease, causing exacerbations and accelerated disease progression.
Cardiovascular system impacts
A 2024 state-of-the-art review in JACC: Advances states: "Air pollution is the most important environmental cardiovascular risk factor, with PM2.5 being the most studied air pollutant." Furthermore: "Clinicians should incorporate air quality considerations when assessing cardiovascular risk factors."
Sagheer U, Al-Kindi S, et al. JACC: Advances, 3(2):100805. 2024. doi: 10.1016/j.jacadv.2023.100805
Mechanisms of cardiovascular harm
Air pollution affects the cardiovascular system through multiple interconnected pathways (Sagheer et al., 2024).
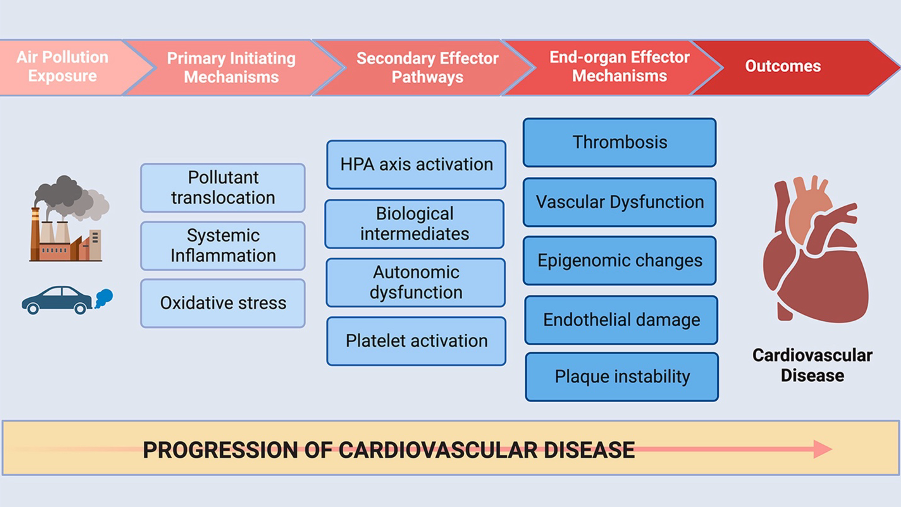
- Ultrafine particles (<0.1 μm) cross alveolar-capillary barrier.
- Enter systemic circulation within minutes to hours.
- Direct access to cardiovascular system.
- Pulmonary inflammation triggers systemic inflammatory response.
- Elevated circulating inflammatory markers:
- C-reactive protein (CRP).
- Interleukin-6 (IL-6).
- Fibrinogen.
- Inflammation persists hours to days after exposure.
- Reactive oxygen species damage vascular endothelium.
- Impaired nitric oxide (NO) production.
- Reduced vasodilation capacity and increased vasoconstriction.
- Measured as decreased flow-mediated dilation.
- Leads to endothelial damage and vascular dysfunction.
- Air pollution activates the hypothalamic-pituitary-adrenal (HPA) stress axis.
- Elevated cortisol and catecholamines increase cardiovascular strain.
- Contributes to hypertension and metabolic dysregulation.
- Decreased heart rate variability (HRV).
- Sympathetic activation.
- Arrhythmia susceptibility increases.
- Effects measurable within hours of exposure.
- Increased platelet activation and aggregation.
- Elevated coagulation factors and blood viscosity.
- Result: Higher thrombosis risk— leading to MI and stroke.
- Chronic exposure accelerates atherosclerosis.
- Plaque inflammation increases vulnerability to rupture.
- Documented by imaging (carotid intima-media thickness).
- Air pollution alters cardiovascular gene expression through epigenetic mechanisms.
- Changes in DNA methylation affect vascular and cardiac function.
- May explain long-term cardiovascular risk even after exposure ends.
Acute myocardial infarction (heart attack)
- Elevated risk within hours to days of high pollution exposure.
- Peak risk: 2–6 hours after exposure spike.
- Cumulative effect over several days.
- Both short-term spikes and chronic exposure increase risk.
Harvard Six Cities Study and subsequent meta-analyses:
- Consistent association between PM2.5 and cardiovascular events:
- Each 10 μg/m³ increase in PM2.5 → 1–3% increase in MI risk.
- Effects seen across multiple countries and populations.
Peters et al. (2004); NEJM: Exposure to Traffic and the Onset of Myocardial Infarction:
- Traffic exposure within 1 hour → 2.9x higher MI risk.
- Demonstrates acute triggering effect.
- Pre-existing cardiovascular disease.
- Diabetes (impaired endothelial function).
- Elderly (reduced physiological reserve).
- Recent MI survivors (vulnerable plaque).
When evaluating acute coronary syndrome, consider air quality as a potential trigger, especially in vulnerable patients. Document exposure in environmental history.
- Types Affected:
- Ischemic stroke: Most common, mediated by thrombosis and atherosclerosis mechanisms.
- Hemorrhagic stroke: Associated with acute blood pressure elevations from pollution exposure.
- Mechanisms:
- Pro-thrombotic state increases clot formation.
- Endothelial dysfunction in cerebral vessels.
- Blood pressure elevations (particularly with PM2.5 spikes).
- Cerebral atherosclerosis progression with chronic exposure.
- Evidence:
- Meta-analyses show consistent associations with both PM2.5 and ozone.
- Acute exposure (hours-days): Triggering effect.
- Chronic exposure (years): Risk factor for stroke development.
- Dose-response: Each 10 μg/m³ PM2.5 → 10–15% stroke risk increase.
- Heart failure
- Heart Failure Exacerbations:
- Hospital admissions spike 20–40% during high pollution episodes.
- AQI >100: Noticeable increase in heart failure hospitalizations.
- Patients with reduced ejection fraction particularly vulnerable.
- Mechanisms:
- Increased afterload.
- Inflammatory stress.
- Arrhythmias.
- Heart Failure Exacerbations:
- Hypertension
- Acute effects:
- Blood pressure elevations with both acute and chronic exposure.
- Systolic BP increases 1–5 mmHg per 10 μg/m³ PM2.5.
- Effects within hours, persist for days.
- Chronic effects:
- Long-term exposure associated with hypertension development.
- Population-level impact on cardiovascular disease burden.
- Contributes to health disparities (communities with high pollution exposure).
- Acute effects:
Three entry pathways: How air pollution reaches the brain
- Blood-brain barrier (BBB) crossing:
- Ultrafine particles can translocate across compromised BBB.
- Inflammation increases BBB permeability.
- Direct particle entry into brain tissue.
- Olfactory nerve pathway:
- Direct entry via nasal passages to olfactory bulb.
- Bypass blood-brain barrier entirely.
- Ultra-fine particles found in olfactory bulb in autopsy studies.
- Systemic inflammation effects:
- Peripheral inflammatory cytokines signal to brain.
- Neuroinflammation triggered without particle entry.
- Microglial activation in brain tissue.
Cognitive decline and dementia
- Neuroinflammation: Microglial activation and chronic inflammatory state in brain.
- Oxidative stress: ROS damage to neural tissue.
- Cerebrovascular effects: Small vessel disease, white matter changes.
- Protein aggregation: Potential role in amyloid and tau pathology.
- Accelerated cognitive aging with chronic PM2.5 exposure.
- Deficits in multiple domains:
- Memory (episodic and working memory).
- Executive function.
- Processing speed.
- Equivalent to ~2 years of aging per 10 μg/m³ PM2.5 increase.
- Effects seen in middle-aged and older adults.
- Reduced white matter volume.
- Hippocampal atrophy.
- White matter hyperintensities (small vessel disease).
- Cortical thinning in frontal and temporal regions.
Landmark Studies
- Carey et al. (2018) – BMJ Open:
- “Air Pollution and Dementia Incidence in London Cohort.”
- Large UK cohort (130,000+ adults).
- Higher PM2.5 and NO₂ → Increased dementia risk.
- Dose-response relationship demonstrated.
- Kioumourtzoglou et al. (2016) – Environmental Health Perspectives:
- “Long-term PM2.5 and Neurological Hospital Admissions.”
- Medicare population analysis.
- Each 10 μg/m³ PM2.5 → Increased dementia hospitalizations.
- 10–40% increased dementia risk with chronic PM2.5 exposure.
- Both Alzheimer’s disease and vascular dementia affected.
- Earlier onset in high-exposure populations.
- May contribute significantly to dementia burden in polluted regions.
- Traffic pollution exposure → Cognitive deficits in school-age children.
- Attention problems and ADHD associations.
- Autism spectrum disorder associations (emerging evidence).
- Critical windows: In utero and early childhood.
Concept map: Pathways from pollutants to disease
- PM2.5
- Ozone
- NO₂
- Oxidative stress.
- Cytokine release (IL-6, TNF-α).
- Endothelial dysfunction.
- Pro-thrombotic state.
- Autonomic dysfunction.
Multi-system outcomes: Respiratory
- Asthma.
- COPD.
- Lung cancer.
Multi-system outcomes: Cardiovascular
- Myocardial infarction.
- Stroke.
- Heart failure.
Major Cardiology Societies Joint Statement (2026)

A joint statement of the European Society of Cardiology, American College of Cardiology, American Heart Association, and World Heart Federation now formally recognizes environmental stressors—including air pollution—as significant contributors to the genesis and rising prevalence of cardiovascular disease.
Key statement findings:
- Environmental risk factors (ERFs) including air pollution have cumulative compound health impacts on cardiovascular disease.
- Urbanization has intensified ERF exposures, creating urgent opportunities for intervention.
- Impactful intervention requires regulatory and policy-driven efforts. targeting exposure sources.
- Vulnerable populations are disproportionately affected despite contributing least to the problem.
Integration of planetary and environmental health into cardiovascular care will be vital in reducing the burden of NCDs globally.
Münzel T, Lüscher T, Kramer CM, et al. (2026)
previous
Sources of Air Quality Degradation
Next
Vulnerable Populations