



What is pain? In a general sense, pain can be thought of as, “An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage” (International Association for the Study of Pain 1979). But a more important definition for providers to keep in mind is that pain is a subjective experience that is often poorly understood by anyone who is not the individual experiencing it; in pediatrics this is especially important as the patient and caregiver can have different perspectives and it is important for the provider to reconcile the two.
goals of pain management
It is important to establish clear, and realistic, pain goals between the care team and family. There should be education for both the care team and family on the steps to achieving those goals and discuss both pharmacologic and non-pharmacologic interventions. Some specific goals include minimizing the intensity and duration of pain, using a developmentally appropriate pain scale to assess pain and monitor medication efficacy, and initiating therapy with a contingency plan in place so there is no delay in care if initial therapy is not sufficient. The relationship between pain and anxiety is important to note, and thus the providers should work on maximizing coping and recovery by breaking the anxiety-pain cycle. Finally, it is important to have a pain plan for home prior to discharging a patient from the Emergency Room or Inpatient setting, with a focus not only on medications but also on appropriate dosing for the patient’s current weight.
-
pediatric versus adult pain
The younger children are, the less likely they are to receive appropriate pain control. Compared to adults, pediatric patients receive fewer and/or incorrectly dosed analgesics. Inadequate analgesia for initial procedures in children diminishes the effect of adequate analgesia in subsequent procedures. Children with persistent pain are more likely to suffer from anxiety and depression as adults and are more likely to have concurrent physical manifestations of their psychiatric illnesses. In children with physical injury or burns that result in hospital treatment, morphine use has been associated with lower levels of medical PTSD.
Types of pain
- Somatic pain is well localized, sharp, intense. This includes pain from soft tissue (e.g., late appendicitis), skin (e.g., laceration), bone (e.g., osteomyelitis), procedural pain.
- Visceral pain is vague, not well localized, achy/dull/cramping/deep. Organ-related pain (e.g., gastroenteritis, pancreatitis, early appendicitis).
- Referred pain is when visceral pain in one area is interpreted as somatic pain in another due to input at the same spinal cord level.
- Neuropathic pain is caused by the dysfunction of the somatosensory system that begins in the nerve itself. Damaged nerves result in pain in corresponding dermatomes. Examples include central (e.g., associated with limb salvage) vs. peripheral (e.g., chemotherapy-induced, ischemia in sickle cell disease (SCD), nerve root compression).
- Psychosocial-spiritual-emotional pain often co-exists with other types of pain but can be the main/only type present (especially in children).
Acuity
Specific event, usually limited to a short period. Examples include sutures and needle pain.
Extends beyond the initial event; however, has a predictable course of healing. An example would be post-operative pain.
Persistence beyond normal tissue healing time (>3 months). This type of pain is often neuropathic but can also be secondary to scar tissue or continued inflammation such as in arthritis.
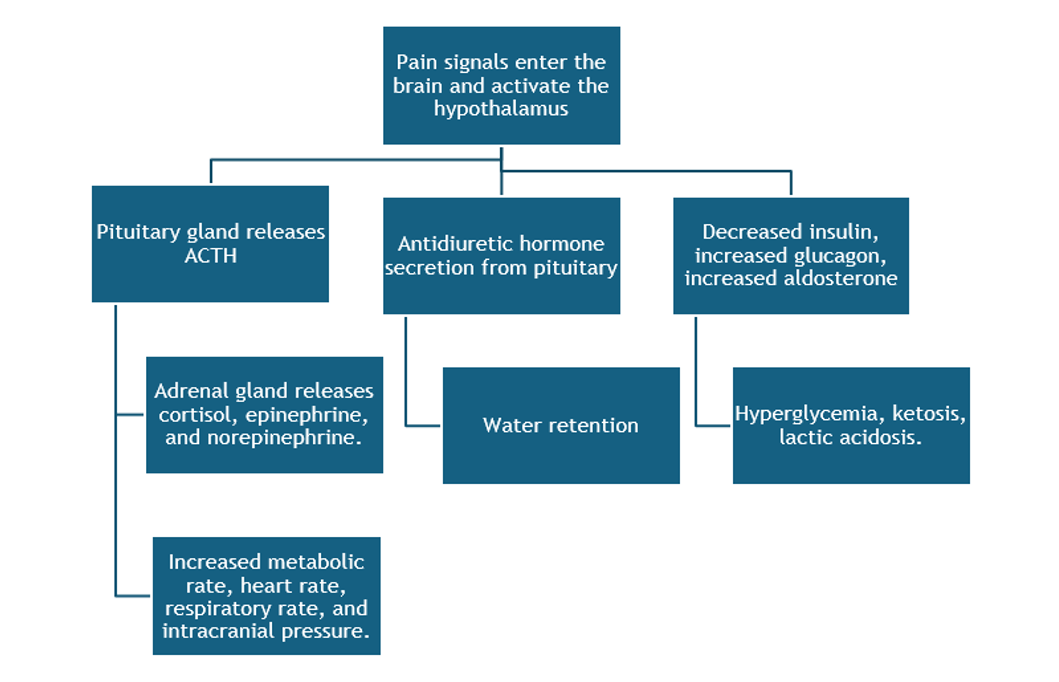
Physiologic effects of pain
Pain is not just a subjective feeling; it can lead to physiological changes in the body both acutely and long term. In the acute setting, pain can decrease pulmonary blood flow and decrease lung volumes which leads to retained secretions and atelectasis. Increased systemic and peripheral vascular resistance can lead to hypertension. Increased coronary vascular resistance can lead to increased myocardial oxygen consumption and myocardial damage. Subacute and chronic pain can impair immune function, delay gastric emptying and decrease gut motility, and cause fatigue and muscle tetany.
barriers to pain control
There are some common misconceptions about pediatric pain. Caregivers and providers may think that because a child is not/cannot vocalize their pain that they are not feeling pain. There is the erroneous thought that children and infants are less sensitive to pain. It is also incorrect to assume that all children have the same response to certain pain medications.
On a larger scale, there is a lack of understanding of the stress/trauma caused by untreated pain. Hospital staff may not have education regarding developmentally appropriate assessment tools, and non-pediatric providers may be unfamiliar or uncomfortable with different methods of pain treatment which then leads to fears of adverse events or addiction when considering stronger pain medication. From the patient’s perspective, they may not appropriately report their pain due to fear of medications, thinking they need to “be brave,” or thinking that asking for medications will keep them in the hospital longer.
Pain assessment tools
The most reliable indicator of the existence and intensity of acute pain is the patient’s own report, however this puts pediatric providers in an especially difficult position as our patients often cannot articulate well. There are three main goals of pain assessment:
1
Identify characteristics of pain.
2
Establish baseline assessment.
3
Evaluate pain status post-intervention.
Mnemonic
In taking a history, a helpful mnemonic when asking about a patient’s pain is the PQRSTU.
- P
- Q
- R
- S
- T
- U
Provocative/palliative
Quality
Region/radiation
Severity: Developmentally appropriate pain scales.
Timing: Constant vs. intermittent.
How it affects yoU: ADLs etc.
FLACC scale
The most commonly used tool in the inpatient setting is the FLACC scale. This can be used in infants and up through 3 years of age and should be used in non-verbal children. As a note for infants, low ATP reserve means repeated insults to baby may result in decrease in the infant’s ability to react to pain due to lack of energy, but this does not alter their perception of pain.
Pre-verbal and non-verbal 1 month–7 years FLACC scale
| Categories | Scoring: 1 | Scoring: 2 | Scoring: 3 |
|---|---|---|---|
|
Face |
No particular expression or smile
|
|
|
|
Legs |
Normal position or relaxed |
|
|
|
Activity |
|
|
|
|
Cry |
No cry (awake or asleep) |
|
|
|
Consolability |
|
|
Difficult to console or comfort |
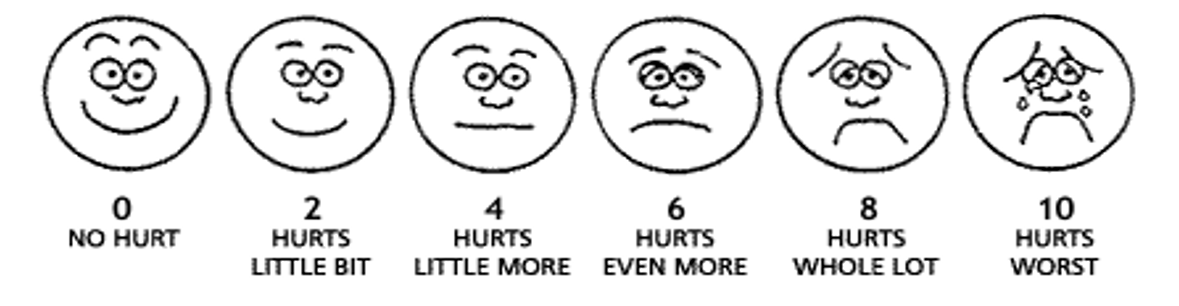
For verbal children over age 3, we use the scale of 1–10 either with faces (3–8 years old) or numbers (>8 years old). It is still important to assess non-verbal clues, including heart rate, facial expressions, and activity (crying, tremors, hypertonicity, fussiness).
Needle pain
This section will help you identify key modalities to prevent needle pain caused by elective procedures such as lab draws, IV placement, vaccines, and lumbar punctures. Untreated needle pain can have long term consequences including, future pre-procedural anxiety, chronic hyperalgesia, needle fear into adulthood, and avoidance of healthcare (including non-adherence with vaccination schedules). Unfortunately, there are multiple healthcare myths that prevent needle pain from being appreciated, such as that needle sticks don’t hurt that much, the pain from needle sticks is unavoidable and fleeting, and the investment of money and time is not worth the benefit in trying to avoid something that is often over so quickly. There are multiple ways to mitigate needle pain, but here we will focus on four high yield methods.
This is often utilized for IV placements and lumbar punctures but can also be utilized for vaccines or intramuscular medications. Lidocaine (4%) is available over the counter and can be used by families in anticipation for vaccines or lab draws. Use of numbing agents such as EMLA cream or Synera patches for IV starts has been shown to increase the success of IV placements on first attempts.
A sugar nipple coated with either sucrose or glucose has a role in increasing endogenous opioids and is best utilized when administered within 1-2 min of a mild procedure and then frequently as needed during the procedure. Breastfeeding has been shown to be more beneficial than a sugar nipple, likely due to the addition of skin-to-skin contact. However, the child should already be breastfeeding for a few minutes prior to the poke rather than attempting to get them on after.
This is one of the most easily modifiable things for a provider to address, and one of the most under-appreciated. Patients should not be supine and should be offered a choice in position when able. Physical restraints should never be used, and parents should never be asked to restrain children as this damages the trust between parent and child.
- For children aged 0–12 mo, toys and music can be helpful.
- For those ages 1–5 yo, there are the additions of bubbles or tablets (iPads and phones).
- Older children, 6–18 yo, may also be able to participate in interactive games.
Interventions
Non-pharmacologic methods have been shown to cause endorphin release and increase descending inhibition of pain from thalamus. These include:
- Physical:
- Massage.
- Heat/cold.
- Acupuncture.
- Positioning
- Behavioral:
- Relaxation therapy.
- Art/play therapy.
- Biofeedback.
- Cognitive:
- Distraction (multimedia, bubbles).
- Guided imagery.
- Hypnosis.
- Prevention and minimization:
- Clustering cares or blood draws.
- Using the smallest gauge needle or least amount of tape.
- When possible, pre-medication with topical or systemic medications prior to procedures.
- Consideration of regional nerve blocks for procedural or chronic neuropathic pain.
The World Health Organization has published principles for the management of acute pediatric pain, including recommendations on timing (the most important of which is the recommendation for use of scheduled medications to avoid the peaks/troughs associated with as needed dosing), collaboration to individualize pain plan, and appropriate route of medication (PO=oral, PR=rectal, IV=intravenous, IM=intramuscular).
The WHO stepwise approach is as follows:
- Mild pain: non-opioid analgesics +/- topical or local anesthetic.
- Moderate pain: Scheduled non-opioid analgesic with intermittent dose of opioid +/- topical or blocks.
- Severe pain: Scheduled non-opioid and opioid analgesics. Consider PCA.
Medications
- Tylenol (PO, PR, IV): Generally, well tolerated without GI or hematological side effects. There is dose dependent hepatotoxicity, thus caution should be taken when using >14 days. The mechanism of action is unknown; however, it is thought to be an inhibitor of serotonergic pathways and affect COX inhibition. It is important to note that rectal formulations are limited to 120 mg or 325 mg, and they cannot be split as uneven distribution can lead to overdose. This is especially important in pediatrics where medications are all dosed based on weight and often have a small range of variation for dosing.
- Ibuprofen (PO): Can cause renal impairment or GI bleeding in high-risk patients due to inhibition of platelet aggregation (specifically those with heart failure or underlying renal disease). There should be caution using this in severe asthmatics as it can precipitate bronchoconstriction, although the reason behind this is not known. Additionally, NSAIDs in general should not be used in infants <6 mo due to poor data on appropriate dosing and unknown risk of renal toxicity.
- Toradol (PO, IV, IM): Multiple studies in post-surgical patients have shown lower pain scores and statistically significant reduction in opioid use in those given toradol immediately post-op. This should be used for no more than 72 hr at a time in children <2 yo and no more than 5 days in children >2 yo. The data on increased post-operative bleeding is mixed and use in surgical patients is surgeon dependent and injury dependent. This is rarely used orally in pediatric patients, but in adults can be used orally for chronic pain patients in the outpatient setting.
- Celecoxib: This is a long-acting NSAID that is good for chronic musculoskeletal pain. It does not have the same bleeding risk as other NSAIDs but is less useful for acute pain or as monotherapy for chronic pain.
- Dissociative agents: Midazolam (IV, intramuscular, intranasal) and ketamine. These do not address pain but do allow for anxiolysis and amnesia.
- Oxycodone (PO, IV): There are various formulations, including immediate release, extended release (OxyContin), Percocet (combined with Tylenol). They undergo CYP3A4 and CYP2DG metabolism. Dosing changes for infants <6 mo, children <50 kg, children >50 kg.
- Morphine (PO, IV, PCA): Metabolized by liver to morphine 3 (inactive) and morphine 6 (active) metabolites. It is important to avoid or reduce the dose in those with renal impairment as metabolites can build up and cause overdose.
- Hydromorphone (PO, IV, PCA): 5x more potent than morphine but with a lower side effect profile. It is metabolized by the liver, and then excreted via the kidneys, but safer to use in renal failure patients than morphine.
- Fentanyl (PO, IV, intranasal, transdermal): 100x more potent than morphine, but much shorter duration of action. Transdermal patches have a long onset to action but last 48–72 hr.
- Side effects of opiates: Most common side effects include:
- Itching.
- Nausea.
- Sedation.
- Urticaria (due to histamine release).
- Constipation (remember to start a bowel regimen).
- There is high risk for sedation and respiratory depression with initiation or large dose changes.
- Specific formulations to avoid in pediatrics include extended or sustained release, combination of weak/strong opioids, Meperidine (Demerol)—neurotoxic metabolites.
- PCA use: Preferred route for older children (>6 yo) needing opioids in moderate to severe acute pain (e.g., vasoocclusive crisis in SCD, post-op from large surgeries, and cancer pain). Although studies have shown a PCA does not decrease overall opioid use and may lead to increased overall use, benefits include:
- Self-regulation.
- Decreased anxiety.
- Avoiding delay in medication administration.
- Risks include over-sedation and respiratory depression, although these risks are low when patients are closely monitoring to adjust dosing. When choosing a medication, the clinician should look at efficacy of past use (morphine versus hydromorphone) and ability to tolerate side effects. At initiation there will be established demand dose, lockout interval, and basal rate. A basal rate should be considered for kids with chronic opioid use, high severity of pain, chronic illness like SCD or cancer. PCA use should be used for the shortest duration possible, and consideration for transitioning off PCA should be made when there is clinical improvement and decreased use of demand dosing. Many providers recommend discontinuation of the basal rate first, trending of demand dosing, and then transitioning to an IV PRN system with scheduled oral medications.
- Codeine: weak (less relief than high dose NSAIDS). The active metabolite is morphine, and variation in metabolism by CyP450 means poor metabolizers (30%) will have poor pain control but the ultra-rapid metabolizers (8%) are at higher risk for overdose. In 2012 there were 3 deaths post tonsillectomy due to respiratory depression, thus there was a black box warning placed, and it was removed from WHO analgesic ladder.
- Tramadol: weak mu receptor agonist and SNRI. It is metabolized by CyP450 to O-desmethyltramadol which is the active metabolite that exerts effect. Common side effects are nausea, vomiting, constipation, and over-sedation. There is a higher risk for serotonin syndrome, and it can lower seizure threshold. It was removed from the WHO analgesic ladder in 2012 after 3 documented deaths in Europe.
- Combined products (Vicodin, Percocet): Not recommended as the daily Tylenol limits restrict optimizing the opiate dosing, and families using Tylenol as needed with a combined product are at high risk for miscalculation and Tylenol overdose.
-
racial and ethnic disparities in pediatric pain management
Multiple studies have demonstrated that there are racial and ethnic disparities in pediatric pain management (see references below), with African American and Hispanic children less likely to receive optimal pain management in emergency departments compared to non-Hispanic white children in cohorts presenting with limb fractures or appendicitis. The authors of these studies concluded that monitoring of variations in pain management practice using both process and outcome measures is warranted in order to eliminate such disparities.
- Committee on Psychosocial Aspects of Child and Family Health. Task Force on Pain in Infants, Children, and Adolescents. The Assessment and Management of Acute Pain in Infants, Children, and Adolescents. Pediatrics September 2001; 108 (3): 793–797.
- Children, Opioids, and Pain: The Stats & Clinical Guidelines. Practical Pain Management. 2018; Volume 18, Issue #9, 18–20.
- Ellis JA, O’Connor BV, Cappelli M, Goodman JT, Blouin R, Reid CW. Pain in hospitalized pediatric patients: How are we doing? Clin J Pain. 2002 Jul–Aug;18(4):262–9.
- Hauer J, Houtrow AJ; SECTION ON HOSPICE AND PALLIATIVE MEDICINE, COUNCIL ON CHILDREN WITH DISABILITIES. Pain Assessment and Treatment in Children With Significant Impairment of the Central Nervous System. Pediatrics. 2017 Jun;139(6):e20171002.
- Lee GY, Yamada J, Kyololo O, Shorkey A, Stevens B. Pediatric clinical practice guidelines for acute procedural pain: a systematic review. Pediatrics. 2014 Mar;133(3):500–515.
- Stevens BJ, Hathway G, Zempsky WT. Oxford Textbook of Pediatric Pain. Oxford University Press, Incorporated; 2014
- Nixon RD, Nehmy TJ, Ellis AA, Ball SA, Menne A, McKinnon AC. Predictors of post-traumatic stress in children following injury: The influence of appraisals, heart rate, and morphine use. Behav Res Ther. 2010 Aug;48(8):810–815.
- Pain Medicine, Palliative and Integrative Medicine. Childrens Minnesota.
- Schreiber S, Ronfani L, Chiaffoni GP, Matarazzo L, Minute M, Panontin E, Poropat F, Germani C, Barbi E. Does EMLA cream application interfere with the success of venipuncture or venous cannulation? A prospective multicenter observational study. Eur J Pediatr. 2013 Feb;172(2):265–8.
- Smith HS. Opioid metabolism. Mayo Clin Proc. 2009 Jul;84(7):613–24.
- Taddio A, Chambers CT, Halperin SA, Ipp M, Lockett D, Rieder MJ, Shah V. Inadequate pain management during routine childhood immunizations: the nerve of it. Clin Ther. 2009;31 Suppl 2:S152–67.
- Weisman SJ, Bernstein B, Schechter NL. Consequences of inadequate analgesia during painful procedures in children. Arch Pediatr Adolesc Med. 1998 Feb;152(2):147–9.
- Ammentorp J, Mainz J, Sabroe S. Parents’ priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med. 2005 Feb;159(2):127–31.
- Guideline for the management of chronic pain in children. World Health Organization Maternal, Newborn, Child, and Adolescent Health and Ageing (MCA) Department. 2020.
- Monika K. Goyal, Tiffani J. Johnson, et. al. PEDIATRIC EMERGENCY CARE APPLIED RESEARCH NETWORK (PECARN). Racial and Ethnic Differences in Emergency Department Pain Management of Children With Fractures. Pediatrics May 2020; 145 (5): e20193370.
- Guedj R, Marini M, Kossowsky J, Berde CB, Kimia AA, Fleegler EW. Racial and Ethnic Disparities in Pain Management of Children With Limb Fractures or Suspected Appendicitis: A Retrospective Cross-Sectional Study. Front Pediatr. 2021 Aug 3;9:652854.
Image credits
Unless otherwise noted, images are from Adobe Stock.