

Climate change and emerging infectious diseases
Pay attention to geographic considerations, diagnostic challenges, and the timeline of disease progression.
Clinical connection: Hunting for a Diagnosis
This short video (~9 min.) from the New England Journal of Medicine (NEJM) highlights the effects of climate change on health through an illustrative patient case.
Case Study: Fatal alpha-gal syndrome
{kind=link}
{kind=link}
{kind=link}
Download PDF of the above case
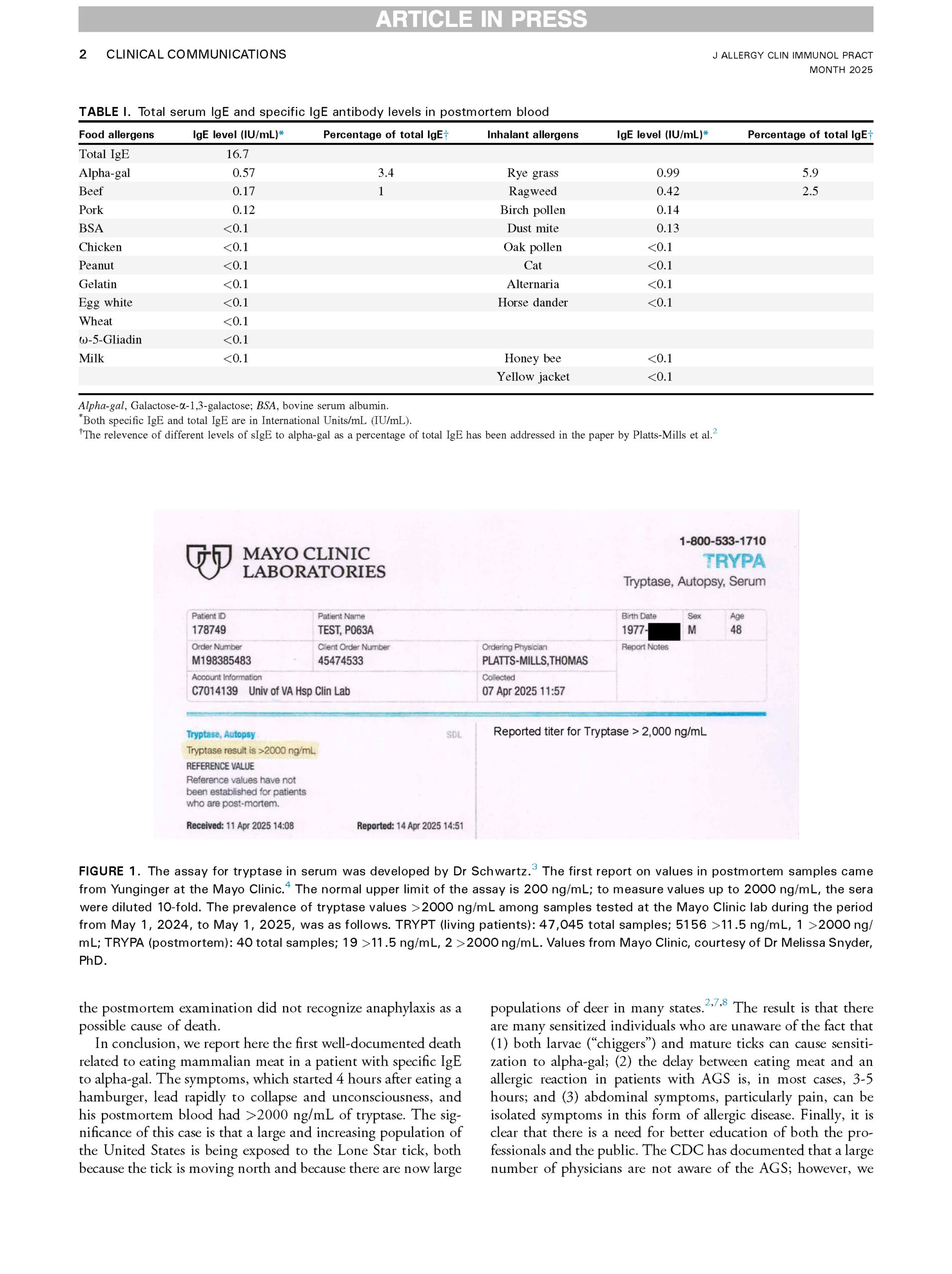
Implications of a fatal anaphylactic reaction occuring 4 hours after eating beef in a young man with IgE antibodies to galactose-⍺-1, 3-galactose
Case presentation

- Patient demographics
- Initial presentation
- Follow-up #1
- Infectious disease consult
- 2 months post exposure
- Second opinion
- Final diagnosis
- Treatment
- Outcome
Diana, a 46-year-old woman living in central Florida, describes herself as “outdoorsy.” She went hiking on the Wekiva Springs trails after several days of heavy rain. Due to the hot, humid weather, she wore shorts and did not use insect repellent. Upon returning home, she discovered 10 ticks on her body, of different shape and sizes: One on her neck and nine on her lower legs, with four ticks embedded on her right leg.
Note: The patient removed the embedded ticks using a blown-out match and tweezers—a method that is not recommended. Heat causes the tick to regurgitate into the wound, increasing infection risk.
Correct method: Use fine-tipped tweezers to grasp the tick as close to the skin’s surface as possible. Pull upward with steady, even pressure. Do not twist or jerk. After removal, clean the area with rubbing alcohol or soap and water. Never use heat, petroleum jelly, or nail polish.
Week 1
Swollen bite marks on right leg. One bite site shows an expanding circular red rash with central clearing, measuring approximately 3 inches in diameter. The rash is warm but not painful or itchy. Swollen and tender inguinal lymph nodes. Patient disposed of ticks but noted they varied in size—some were very small, others larger. She believed they included deer ticks (Ixodes scapularis).
Initial testing: CMP, CBC, TSH normal.
Lyme disease antibody test: Negative.
Physician’s assessment: These are just minor tick bites, not enough time to transmit infection.
Treatment: Doxycycline 200mg 1 for prophylaxis.
Week 3
Bull’s-eye rash still visible on right leg, now expanded to approximately 5 inches. Most bite sites improved. Lymph nodes no longer swollen.
New symptoms: Extreme afternoon fatigue (“fall asleep at your desk tired”), headaches, and diffuse joint aches.
Repeat testing: Lyme disease antibody test: Negative.
Physician’s assessment: “Lyme disease isn’t in central Florida, but I can send you to a specialist if you want.”
Action: Referred to infectious disease specialist.
Week 5
Low-grade fever (100.5°F average), extreme fatigue, decreased appetite. Bull’s-eye rash on right leg has faded, but site remains red.
New finding: Petechial rash (small red-purple spots) appeared on wrists and ankles, spreading to arms and legs—classic distribution for Rocky Mountain spotted fever.
Comprehensive testing
- Rocky Mountain spotted fever (RMSF): Positive.
- Lyme disease antibody test #3: Negative.
Treatment: Doxycycline 100mg twice daily for 10 days.
Week 9
Despite treatment for RMSF, Lyme-like symptoms persisted and worsened: Progressive fatigue, constant dull headache, ongoing joint aches, afternoon/evening fevers (99–101°F), and new right-sided Bell’s palsy (facial paralysis). RMSF rash has resolved, but original bite site on right leg remains red with some residual discoloration.
Testing: Lyme disease antibody test: Negative.
Family physician: “We can’t find anything wrong with you. Lyme disease isn’t in central Florida. Your symptoms should have resolved after treating the RMSF.”
Infectious disease specialist: “The RMSF has been successfully treated with doxycycline. These persistent symptoms don’t fit with resolved RMSF.”
Week 10
Patient sought a second opinion from a doctor at a center that researches and treats Lyme disease. The doctor’s first question: “Where did you hike?” When told Wekiva Springs, the specialist confirmed: “Lyme disease is most certainly in central Florida and is most prevalent in the Wekiva Springs trails area.”
Repeat testing results
- CBC: Platelets 140,000 (normal range 150,000–400,000 cells/microliter).
- CMP: AST 60, ALT 75 (normal range AST 10–40 Units/L, ALT 7–56 Units/L).
- Lyme disease Western blot (IgG): Positive (indicates established infection; IgG antibodies typically develop 4–6 weeks after exposure).
- Rocky Mountain Spotted Fever: Positive (co-infection).
- Anaplasmosis, Babesiosis, Ehrlichiosis: All negative.
- Cortisol: Elevated.
Dual infection with Lyme disease and Rocky Mountain spotted fever.
Doxycycline 100mg twice daily for 28 days (standard duration for neurologic Lyme disease with Bell’s palsy).
Complete resolution of all symptoms after 28 days of treatment. Six months later, patient remains symptom-free. A small, red mark persists on her right leg.
Lyme disease

- Climate change is expanding tick habitats beyond traditional endemic areas. This case demonstrates that Lyme disease is no longer confined to the northeast United States.
- Physicians must update their assumptions about disease geography. The statement “Lyme disease isn’t in central Florida” represents outdated thinking that delayed diagnosis in this case.
- Warmer temperatures and changing precipitation patterns are allowing ticks to survive in previously inhospitable regions.
- Lyme disease testing has a “serologic window”—initial antibody screening tests (ELISA) may be negative in the first 3–4 weeks. This patient had four negative screening tests over 9 weeks. The Western blot, a more specific confirmatory test, finally detected IgG antibodies indicating established infection. Note: For Lyme disease, IgM testing is only interpreted within 30 days of symptom onset due to false positive risk; after that, only IgG results are clinically meaningful.
- Clinical diagnosis should take precedence when classic signs (bull’s-eye rash, appropriate exposure, compatible symptoms) are present, even with negative laboratory tests.
- The lifecycle of Borrelia burgdorferi (Lyme spirochete) involves morphological changes that can affect test accuracy.
- This case demonstrates distinct rash patterns: Lyme disease presented with expanding erythema migrans (bullseye, warm, non-itchy, 3–5 inches) appearing early. RMSF presented with petechial rash (small red-purple spots starting on wrists/ankles, spreading centrally) appearing at week 5. Recognizing these distinct patterns is crucial.
- The patient had 10 ticks of varying shapes and sizes, suggesting the possibility of multiple tick species. Lyme disease is transmitted by Ixodes scapularis (deer tick/black-legged tick), while RMSF in the Southeast is typically transmitted by Dermacentor variabilis (American dog tick) or Amblyomma americanum (lone star tick). Co-infection from exposure to multiple tick species is biologically plausible.
- Co-infections can complicate diagnosis and treatment, as symptoms may overlap or mask each other.
Note: Doxycycline treats both RMSF and Lyme disease. RMSF requires 7–10 days of treatment. However, neurologic Lyme disease with manifestations like Bell’s palsy requires 14–28 days of treatment. The 10-day course successfully treated RMSF but was insufficient for the established neurologic Lyme infection, which required the full 28-day course.
- Proper tick removal: Use fine-tipped tweezers to grasp the tick as close to the skin as possible and pull upward with steady pressure. Never use a match, petroleum jelly, or other folk remedies.
- Prevention strategies: Wear long pants tucked into socks; use DEET-based repellent; perform thorough tick checks after outdoor activities, especially in wooded or grassy areas.
- Save the tick (if possible) for identification—knowing the tick species can help guide diagnosis and treatment decisions.
- Dismissive statements like “We can’t find anything wrong with you” can cause significant patient distress and erode trust, especially when symptoms are debilitating.
- When test results conflict with clinical presentation: Acknowledge the patient’s experience and continue investigation rather than dismissing their concerns.
- This case demonstrates the importance of medical humility—being willing to question established assumptions (like disease geography) when faced with compelling clinical evidence.
Think about this and discuss
- How is climate change specifically affecting the geographic distribution of vector-borne diseases? What mechanisms (temperature, precipitation, ecosystem changes) are driving this expansion?
- What should physicians do when clinical presentation strongly suggests a diagnosis, but laboratory tests are negative? How do we balance evidence-based medicine with clinical judgment?
- Why did it take two months to diagnose this patient despite multiple physician visits and classic symptoms? What systemic factors contributed to the diagnostic delay?
- What other vector-borne diseases are likely to expand their range due to climate change? Consider both domestic and tropical diseases that might move northward.
- How should medical education adapt to prepare future physicians for the changing epidemiology of infectious diseases? What specific knowledge gaps need to be addressed?
Additional exploration
Image credits
Unless otherwise noted, images are from Adobe Stock.