



Sepsis and septic shock represent a severe manifestation of infection associated with significant morbidity and mortality in children. They remain prevalent in the pediatric population both in resource-limited and resource-abundant regions. The definitions for sepsis and septic shock in children were updated in 2024 by the International Society of Critical Care Medicine Pediatric Sepsis Definition Task Force in order to provide better specificity and a useful means of predicting survival to hospital discharge. These employ a “Phoenix Sepsis Score”.
-
definitions
- Sepsis may be defined as suspected infection and a Phoenix Sepsis Score of 2+ (see Table below).
- Septic shock may be defined as sepsis plus 1 or more cardiovascular points in the Phoenix sepsis score:
- Hypotension (using the mean arterial pressure for age).
- Blood lactate > 5 mmol/L.
- Need for vasoactive medication.
- “Evolving sepsis” in children may be defined as suspected infection and clinical findings of altered perfusion that are not severe enough to meet the 2024 International Consensus Criteria for sepsis or septic shock.
Phoenix Sepsis Score
| Variables | 0 points | 1 point | 2 points | 3 points |
|---|---|---|---|---|
|
Respiratory, 0 to 3 points |
|
|
|
|
|
Cardiovascular, 0–6 points |
|
|
|
Intentionally left blank |
|
Coagulation (1–2 points) |
|
|
Intentionally left blank |
Intentionally left blank |
|
Neurological (0 to 2 points) |
|
Glasgow Coma Scale score ≤10 |
Fixed pupils bilaterally |
Intentionally left blank |
Age based
| Age | 0 points | 1 point | 2 points | 3 points |
|---|---|---|---|---|
|
< 1month |
>30 mmHg |
17–30mmHg |
<17mmHg |
Intentionally left blank |
|
1 to 11 months |
>38mmHg |
25–38mmHg |
<25mmHg |
Intentionally left blank |
|
1 to <2 years |
>43mmHg |
31–43mmHg |
<31mmHg |
Intentionally left blank |
|
2 to <5 years |
>44mmHg |
32–44mmHg |
<32mmHg |
Intentionally left blank |
|
5 to <12 years |
>48mmHg |
36–48mmHg |
<36mmHg |
Intentionally left blank |
|
12 to 17 years |
<51mmHg |
38–51mmHg |
<38mmHg |
Intentionally left blank |
criteria
- Sepsis = Suspected infection and Phoenix Sepsis Score ≥ 2 points.
- Septic shock = Sepsis with ≥ 1 cardiovascular point(s).
Epidemiology
Pediatric sepsis has a high burden, impacting an estimated 28 million children worldwide, with estimated in-hospital mortality of 33% in resource-limited settings, and just over 10% in resource-abundant settings. Many pathogens causing sepsis are vaccine-preventable (see Etiology).
- Age younger than one month.
- Serious injury (e.g., major trauma, burns, or penetrating wounds).
- Chronic debilitating medical condition (e.g., static encephalopathy with quadriplegia and frequent aspiration pneumonia, uncorrected congenital heart disease, short bowel syndrome).
- Host immunosuppression:
- Malignancy.
- Human immunodeficiency virus infection.
- Severe malnutrition.
- Congenital immunodeficiency.
- Sickle cell disease and other diseases with splenic dysfunction.
- Immunosuppressive medications.
- Large surgical incisions
- In-dwelling vascular catheters or other invasive devices (e.g., endotracheal tube, Foley catheter, chest tube).
- Urinary tract abnormalities with frequent infection.
Etiology
Bacterial and viral pathogens are most common, but fungal, parasitic, and rickettsial infections are all possibly pathogenic.
- Staphylococcus aureus including methicillin-resistant strains (MRSA).
- Coagulase-negative Staphylococcus especially in neonates or young infants with in-dwelling vascular catheters.
- Streptococcus pneumoniae.
- Streptococcus pyogenes.
- Neisseria meningitidis (especially in sub-Saharan Africa).
- Group B streptococcus in the neonate.
- Pseudomonas aeruginosa including carbapenem-resistant strains.
- Escherichia coli, including those with extended spectrum beta-lactamase activity (ESBL).
- Enterococcus species, including vancomycin-resistant species.
- Klebsiella species, including those with ESBL activity.
- Alpha streptococcus in children with acute myelogenous leukemia with mucositis and neutropenia.
- Alpha streptococcus in children with acute myelogenous leukemia with mucositis and neutropenia.
- Haemophilus influenzae type b in unimmunized children.
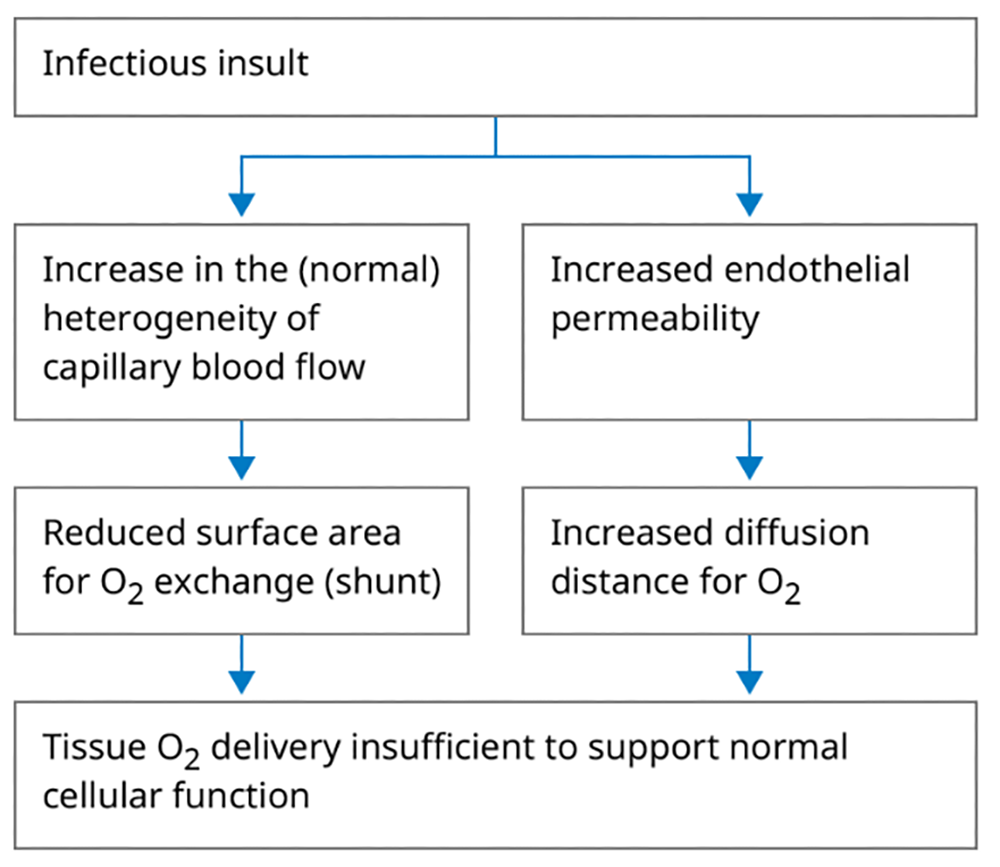
Pathophysiology
Sepsis and septic shock result from a complex interplay of microbial factors, host immune response, and endothelial dysfunction. Microbial products (endotoxins, exotoxins) attach to pattern recognition receptors, e.g., toll-like receptors, on the surface of host immune cells, triggering cytokine cascades, especially TNF-alpha and IL-1, complement activation, and coagulation pathways (DIC).
Septic shock, as the practical definition above implies, occurs when these factors result in hemodynamic changes, which reduce perfusion to vascular beds.
Cellular injury may occur through multiple mechanisms: As a result of cytopathic injury caused by proinflammatory mediators and resulting mitochondrial dysfunction; tissue ischemia; and apoptosis.
Widespread cellular injury is common in sepsis and septic shock, and often adversely impacts organ function across multiple organ systems causing one or more of:
- Vascular insufficiency characterized by vasodilation, shunting, and increased capillary permeability.
- Pulmonary edema and insufficiency, ARDS.
- Enteric dysfunction, with increased gut permeability to bacteria.
- Liver dysfunction, which further reduces the liver’s ability to handle enteric-derived endotoxins and other bacterial toxins.
- Acute kidney injury, kidney failure caused by acute tubular necrosis.
- Encephalopathy, characterized by altered mental status.
Clinical features
Early recognition of sepsis and septic shock is critical. Children may present with fever, tachycardia, tachypnea, hypotension, widened pulse pressure, altered mental status (e.g. irritability, somnolence, or lethargy), poor peripheral perfusion (as evidenced by cool extremities, mottling of the skin, and prolonged capillary refill time), and signs of organ dysfunction (e.g., respiratory distress, oliguria). However, the clinical presentation varies significantly with age, underlying health status, and the causative pathogen. In particular, infants and especially premature newborns may present with hypothermia, bradycardia, hypopnea, and apnea due to immaturity in brain stem responses and central temperature regulation.
Specific features to look for on examination include:
- Toxic appearance (for example, glassy-eyed stare; sometimes a parent may verbalize that the child just doesn’t look right, or she’s not herself).
- Poor color.
- Altered mental status.
- Abnormal vital signs.
- Altered peripheral perfusion.
- Bounding pulses.
- Pulmonary rales.
- Distended and/or tender abdomen.
- Meningismus.
- Seizures.
- Hypotonia.
- Skin eruptions occurring in specific infections such as cellulitis or the purpuric rash of meningococcemia.
- Point-of-care glucose (hypoglycemia may occur, especially in newborns).
- Complete blood count (often shows leukocytosis, but sometimes may show paradoxical leukopenia; also look for evidence of disseminated intravascular coagulation, or DIC, including anemia with fragmented RBCs and thrombocytopenia).
- Blood gas (may be obtained from a sample of venous, arterial, or “capillary”—from a heelstick specimen, for example—blood; may show significant metabolic acidosis, and respiratory compensation in an arterial or capillary sample).
- Blood chemistries, including:
- Electrolytes (also including iCa, Mg, Phos).
- BUN.
- Creatinine.
- Liver transaminases.
- Total bilirubin.
- Lactate (these studies provide information on electrolyte imbalances associated with sepsis, as well as evidence of poor perfusion and end-organ damage).
- Coagulation studies, including:
- PT.
- PTT.
- INR.
- Fibrinogen.
- D-dimer (which investigate for specific evidence of consumptive coagulopathy and DIC).
- Inflammatory biomarkers, including:
- Procalcitonin.
- C-reactive protein (while neither diagnostic for sepsis nor specific to any type of infection, these studies may add weight to evidence for serious bacterial infection and may be useful for following the course of the infection once treatment has been initiated).
- Urinalysis (mostly to look for UTI and urosepsis, but also useful to screen for findings of acute tubular necrosis including proteinuria, hematuria, and muddy brown granular casts).
- Cultures—blood, and possibly urine, CSF, sputum, wound (with gram stains when possible, to identify pathogen and extent of spread).
- Additional studies may include:
- CSF fluid analysis.,
- Viral studies.
- Fungal cultures.
- Serological investigations when the pathogen is not readily identifiable.
- Commonly includes chest X-ray, which is an excellent means of diagnosing pneumonia and screening for radiographic changes of ARDS.
- Other imaging studies including ultrasound, CT, and other imaging modalities may be indicated to investigate sources of infection in the abdomen, CNS, joints, and other body regions.
Diagnosis
The diagnosis of sepsis and septic shock begins with clinical index of suspicion based on history and physical exam findings. Diagnostic testing described above helps to delineate the extent of the disease, end-organ involvement, and to identify the pathogen. The Phoenix Sepsis Score delineated above provides a more robust diagnostic tool for confirmation of the diagnosis and prediction of survival to hospital discharge.
Treatment
Immediate management focuses on four key elements:
Aggressive fluid resuscitation with crystalloid (e.g. normal saline) to replenish a depleted vascular compartment.
Vasoactive medications such as epinephrine or norepinephrine are often necessary when perfusion remains poor following administration of 40–60mL/kg of crystalloid to reduce the severe vasodilatation which often accompanies sepsis and septic shock.
Antibiotic therapy should be initiated promptly, based on suspected pathogens and local resistance patterns, initially with a broad spectrum of coverage (see empiric antibiotic coverage), then refined to narrow the spectrum of coverage to identified pathogens.
Supportive care with close monitoring of vital signs, perfusion, urine output, and oxygen saturation, often including:
- Antipyretic therapy.
- Oxygen.
- Mechanical ventilation.
- Nutritional support following initial fluid resuscitation.
- Sometimes transfusion of blood products.
- Renal replacement therapy.
- Adjunctive therapies (e.g., corticosteroids, intravenous immunoglobulin) in selected cases.
-
principles of empiric antibiotic coverage
- Initial coverage should be administered rapidly and should be broad-spectrum.
- Pathogens vary significantly by age.
- Antibiotic sensitivities vary from institution to institution.
- Meropenem is a suitable commonly used alternative to penicillins for patients with serious allergy to penicillin, e.g., anaphylaxis.
- Vancomycin should be included when there is a high prevalence of MRSA in the community or known MRSA in the patient or immediate family.
- Coverage for Pseudomonas spp should be included in immunocompromised patients and patients with cystic fibrosis.
- Coverage of enteric coliforms and anaerobes should be included with a suspected GI source.
- Acyclovir should be included for a newborn (up to 28 days old) with suspected HSV infection.
- For infants >28 days of age and older children, either ceftriaxone or cefotaxime are suitable agents for broad-spectrum empiric coverage.
- The table delineates commonly used antibiotic regimens for newborn infants.
| Empiric therapy | Antibiotic regimen |
| Early onset (<72 hours) | Ampicillin and an aminoglycoside (typically gentamicin) |
| Late onset (≥72 hours): Admitted from the community |
|
| Late onset (≥72 hours): Hospitalized since birth |
Vancomycin or nafcillin/oxacillin, and an aminoclycoside (typically gentamicin) |
Special circumstances
| Empiric therapy | Antibiotic regimen |
| Suspected meningitis (e.g., CSF pleocytosis) | Same as above expect substitute an expanded-spectrum cephalosporin [e.g., ceftazidime, cefepime, or cefotaxime (where available)] for the aminoglycoside |
| Suspected pneumonia |
|
| Suspected infection of skin, umbilicus, soft tissue, joints, or bones (S. aureus is a likely pathogen) |
|
| Suspected intravascular catheter-related infection | Vancomycin and an aminoglycoside (typically gentamicin) |
| Suspected infection due to organisms found in the gastrointestinal tract (e.g., anaerobic bacteria) |
|
Potential complications
Sepsis and septic shock can lead to profound complications despite optimal therapy. These include:
- Acute respiratory distress syndrome (ARDS).
- Acute kidney injury (AKI).
- Hepatic dysfunction.
- Myocardial dysfunction (septic cardiomyopathy).
- Neurologic sequelae.
Long-term outcomes may include physical, cognitive, or developmental impairments, emphasizing the need for comprehensive follow-up care.
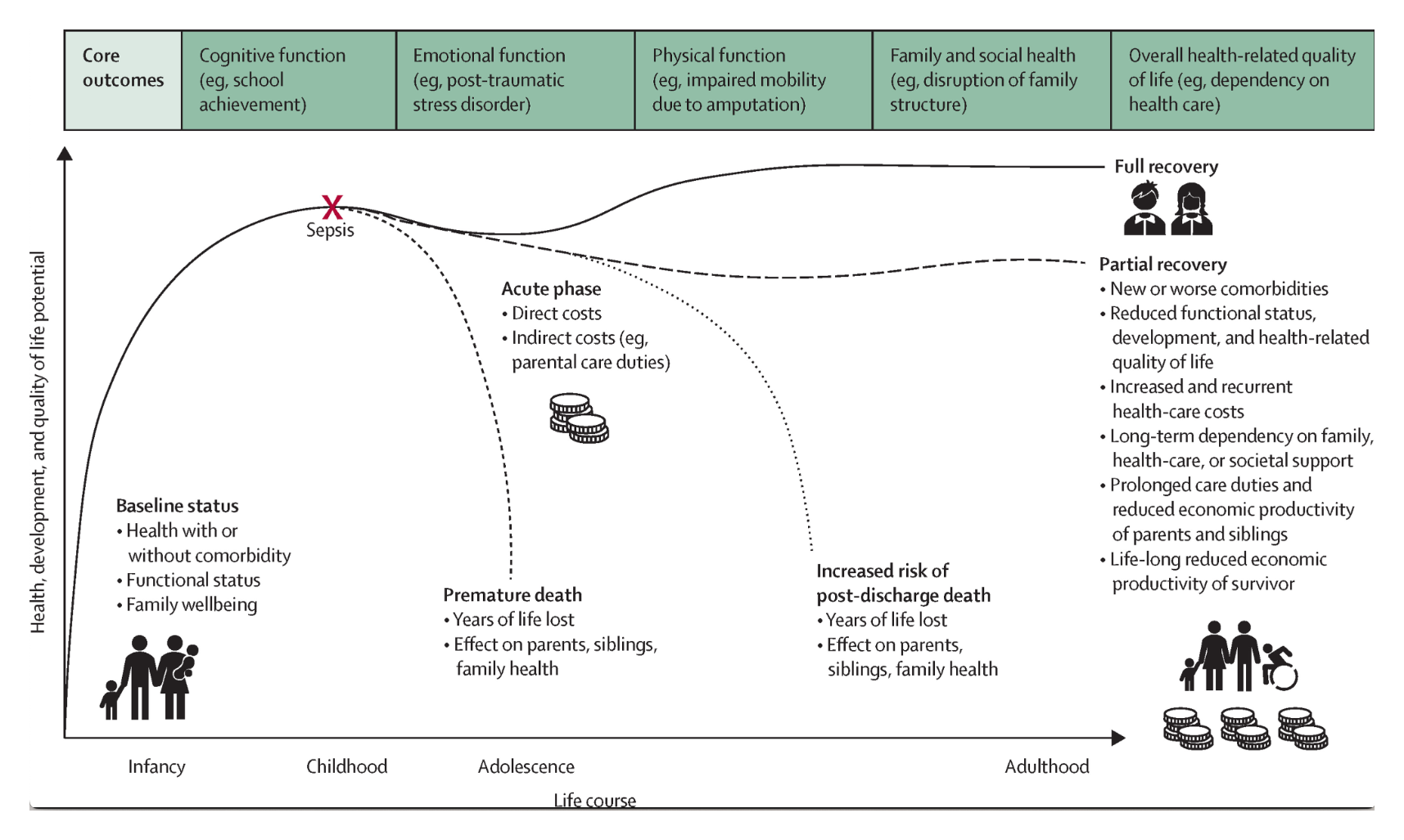
Source: The burden and contemporary epidemiology of sepsis in children. The Lancet Child & Adolescent Health.
Conclusion
Students and residents engaged in the care of the child must remain vigilant in recognizing the signs of sepsis and septic shock in children, as early recognition and treatment is associated with improved outcomes. Early recognition, prompt fluid resuscitation, initially broad-spectrum antibiotic therapy, followed by therapy specifically targeted to treat the identified pathogen(s), vigilant monitoring, and supportive care are pivotal in optimizing outcomes.
Image credits
Unless otherwise noted, images are from Adobe Stock.