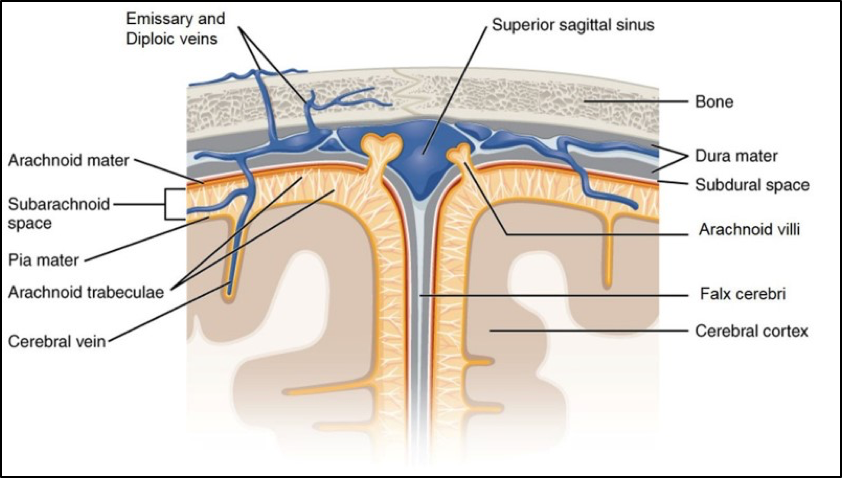
Figure 2.1. Meninges and meningeal spaces. By OpenStax, CC BY 4.0. Modified July 9, 2018, by Lampa.
The meninges can be subdivided into cranial and spinal portions.
The meninges function to protect, to act as a scaffold supporting blood vessels and venous sinuses, and finally to form a continuous sac, the subarachnoid space, for the flow of cerebrospinal fluid (CSF).
This should be review and reinforce the information discussed in FMS 501; see Figure 2.1.
The meninges in the cranial cavity are as follows:
The dura mater
The tough outer fibrous layer
The arachnoid mater
The middle thin layer
The pia mater
The delicate inner layer
The pia mater (from the Latin word pia, meaning “tender”): This membrane closely invests the external surface of the CNS.
Pia mater follows all the contours of the brainstem and cortex. Arachnoid trabeculae span the subarachnoid space and merge with the pia mater, making it very difficult to distinguish between the two layers.
Cerebral arteries and veins travel in the subarachnoid space and are anchored to the pia by sheets and strands of connective tissue, before penetrating the cerebral cortex.
pad
An acronym for meningeal layers from inside to outside
The dura mater in the skull consists of two layers: the periosteal and meningeal layers.
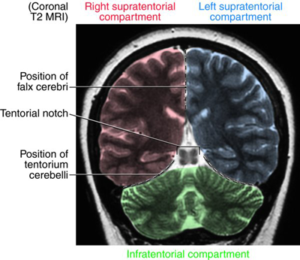
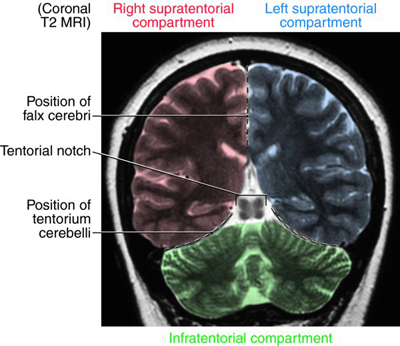
The main dural reflections in the cranial cavity are the falx cerebri between the two cerebral hemispheres and the tentorium cerebelli between the cerebral hemispheres and the cerebellum (review from FMS 501).
The falx cerebri (Latin falx = “sickle”) is a long, arched vertical sheet of dura mater occupying the longitudinal fissure
Anteriorly, the falx cerebri attaches to the crista galli of the ethmoid bone. The falx cerebri curves posteriorly, fusing on the midline with the tentorium cerebelli.
The inferior free-edge of the falx cerebri parallels the corpus callosum.
The supratentorial compartment contains the cerebrum.
The infratentorial compartment contains the brain stem and cerebellum.
Posteriorly, the tentorium cerebelli attaches to the occipital bone, laterally it attaches along the petrous portion of the temporal bone, and anteriorly it attaches to the clinoid processes of the sphenoid.
The free edges of the tentorium cerebelli curve anteriorly, nearly encircling the midbrain. The brainstem passes through the tentorial notch (or tentorial incisure).
Soft-tissue structures (i.e., cranial nerves III and IV) may get compressed against the tentorium, leading to neurologic deficits such as pupillary dilation and impaired eye movement.
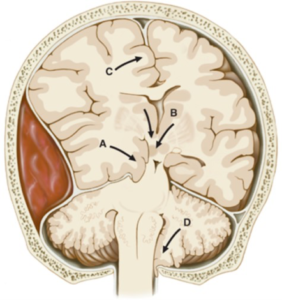
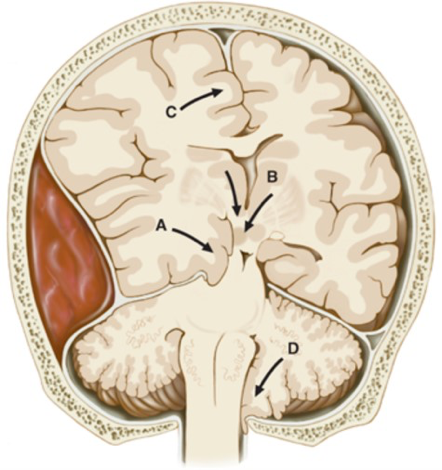
Figure 2.3. Herniations of the Central Nervous System. Increased Intracranial Pressure and Head Trauma, Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson J, Loscalzo J. Harrison’s Manual of Medicine, 19e; 2016. Accessed July 17, 2018.
Increases in intracranial pressure leads to herniations; A is a herniation of the temporal lobe (uncal herniation) into the midbrain or B is showing a herniation of the thalamus (central) into the midbrain can occur. Both of these herniation are the result of the tentorial notch.
A herniation of the cerebellar tonsil (foraminal) into the foramen magnum may cause death because of compression of the vital centers within the medulla (D).
A mass or swelling can force the temporal lobe inferiorly into the tentorial notch (incisura), leading to an uncal herniation. Damage to the uncus may result in disturbances in olfaction. Compression of the midbrain from an uncal herniation can lead to 3rd nerve damage that may also lead to stupor or coma if the compression is not treated. See Figure 2.3.
Review
A mass associated with the parietal lobe expands toward the midline. This might cause the ipsilateral cingulate gyrus to herniate:
Meningeal spaces
The meningeal spaces in the cranial cavity are only present between the periosteum and dura (epidural) and dura and arachnoid (subdural) in pathological conditions, like hematomas or hemorrhages. Otherwise these two meningeal spaces are “potential.”
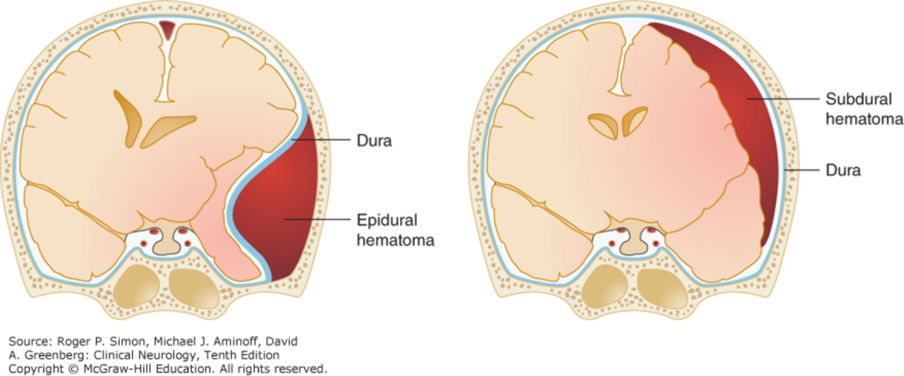
Figure 2.4. Hematoma into the meningeal spaces. Confusional States, Simon RP, Aminoff MJ, Greenberg DA. Clinical Neurology, 10e; 2017. Accessed July 17, 2018.
Bleeding from a rupture of meningeal vessels passes into the epidural space, an epidural hematoma. Bleeding associated with the cerebral veins can pass into the subdural space, a subdural hematoma. (See Figure 2.4.)
Both epidural and subdural hematoma have distinct radiographic signs. An epidural hematoma is lens-shaped and restricted by the sutural attachments of the dura mater and a subdural hematoma is crescent-shaped following the convexity of the cerebral hemisphere. (See Figure 2.4.)
The only “real” space in the cranial cavity is the subarachnoid space containing cerebrospinal fluid. The subarachnoid space besides containing CSF can also fill with blood from a rupture of cerebral arteries forming a subarachnoid hemorrhage (subarachnoid hematoma).
The meningeal spaces can also be involved in other pathologic processes like cysts, tumors, and certain infections.
Both epidural and subdural hematomas also lead to increases in intracranial pressure.
Table 2.1. Comparison of cranial vs. spinal meninges
Cranial
Spinal
Dura
Adherent to the skull (no epidural space), especially at the coronal and sagittal sutures
The attachment to sutures gives a distinct crescent-shaped appearance of an epidural hematoma that can be viewed on MRI or CT scans
Composed of two fused layers (periosteal and meningeal), which split and form the venous sinuses
Separated from vertebrae by epidural space (containing fat and blood vessels)
Composed of only one layer
Arachnoid
Attached to dura in the living (no subdural space)
Arachnoid villi (in superior sagittal sinus)
Arachnoid trabeculae
Subarachnoid space with multiple cisterns (e.g. cisterna magna, pre-pontine)
Attached to dura in the living (no subdural space)
Few or no arachnoid trabeculae but larger arachnoid septae
Subarachnoid space with a large lumbar cistern
Pia
Intimately adherent to surface of brain
No pial specializations
Follows vessels as they pierce the cerebral cortex
Intimately adherent to surface of the spinal cord
Specializations form the denticulate ligaments and filum terminale
Follows vessels as they pierce the spinal cord
Intracranial mass lesions and intracranial pressure
Any abnormality occupying a volume in the cranial cavity functions as a mass. These abnormalities include: hemorrhages (hematomas), arteriovenous malformations, abscesses, edema, and tumors.
Intracranial mass lesions and neurologic symptoms
Compression and/or destruction of neuronal tissue leads to neurologic abnormalities.
Increases in intracranial pressure leading to neurologic symptoms.
Physical displacement (herniations) of CNS structures into other compartments where the neuronal tissue is normally not found.
A common example of a mass lesion is an epidural hematoma. Initially, the brain is able to compensate for a small rise in intracranial pressure, from small hemorrhages, by decreasing CSF and blood volume. The increasing size of a mass makes it so that the brain is unable compensate, and intracranial pressure rises dramatically leading to decreases in cerebral perfusion and ultimately herniations and/or neuronal ischemia.
Key concept
Elevated intracranial pressure causes a decrease in cerebral perfusion and brain ischemia.
Physical signs of elevated intracranial pressure include:
Headache
Altered mental status (irritability and depressed level of alertness)
Nausea and vomiting (emesis)
Papilledema (swelling of the optic disc)
Visual loss
Diplopia (double-vision)
An autonomic reflex in response to increased intracranial pressure (ICP) can lead to the symptoms of hypertension, bradycardia, and irregular respirations.
Increasing ICP that forces nervous tissue into the midbrain can also lead to a loss of consciousness and stupor.
If left untreated, severely elevated intracranial pressure causes irreversible brain damage and death, sometimes within a few hours.
Ventricular system
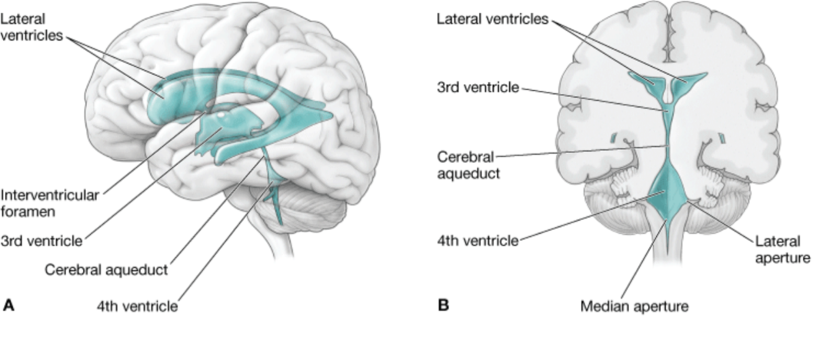
Figure 2.5. The ventricular system. Chapter 16. Brain, Morton DA, Foreman K, Albertine KH. The Big Picture: Gross Anatomy; 2011. Accessed July 17, 2018.
The cavities of the developing secondary brain vesicles (see FMS 512_CNS Development notes) form the ventricular system in the cerebrum and brain stem (Figure 2.5).
All the ventricles contain networks of capillaries, the choroid plexuses, which produce CSF.
Lateral ventricles
Third ventricle
Fourth ventricle
The lateral ventricles consist of anterior, posterior, and inferior horns, as well as a body and atrium (trigone).
A thin membrane, the septum pellucidum, separates the two lateral ventricles in the midline. Exiting the lateral ventricles are interventricular foramina (foramen of Monro), which connect into the third ventricle.
Remembering the shape and location of the lateral ventricles is important for understanding the structures of the cerebrum whose shape follows the contour of the lateral ventricles. These structures in the cerebrum include the corpus callosum, caudate nucleus, fornix, and hippocampus.
Located between the two halves of the diencephalon.
Exiting the third ventricle is the cerebral aqueduct (aqueduct of Sylvius).
The cerebral aqueduct is located posterior to the tegmentum and anterior to tectum of the midbrain.
The floor is formed by the rhomboid fossa and the roof by superior medullary velum and superior cerebellar peduncle.
Apertures exiting the 4th ventricle include a median (of Magendie) and two lateral (of Lushcka) foramina leading into the subarachnoid space.
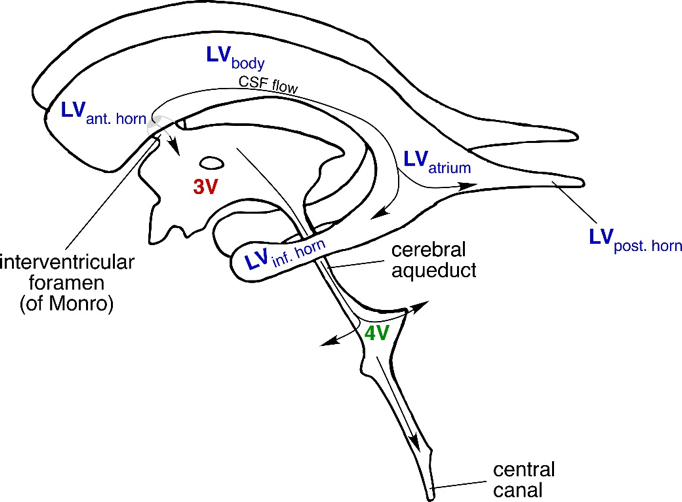
Figure 2.6. Diagram of ventricular system. LV: Lateral ventricle 3V: Third ventricle 4V: Fourth ventricle. From Neuroanatomy: A Laboratory Guide (2e); Jansen and Lampa.
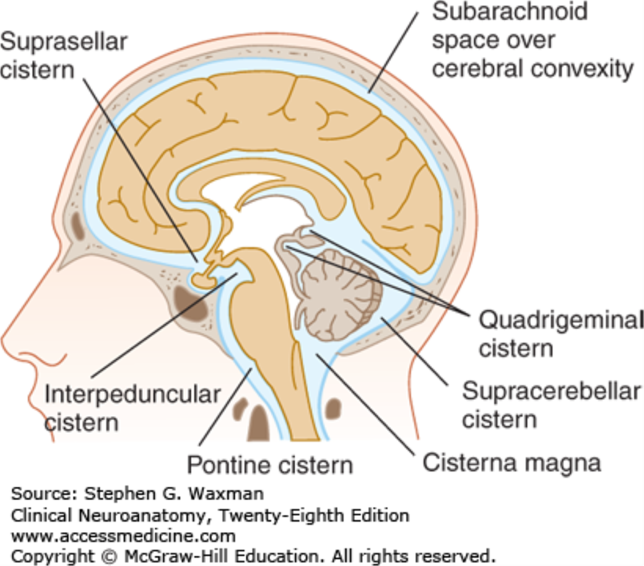
Figure 2.7. Subarachnoid cisterns. Ventricles and Coverings of the Brain, Waxman SG. Clinical Neuroanatomy, 28e; 2017. Accessed July 17, 2018.
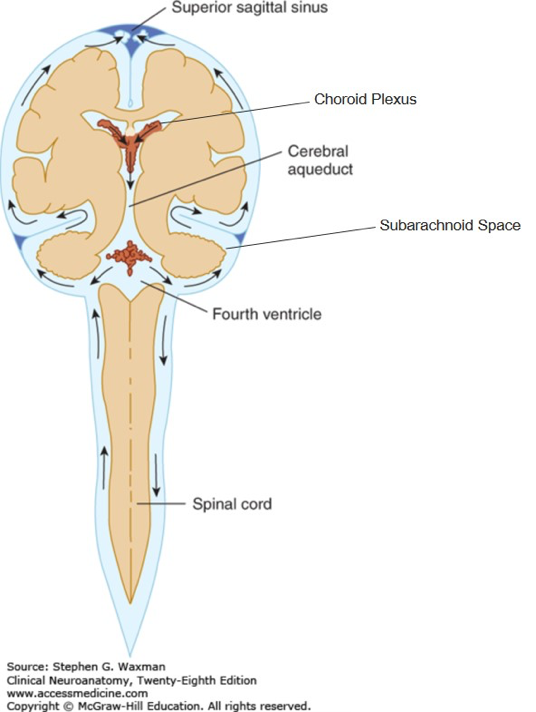
Figure 2.8. Flow of cerebrospinal fluid. Ventricles and Coverings of the Brain, Waxman SG. Clinical Neuroanatomy, 28e; 2017. Accessed July 17, 2018.
After leaving the ventricular system, CSF courses through the subarachnoid space. Within the subarachnoid space are cisterns (L. cistern = a reservoir) where CSF can accumulate. See Figure 2.7. In a T2-weighted MRI, vessels and nerves in the subarachnoid cisterns surrounding the brainstem can be observed. Also, the reduction of these cisterns can occur with pathologic conditions.
Major subarachnoid cisterns include: quadrigeminal, interpeduncular, (pre)pontine (ventral to the pons); the cisterna magna (around the foramen magnum), suprasellar, and the lumbar (expansion of subarachnoid space from L3–S2 (not pictured in Figure 2.7).
The schematic in Figure 2.8 shows the cerebrum overlying the thalamus and brain stem. The small arrows represent the direction of the flow of cerebrospinal fluid.
Review from FMS 501
A lumbar puncture is commonly performed to remove CSF from or inject anesthetic into the lumbar cistern. A lumbar puncture is performed with the patient lying down because the pressure is much lower when there isn’t a resistance associated with gravity. A lumbar puncture is usually performed in between the last couple lumbar vertebrae (L4 or L5).
Thought question
Why is a lumbar puncture done at the above location?
Cerebrospinal fluid (CSF)
Cerebrospinal fluid (CSF) is mostly produced from arterial blood by the choroid plexuses of the lateral, 3rd, and 4th ventricles by a combined process of diffusion, pinocytosis, and active transport. A small amount of CSF is also produced by ependymal cells and other extracellular fluids.
The choroid plexuses are tufts of capillaries with thin, fenestrated endothelial cells covered by modified ependymal cells.
Functions of CSF include:
To cushion and protect the brain and spinal cord from shocks and trauma, as well as support of the venous sinuses. CSF increases the buoyancy of the brain, which reduces momentum and acceleration during severe displacement of the cranium.
Playing important roles in the homeostasis and metabolism of the central nervous system.
FYI
The increased buoyancy of CSF makes a 1500 g brain in air, weigh 50g when floating in CSF.
CSF is usually acellular; but the presence of a few cells in the CSF is not an abnormal finding. The finding of more cells than normal is indicative of a pathologic process. The presence of red blood cells in CSF leads to yellow-tinged CSF, xanthochromia.
The total volume of CSF in the adult is about 150 ml (cc). A total volume ~25 ml is found in ventricles with the remainder being contained in the subarachnoid space.
CSF is produced at a rate of 500–600 ml/day.
CSF is reabsorbed across the arachnoid villi into the venous circulation. The arachnoid villi act as one-way valves between the subarachnoid space and the dural sinuses.
The rate of reabsorption of CSF correlates with the CSF pressure. The pressure of CSF is normally greater than the venous system, facilitating the bulk flow of CSF into the venous sinuses.
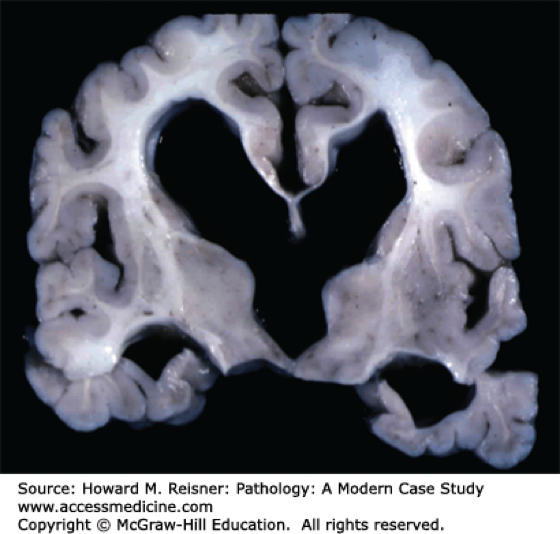
Figure 2.9. Enlarged lateral and 3rd ventricles. Pathology of the Nervous System, Reisner HM. Pathology: A Modern Case Study; 2015. Accessed July 27, 2018.
Non-communicating hydrocephalus—also called “obstructive” hydrocephalus—occurs when the flow of CSF is blocked in the ventricular system; this is the most common form of hydrocephalus (Figure 2.9). Congenital defects of the embryonic ventricular system involving faulty canalization/narrowing of passageways lead to this condition. Other causes may include tumors or abscesses.
One of the most common locations of this narrowing is the cerebral aqueduct, aqueductal stenosis, between the 3rd and 4th ventricles.
Other locations for obstructive hydrocephalus are where the lateral ventricles drain into the third ventricle at the interventricular foramen and where the 4th ventricle opens via the lateral foramina.
Atrophy of brain tissue may also occur if non-communicating hydrocephalus remains untreated.
Communicating hydrocephalus—also called “non-obstructive”—occurs when the flow of CSF is blocked after exiting the ventricles. This form is called communicating because the CSF still flows between the ventricles.
Communicating (non-obstructive) hydrocephalus shows enlarged sulci on an MRI, which is due to an increase of CSF in the subarachnoid space.
The most common cause of communicating hydrocephalus is the inability of arachnoid villi to reabsorb CSF.
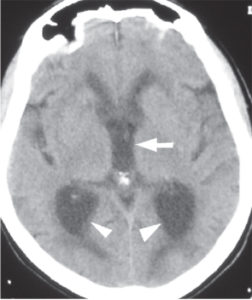
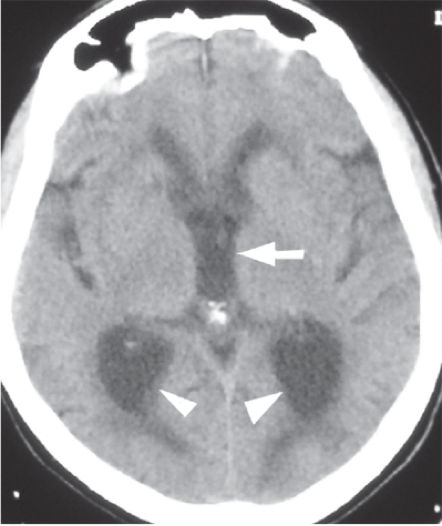
Figure 2.10. CT of patient w/ normal pressure hydrocephalus. Note the dilated atria of the lateral ventricles (arrowheads) and rounded third ventricle (arrow) on this image. This is from a patient with normal pressure hydrocephalus. Neurosurgery, Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE. Schwartz’s Principles of Surgery, 10e; 2014. Accessed: July 27, 2018.
Abnormalities in the production, absorption, or flow of CSF result in ventricular dilatation, with no increases in overall intraventricular pressure. This is oftentimes an idiopathic disorder that is most common after 60 years of age.
A group of clinical findings that is characteristic of NPH includes: a slowly progressive gait disorder that is usually the earliest feature, followed by impaired of mental function and, later, urinary incontinence.
Review
A 6-year-old comes in with obstructive (non-communicating) hydrocephalus. An MRI shows enlargement of the lateral ventricles, but the other parts of the ventricular system appear normal. Which portion of the ventricular system is likely occluded?
Case study: Felipe Moreno
Tap the arrow to view the case.
A 75-year-old gentleman. Felipe Moreno, is brought in by his family because of a 6-month history of progressive difficulty with walking and balance and a 4-month history of urinary incontinence. Further inquiry reveals that, while he was once gregarious and busy with any one of dozens of projects, he now spends his days quietly sitting alone, staring into space.
On a neurologic exam, Felipe generally answers appropriately when asked a question, but only with single words or short sentences without elaboration. If given several tasks in sequence, he will at best complete one of them (motor impersistence). For example, if asked to write a note, fold the paper, put it in an envelope, and seal it, he may simply write one word on the paper.
Felipe cannot rise to a standing position without assistance. As he attempts to walk, his feet appear to be glued to the floor (magnetic gait). Eventually he is able to make wide-based steps, and he also has stiffness and is unable to pivot properly.
A ventriculoperitoneal shunt was placed, and Felipe's gait and urinary incontinence improved markedly, but he still had lingering significant cognitive impairment.
Describe some possible causes of NPH in this patient.
Review
What brain regions might be affected to produce the gait apraxia (motor planning)?
Treatment
Hydrocephalus can be treated by surgical intervention when a shunt is implanted to divert the flow of CSF from the ventricular system to another area of the body or the blood stream.
Ventriculo-peritoneal (VP) shunt
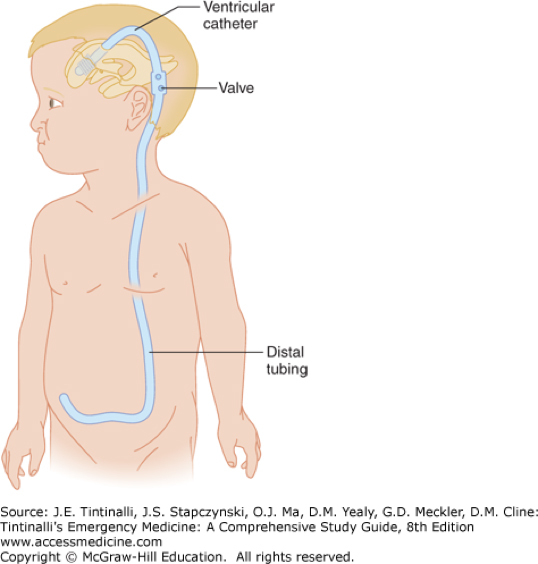
Figure 2.11. Ventriculo-peritoneal shunt. Central Nervous System Procedures and Devices, Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e; 2016. Accessed July 27, 2018.
A ventriculo-peritoneal (VP) shunt has been used for more than 40 years to alleviate the pressure associated with hydrocephalus. In this procedure, one end of the catheter is placed within a brain ventricle or the subarachnoid space of the spinal cord. The other end of the catheter is commonly placed within the peritoneal cavity to drain the CSF. (See Figure 2.11.) A catheter may also be placed at other sites, such as in a chamber of the heart or the pleural cavity where the CSF can also be drained and reabsorbed. A valve located in the catheter maintains has a one-way flow that regulates the rate of CSF being drained.
The blood-brain barrier
Review from FMS 503
The concept of a blood-brain barrier (BBB) arose from early observations that many substances, when injected into the bloodstream, do not gain access to the brain.
Endothelial cells of the blood-brain barrier restrict diffusion of microorganisms and large molecules into the CSF, while allowing the transfer of small molecules (O2, hormones, or CO2). Cells of the blood-brain barrier are involved in the active transport metabolic products such as glucose across the barrier by specific proteins.
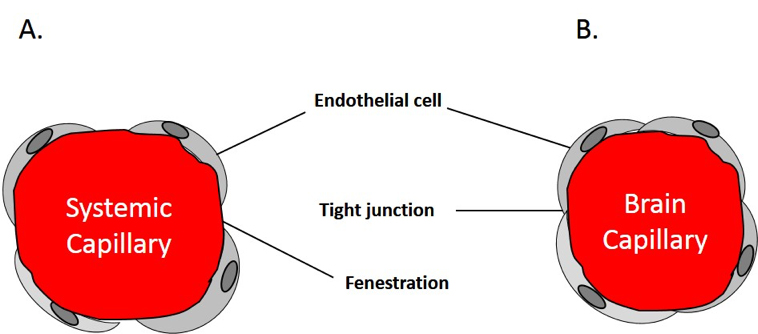
Figure 2.12. Systemic vs. brain capillaries.
The concept of the blood-brain barrier was directly visualized by work of Karnovsky et al., who found endothelial cells of the brain were different from peripheral endothelial cells in the following ways:
1.
First, brain endothelial cells are joined by tight junctions of high electrical resistance, providing an effective barrier against certain molecules.
2.
Second, peripheral endothelial cells have good trans-cellular movement of molecules. There is no such trans-cellular movement in brain endothelial cells.
3.
Finally, most brain capillaries are in contact with foot processes of astrocytes, which essentially separates the capillaries from the neurons.
Clinical correlation
The complex barrier system between the blood and neuronal tissue is a mixed blessing. For example, it is very efficient for keeping microorganisms out of the brain, but it is as equally efficient at keeping many pharmacological agents out. Therefore, intracranial infections can be difficult to treat.
The BBB can also be damaged so it becomes permeable in many pathologic conditions affecting the CNS. These may include stroke, Alzheimer’s disease, Parkinson’s disease, bacterial infections, Multiple Sclerosis, HIV, to name a few.
A blood-CSF barrier also exists that is made from tight junctions between the ependymal cells of the choroid plexus epithelium.
Image credits
Unless otherwise noted, images are from Adobe Stock.