



Least reliable at delivering a specific FiO2. Usually <30% FiO2 at 10L/min of flow. Can try temporarily if a child is agitated with anything else but should be used as a stop gap while another method is being prepared.

Setting suggestions: 10L, FiO2 100%.
Consider: Least reliable at delivery a specific FiO2 usually <30% FiO2 at 10L.
Rarely used anymore but previously used in the neonatal population. Start 2–3 L/min. Difficult to maintain higher oxygen concentrations due to the large neck opening and less than optimal seal around the edges.
Setting suggestions: 2–3L, FiO2 30–90%.
Consider: Higher flow rates can increase rebreathing carbon dioxide. Difficult to obtain higher oxygen concentrations with large neck opening and less than optimal seal around the edges.
Standard flow rates (below). Can increase up to 5–6L/min but then need to humidify. Positive end expiratory pressure (PEEP) production is unpredictable, so even just 2L/min in neonates can give excess PEEP that puts them at higher risk for pneumothorax or lung injury.

Setting suggestions:
- 0.5–1L in neonate.
- 1–2L in infant.
- 1–4L children.
- FiO2 28–44%.
Consider: Rates >4L can cause mucosal irritation and discomfort.
Heated and humidified. Flow rates are often weight based, with variation nationwide on starting liter flow recommendations. Often start at 0.5L/min/kg in neonates/smaller children or 10L/min in older kids/adolescents, but units differ on what they offer for flow rate and thus make sure your circuit matches the flow you expect to need. Can go as high as 40L/min but should be in the ICU setting at that point. Benefits include:
- Extra-thoracic dead space washout.
- More consistent PEEP.
- Increased pulmonary compliance.
Other than liter flow, you can also give more FiO2, although the amount the patient gets is not as high as you set, as it’s affected by breathing pattern and leakage).
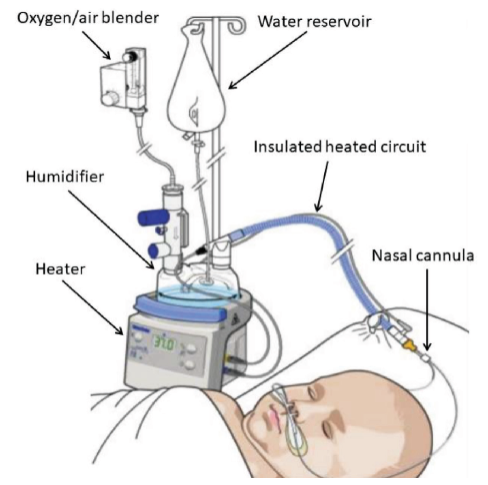
Setting suggestions:
- Start at 0.5–1L/kg and increase up to 8L in infants, up to 40L in adolescents.
- FiO2 20–100%.
Consider: Always use blenderized oxygen instead of off the wall. Patients can tolerate higher flow rates due to 100% FiO2. Can cause gastric distention, consider decompression.
Start at 6–10 L/min. Allows CO2 to stay in mask and will be re-breathed. Not often used in pediatrics but can be used as a stop gap as other methods are being prepared or if there is a child that absolutely will not tolerate nasal cannula.

Setting suggestions: 6–10L, FiO2 100%.
Consider: Allows CO2 to stay in mask and will be re-breathed, so switch to NC if low settings. Not well tolerated in pediatric patients.
Start at 10–15 L/min. It reaches 95% FiO2 because mixing of gases is limited thanks to the 2 valves. This modality offers the highest oxygen concentration that can be delivered to a spontaneously breathing patient. Partial non-rebreather can provide FiO2 concentrations 40–60% at 4–6 L/min and are similar to simple facemasks but have a reservoir causing mixing of fresh oxygen supply with expired gas.

Setting suggestions:10–15L, FiO2 100%.
Consider: Reaches 95% FiO2 b/c mixing of gases is limited thanks to the 2 valves. Highest O2 concentration that can be delivered to a spontaneously breathing patient.
For cases of hypercapnia or assisted breathing for hypoxemia. Continuous positive airway pressure (CPAP) is one constant pressure, like constant PEEP throughout the breathing cycle. BiPAP is a type of noninvasive positive pressure ventilation (NIPPV) in which you set an inhale and exhale pressure (IPAP and EPAP). These should be avoided in cases of altered mental status or when there is a higher aspiration risk. For obstructive sleep apnea, CPAP is often used at a lower pressure to allow for comfort. For those patients requiring higher pressures, bipap may be more comfortable.

Setting suggestions: Discuss with pulmonology.
Consider:
- CPAP is one constant pressure, like constant PEEP.
- BiPAP is a type of NIPPV, you set an inhale and exhale pressure (IPAP and EPAP). Do not use in cases of altered mental status or aspiration risk.
- For OSA, CPAP comfortable if mild to moderate level of pressure. If higher, bipap may be more comfortable for them.