



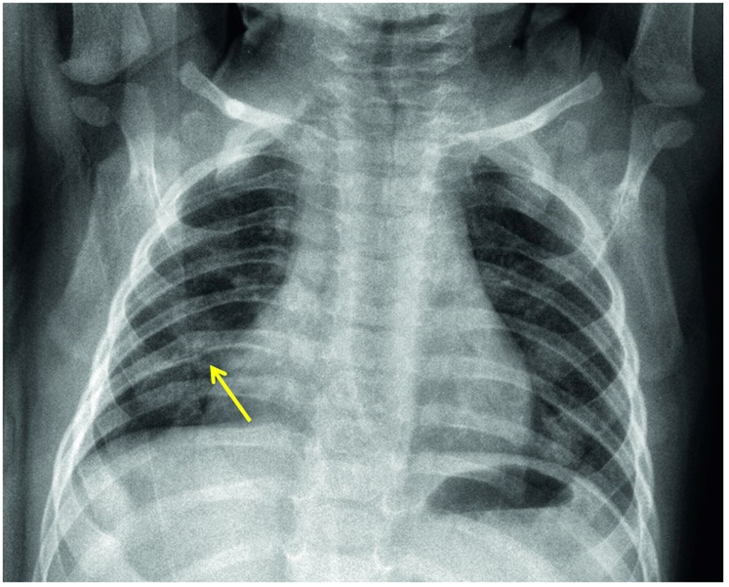
 The diagnosis of bronchiolitis is clinical (based on the patient’s history and physical examination). Laboratory testing and radiographic studies are not recommended for diagnosis. CBC, inflammatory markers, blood culture, and chest x-ray should only be used when a serious bacterial infection (SBI) is suspected. A viral respiratory panel may be used to aid in the more accurate diagnosis of the viral pathogen, which may be useful for the hospitalized patient or in patients not following the expected course of illness. A chest x-ray may be performed to rule out conditions like effusions or pneumothorax when there is clinical suspicion but should not be used to evaluate for pneumonia as that is a clinical diagnosis. In bronchiolitis, the chest x-ray may show hyperinflation of the lungs, atelectasis, or peribronchial cuffing that is often referred to as the classic cheerio (see CXR).
The diagnosis of bronchiolitis is clinical (based on the patient’s history and physical examination). Laboratory testing and radiographic studies are not recommended for diagnosis. CBC, inflammatory markers, blood culture, and chest x-ray should only be used when a serious bacterial infection (SBI) is suspected. A viral respiratory panel may be used to aid in the more accurate diagnosis of the viral pathogen, which may be useful for the hospitalized patient or in patients not following the expected course of illness. A chest x-ray may be performed to rule out conditions like effusions or pneumothorax when there is clinical suspicion but should not be used to evaluate for pneumonia as that is a clinical diagnosis. In bronchiolitis, the chest x-ray may show hyperinflation of the lungs, atelectasis, or peribronchial cuffing that is often referred to as the classic cheerio (see CXR).
There are multiple ways to score severity of respiratory distress in the setting of bronchiolitis, which in turns aids in informing how aggressive clinical management should be and whether hospitalization should be considered. Most large Children’s Hospitals have internal scoring systems; however, they often include the following consistent variables: Respiratory rate based on age, work of breathing, mental status, oxygen requirement, and breath sounds.
One such scoring system is the Respiratory Severity Score (RSS):
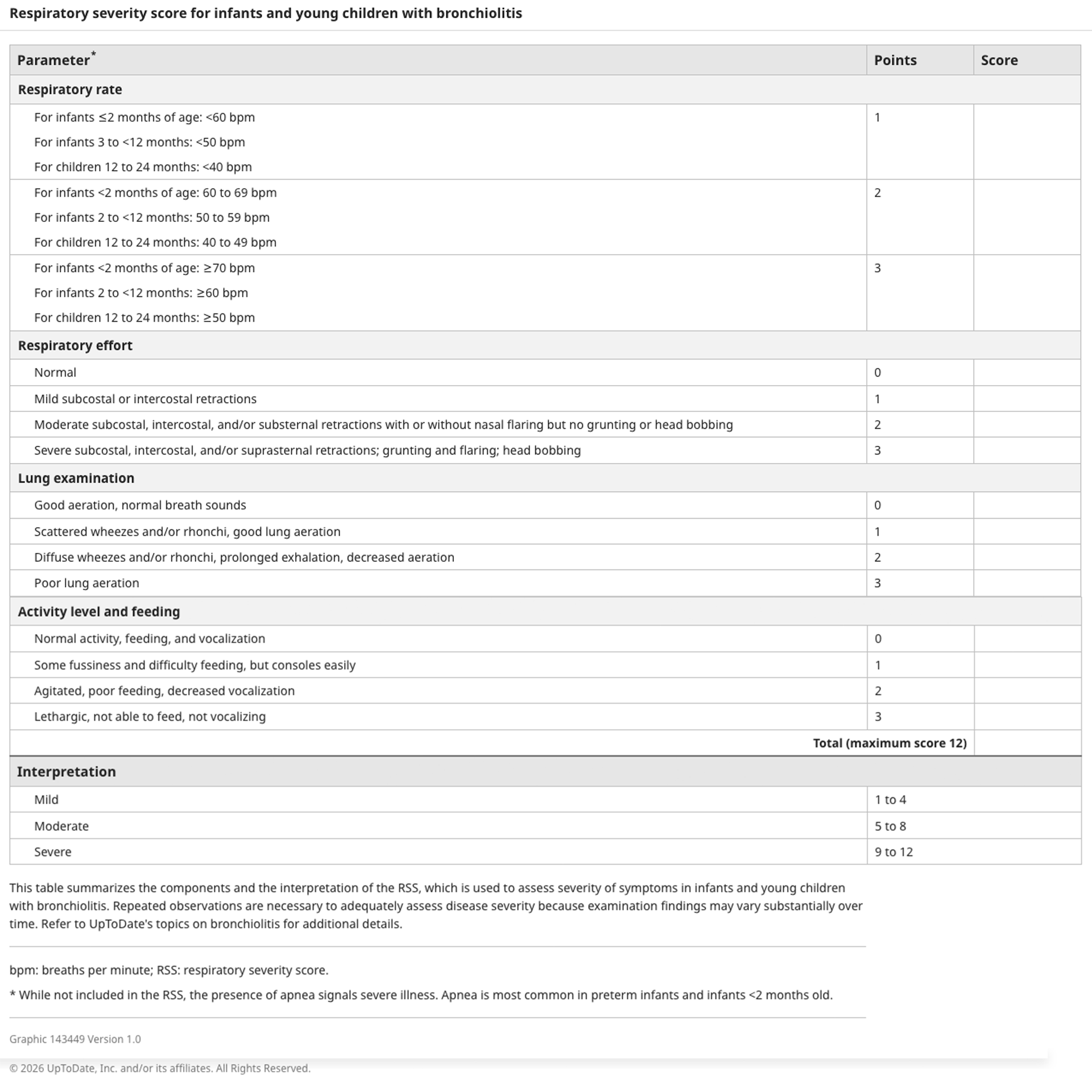
While these scoring tools aid in management decisions at initial presentation, decision to admit should also take into account whether the patient is able to hydrate well on their own and where they are in their illness course (as we know most viral infections will worsen until their 3–5 day peak and then start to self-resolve). If the family lives very far from their nearest healthcare facility, or cannot get close follow up with their pediatrician, the provider may also make the decision to admit the child for close monitoring.