Neurulation and formation of the Central Nervous System
A quick review of neurulation from FMS 501 . . .
1. After migration and patterning, the dorsal layer of ectoderm further differentiates into neuroectoderm.
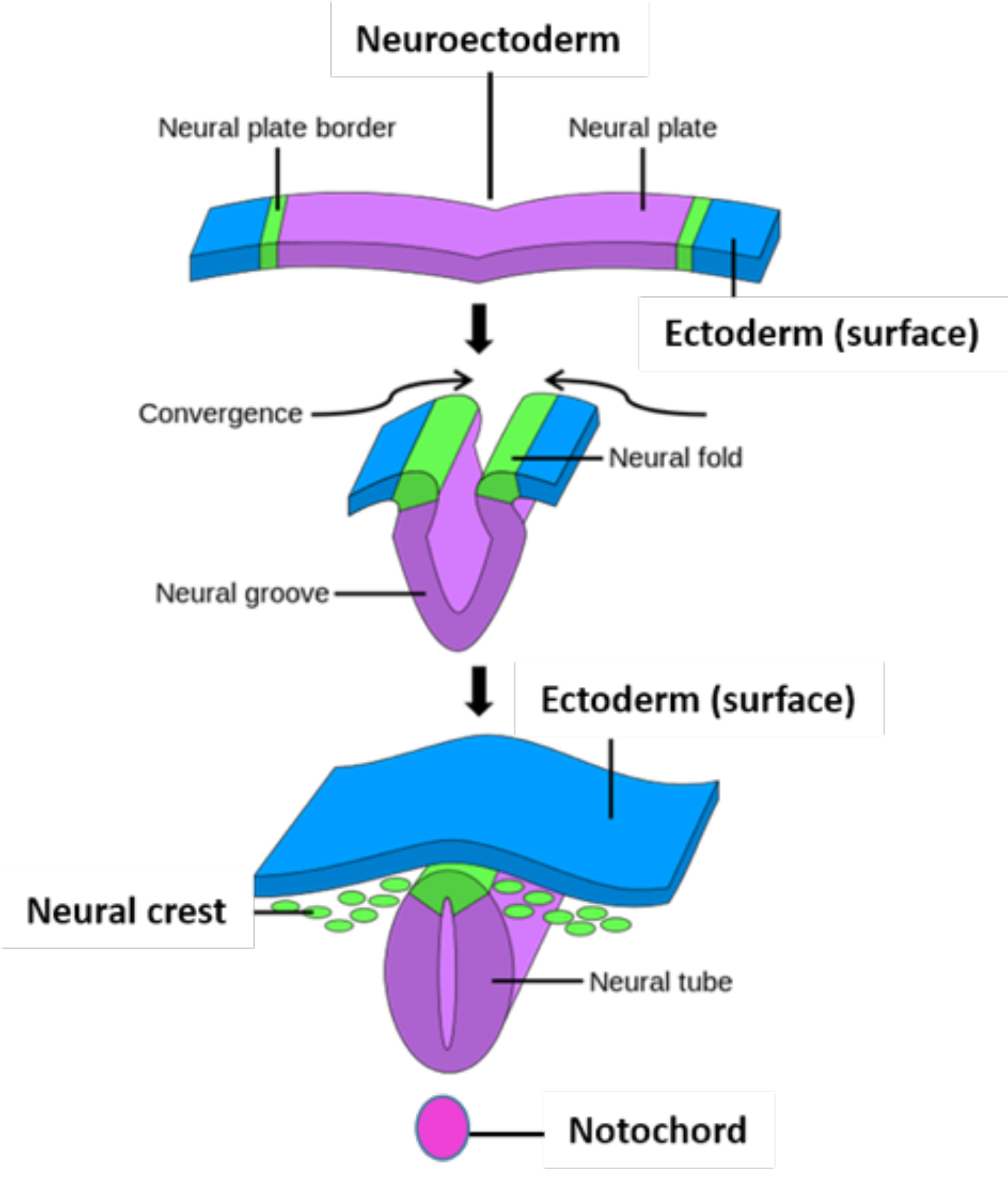
Figure 1.1. Neurulation and neural crest formation. Commons.wikimedia.org.
Neuroectoderm begins to invaginate at ~18 days, forming a neural groove between paired neural folds. The neural folds later fuse dorsally, forming a neural tube. This process is called neurulation. (See Figure 1.1.)
Fusion of neural tube begins in the cervical region of the embryo and proceeds cranial (rostral) and caudal to the spot of initial fusion.
A central cavity forms within the neural tube called the neural canal.
The critical structure necessary for inducing neurulation is the notochord. The notochord releases signaling molecules which are important for formation of the neural tube. One of the molecules released by the notochord is the signaling protein sonic hedgehog (SHH). It has been shown that SHH is necessary for both migration and formation of motor neurons that will populate the developing neural tube.
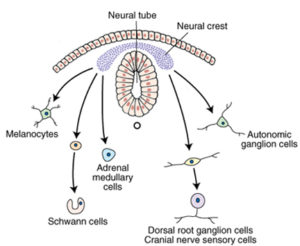
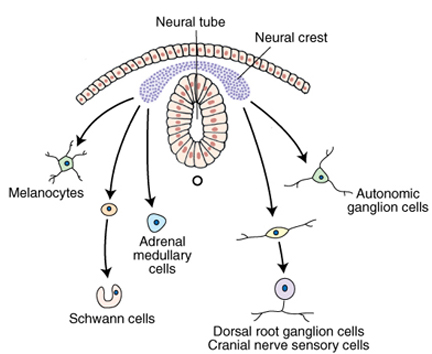
2. Neural crest cells develop along the lateral margin of the neural folds.
Neural crest cells can differentiate into a plethora of structures associated with the developing nervous system.
Defects in neural crest migration can lead to different congenital defects. These rare defects include aganglionosis of the developing gut (Hirschsprung’s Disease), tumors associated with the developing adrenal gland and sympathetic ganglia (neuroblastoma), albinism, deafness, and defects in the cardiac outflow tract.
3. After neurulation, a primitive brain and spinal cord are formed and then the neuroepithelial cells lining the closed neural tube begin the process of differentiation.
The brain and brain stem develops from the broader cranial (cephalic) portion of the neural tube and is characterized by a number of dilations called brain vesicles.
The spinal cord develops from the narrow caudal portion of the neural tube.
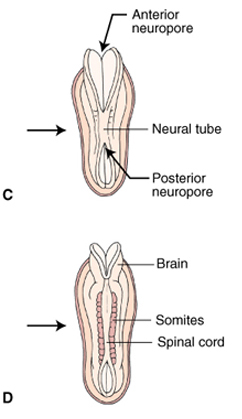
Both ends of the neural tube communicate with the amniotic cavity through large openings, the anterior (rostral) and posterior (caudal) neuropores (Figure 1.3).
Neuronal and non-neuronal structures formed from neural crest cells
Cranial nerve ganglia (III, V, VII, VIII, IX, and X)
Schwann cells
Pia and arachnoid mater
Adrenal medulla
Melanocytes (skin pigment cells)
Odontoblasts
Review 1.1.
A pediatric patient has a neuroblastoma associated with the adrenal medulla. This tumor could be related to a pathological disturbance of which of these embryonic structures?
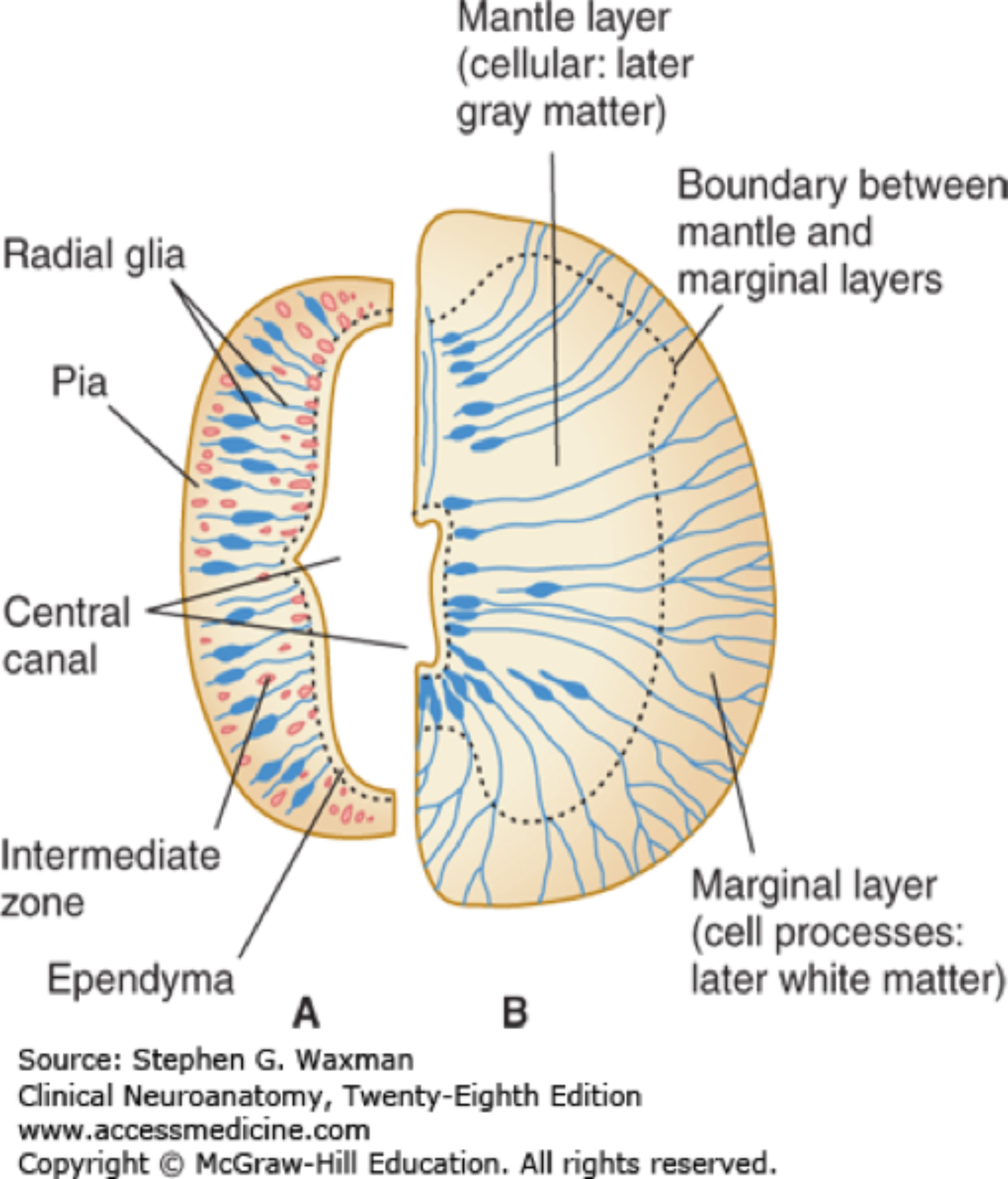
The epithelium of the neural tube differentiates, forming three distinct zones. A brief description of each of these zones are as follows. Figure 1.4 illustrates the two phases of neural tube development neuroblast formation and migration.
1. A ventricular (ependymal) zone (a neuroepithelial layer)
The inner-most zone contains mitotically active cells which give rise to the cells that will populate the intermediate (mantle) zone. The neuron-forming cells are called neuroblasts. Once neuroblasts form, they are unable to divide further. After mitotic activity ceases, the remaining cells of the ventricular zone will become the ependymal cells of the brain ventricles and the central canal.
2. Intermediate (mantle) zone
The neuroblasts from the ventricular zone migrate into this zone and differentiate into neurons, astrocytes, and oligodendrocytes. Neuronal cells in this zone will form the gray matter of the brain stem and spinal cord.
3. Marginal zone (outer layer)
Neuroblasts developing in the intermediate zone of the spinal cord send axons which project peripherally; these myelinated axons will form the white matter of the spinal cord.
The positioning of the gray and white matter in the brain versus the brain stem and spinal cord is due to differences in the migration of neuroblasts. (See slide 12 from CNS Development Lecture.)
In the cerebral cortex, the neuroblasts migrate peripherally and send their axons centrally. The neuroblasts migrate along specialized radial glia cells to begin population of the developing cerebral cortex.
Neurons stay centrally located and their axons project peripherally in the spinal cord and brainstem.
Factors involved in neuronal proliferation include:
Birth and differentiation of neurons within the ventricular zone of the developing neural tube.
Migration to proper brain regions—developing and migrating neurons travel along the processes of radial glial cells.
Growth and pruning of axons to their appropriate targets.
(This involves many signaling factors that will not be discussed, as this is not a developmental neuroscience course.)
Generation of synapses between interacting neurons, synaptogenesis relies primarily on the interaction of intrinsic trophic factors within the CNS and is largely independent of environmental events.
Neurogenesis occurs mainly during the 3rd to 5th months of development. But, a caveat of this is that neuronal connections and myelin production continues until well after birth. It has also been shown that neurogenesis still occurs in portions of the subventricular zone of the hippocampus and olfactory bulbs in the adult (Eriksson et al., 1998; Curtis et al., 2012).
Environmental factors such as drugs, alcohol, and viral illnesses may disrupt normal brain development during critical periods of CNS development by affecting the actively dividing neuronal precursors.
Brain vesicle formation
1. The brain, brain stem, and cerebellum form from primitive swellings in the rostral (anterior) part of the neural tube.
After closure of the neural tube, the cranial part bends ventrally and enlarges to form the simple parts of the brain and brain stem.
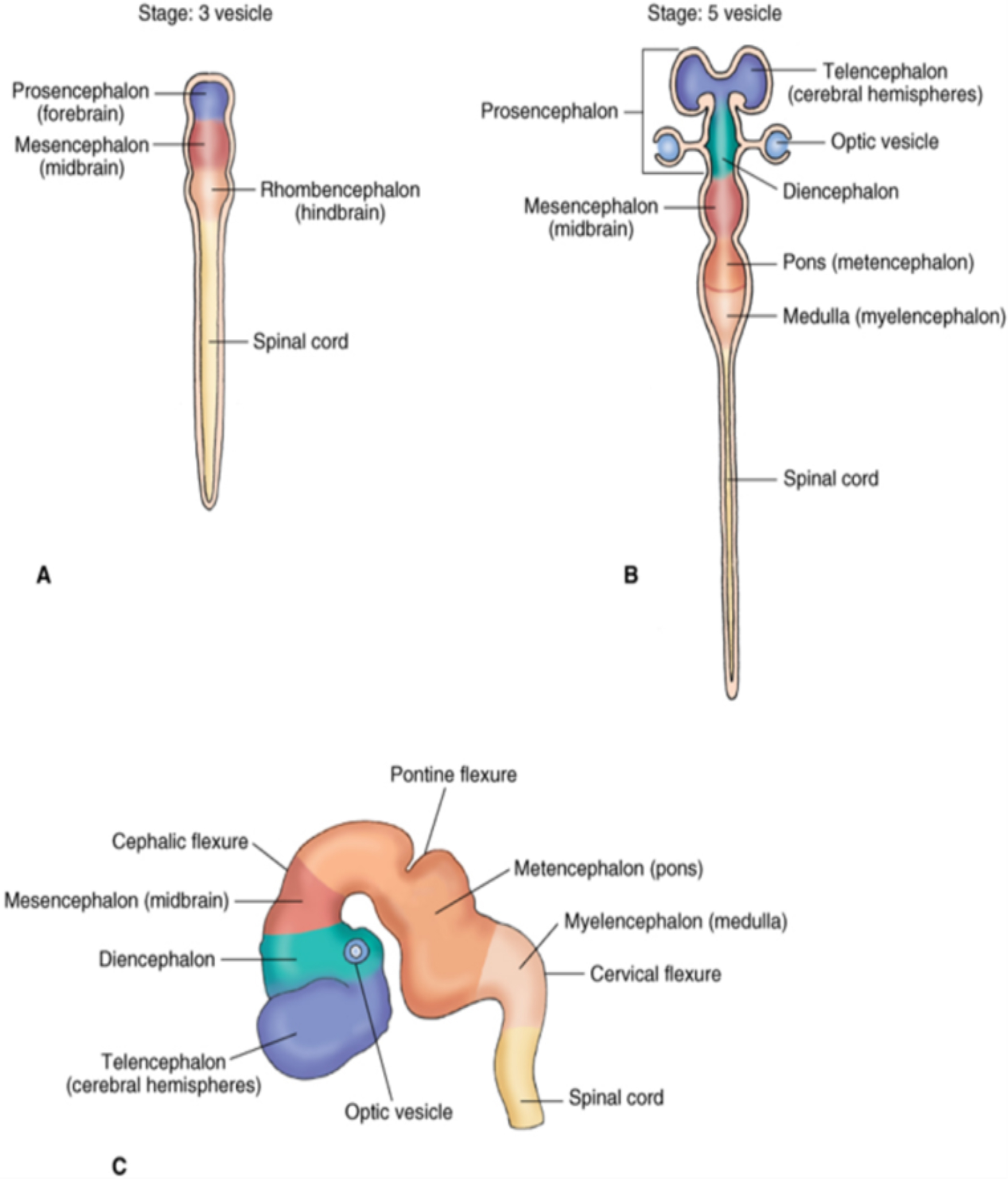
Three primary (1°) brain vesicles (Figure 1.5A) that initially form the vesicles from rostral to caudal are:
the prosencephalon (forebrain)
the mesencephalon (midbrain)
the rhombencephalon (hindbrain)
In the 1° brain vesicles stage, cephalic and cervical flexures are apparent in the rostral (anterior) portion of the neural tube.
The primary brain vesicles further subdivides into secondary (2°) brain vesicles (Figure 1.5B).
The prosencephalon subdivides into:
Telencephalon forms the cerebral hemispheres and basal ganglia. Expansion of the cerebral hemispheres (into a C-shape) after formation of the 2° brain vesicles leads to the shape of the adult cortex.
Diencephalon is a single midline structure which develops into the hypothalamus, thalamus, and pineal gland.
An optic cup develops off the diencephalon forming the retina and optic nerve.
The mesencephalon (midbrain) does not subdivide and eventually forms connections with the cerebellum.
The rhombencephalon (hindbrain) subdivides into:
Metencephalon, forming both the cerebellum and pons
The cerebellum develops from a rhombic lip of the metencephalon.
Myelencephalon, which develops into the medulla oblongata.
Note
All mammalian brains initially are lissencephalic (unfolded), but as further development occurs, the brains become gyrencephalic (folded) in humans and other mammals.
The human brain development continues until at least 20 years of age. Four main developmental stages could roughly be described as: before birth; birth to 5 years; 5 to 10 years; and 10 to 20 years. Specific developmental skills are attained by individuals at all of these stages.
2. Closure of the anterior (rostral) neuropore (~25 days).
The closure of the anterior neuropore begins in the cervical region of the spinal cord, and continues to the anterior pole of the developing prosencephalon. The early swelling of brain vesicles is due to cavitation caused by the increase in pressure; this physical force (pressure) is necessary for normal cell proliferation.
Swelling of brain vesicles occurs because of two separate but yet significant events: the first is the closing of the rostral (cranial) neuropore, and second is a transient constriction of the central canal in the caudal hindbrain. Later in development, the constricted central canal re-canalizes. If re-canalization does not occur, the pressure becomes too great, resulting in hydrocephalus.
review 1.2.
(Tap to open; use your Apple Pencil to draw.) Diagram the primary and secondary brain vesicles and correlate these structures with the adult structures that are derived from them.
3. Closure of the posterior (caudal) neuropore (~28 days).
A defect that is associated with the failure of the posterior neuropore to close is spina bifida. Grossly, spina bifida presents as the failure of the vertebral arches to fuse.
There is not one specific cause for spina bifida, nor any way to prevent it 100%. Supplementation of the maternal prenatal diet with folic acid has been shown to be helpful in preventing forms of spina bifida along with other neural tube defects.
The presence of alpha-fetoprotein (AFP) in the amniotic fluid is used as a diagnostic predictor of neural tube defects such as a spina bifida or anencephaly. Blood test can be used to detect AFP.
4. Once the normal swelling of the brain has occurred and the pressure is relieved, the cell populations associated with the brain vesicles begin proliferating.
The cavity of the 2° brain vesicles will be reduced to a series of interconnected ventricles through which cerebral spinal fluid (CSF) will flow.
Review 1.3.
The medulla in the adult is derived from what embryonic structure?
Spinal cord development
1. After neurulation, the three neuroepithelial zones are present in the caudal portion of neural tube.
These include:
the mitotically active ventricular zone,
the intermediate (mantle) zone,
and then the outer marginal zone (see Figure 1.4).
The parts of the adult spinal cord are derived from these cells:
The neuroblasts from the intermediate zone will form the “grey matter” (neuronal cell bodies) of the brain stem and spinal cord.
Axons in the marginal zone will form “white matter” (axonal fiber tracts) of the brain stem and spinal cord.
The closed neural canal becomes the central canal through which cerebrospinal fluid eventually flows.
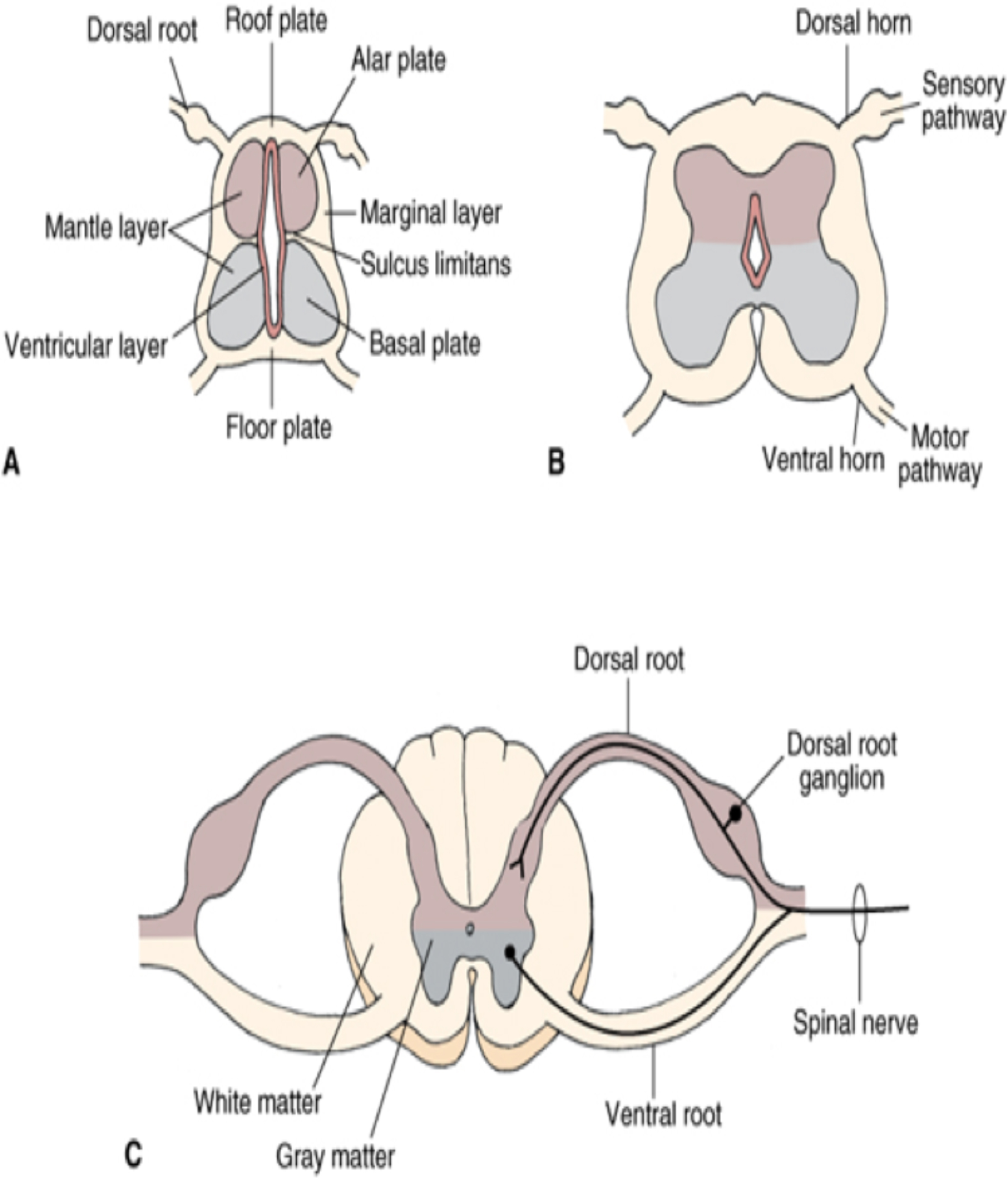
2. Differential migration of developing neurons leads to the formation of alar and basal plates.
Neurons from neuroepithelial cells located along the dorsal half of the neural tube migrate dorso-laterally, and those in the ventral half migrate ventro-laterally.
Because of these differential migrations, a longitudinal groove is formed on either side of the central canal. This groove, termed the sulcus limitans, demarcates the alar plate dorsally and the basal plate ventrally. (Figure 1.6A)
Continued migration of neuroblasts results ultimately in the butterfly shape of the gray matter.
The neuroepithelial cells in the alar plate differentiate, forming the 2nd order sensory neurons and the basal plate differentiates into motor neurons (GSE or GVE).
The dorsal (posterior) gray columns (horns) develop from the alar plates.
The intermediolateral and ventral (anterior) gray columns (horns) develop from the basal plates.
Molecular Determinants of Spinal Cord and Cerebellar Development
In the spinal cord, the populations of cells forming the basal plate are greatly influenced by the notochord. The notochord releases sonic hedgehog (SHH), which is necessary for the migration and formation of motor neurons associated basal plate.
The sonic hedgehog signaling pathway is also extremely important for the development of cerebellar granule cells.
The alar plate formation is influenced by the BMPs (bone morphogenic proteins), which are another important family of signaling molecules. BMPs are also involved in induction of neurulation and neural plate development.
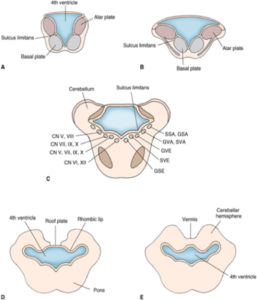
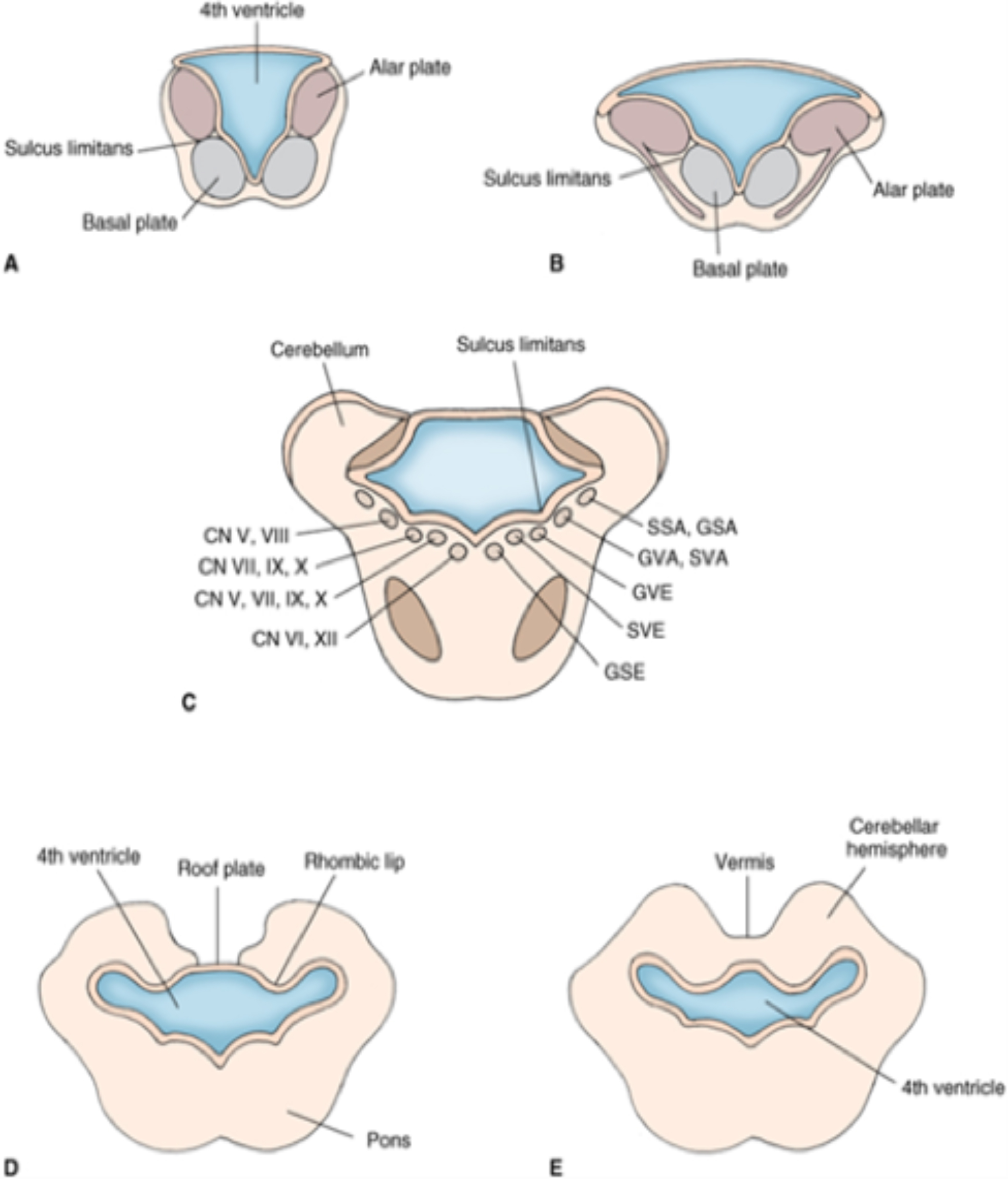
The alar and basal plates are oriented differently in the brainstem compared to the spinal cord. This difference in orientation is due to the expansion of the 4th ventricle posterior to the rhombencephalon (Figure 1.7).
A general statement, with a few exceptions, to describe the location of the cranial nerve nuclei in the brainstem is that the basal plates forming the motor nuclei are medially located, and the alar plates forming the sensory nuclei are more laterally placed.
Important
This is an important distinction to think about when you are trying to deduce where focal lesions may be located related to the adult topography of the brainstem.
Review 1.4.
Which of the following forms from the basal plate of the developing neural tube?
Anencephaly is a normally fatal congenital defect occurring when the anterior (rostral) end of the neural tube (anterior neuropore) fails to close, during the 5th week of gestation. The resulting phenotype is a fetus with an absence of major portions of the brain, skull, and scalp. Children with this disorder are usually born without the telencephalon.
Incidence rate ~11.1/ 100,000 live births
The incidence of anencephaly may be reduced by increasing folic acid during the 1st trimester of pregnancy.
In anencephaly, the brain stem remains intact. In some cases, the neural tube defect extends caudally into cervical region of vertebral column and is called a craniorachischisis.
Holoprosencephaly is caused by a failure of the embryo’s forebrain to divide and form bilateral cerebral hemispheres. It results in defects in the development of the face, as well as structural and functional forebrain deficits. This defect varies in severity from a condition of cyclopia to a fused of cerebral hemisphere with only minor craniofacial defects.
One cause of holoprosencephaly is related to the sonic hedgehog protein (SHH) and the signaling cascades that are influenced by sonic hedgehog.
Another cause of holoprosencephaly is an error in cholesterol biosynthesis.
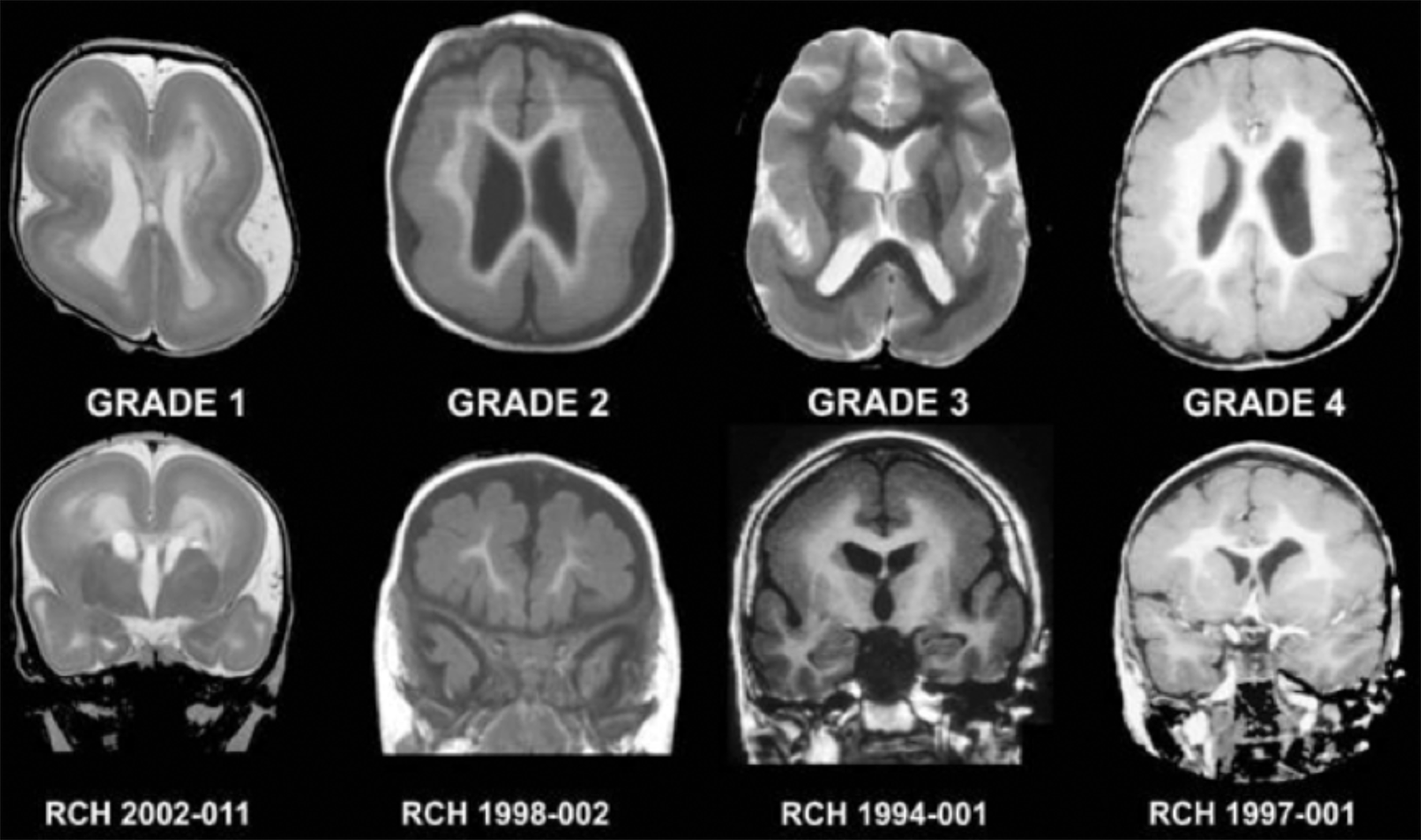
Lissencephaly is a very rare (1:100,000 births) brain malformation with a genetic (X-linked) component of inheritance. In affected individuals, the cells in the layers of the cerebral cortex do not migrate properly, which results in abnormally formed cortical layers.
Lissencephalic patients have differing degrees of developmental arrest depending upon the severity of the condition (see different grades in Figure 1.8). Also, another clinical presentation of lissencephaly is seizures; it is associated with the DCX (Doublecortin) mutation form of lissencephaly.
The phenotype of this defect is where the surface of the cerebral cortex appears smooth to differing degrees (similar to the early fetal brain). See Figure 1.8, showing different gradations of classic lissencephaly, from agyria (absence of gyri) to pachygyria (thick gyri).
Genes shown to be involved in a majority of classic lissencephalic conditions have included the LIS1 and DCX. These genes are involved in the regulation of cytoskeletal function which are associated with neuronal migration.
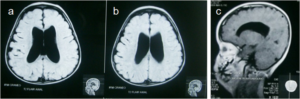
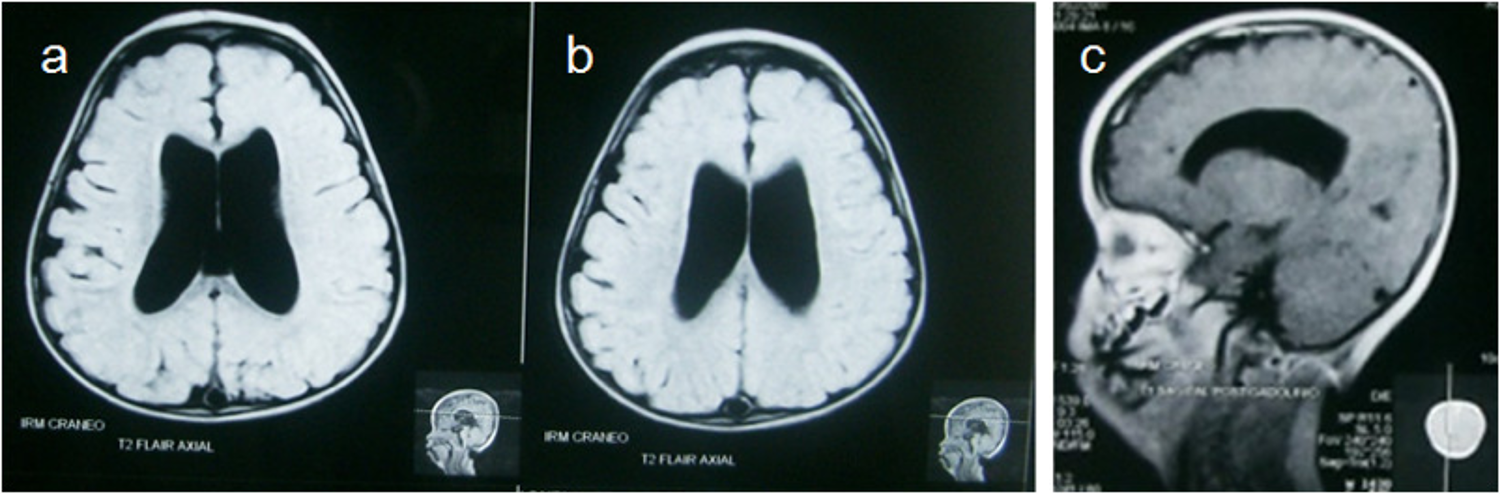
Hydrocephalus occurs in 1:500 live births, making it one of the most common congenital defects. Causes of hydrocephalus can be exposure to teratogenic agents (e.g., fetal exposure to microbes or viruses).
Figure 1.9. Congenital hydrocephalus (non-communicating). This figure shows sections through a hydrocephalic newborn brain with a genetic defect, showing enlarged lateral ventricles. Also note atrophy of the corpus callosum in C. Wikimedia.org.
There are two types of hydrocephalus: obstructive (non-communicating) or non-obstructive (communicating).
In most cases, hydrocephalus in newborns is due to an obstruction of the cerebral aqueduct. This obstruction prevents the passage of cerebrospinal fluid produced in the lateral and 3rd ventricles from passing into the 4th ventricle.
Chiari Malformation (CM) II: The cerebellar vermis and tonsils herniate with a resulting hydrocephalus. This condition often presents early in childhood and is associated with clinical signs that include difficulty swallowing, apnea, and spastic paralysis of the upper limb. There is usually an accompanying form of spina bifida, a meningomyelocele, in this type of Chiari malformation.
Chiari Malformation III and IV are very rare and involve incomplete development of the cerebellum and skull.
Thought question What symptoms would be associated with the syringomyelia resulting from a Chiari Type I malformation if the syrinx was localized to the cervical spinal cord?
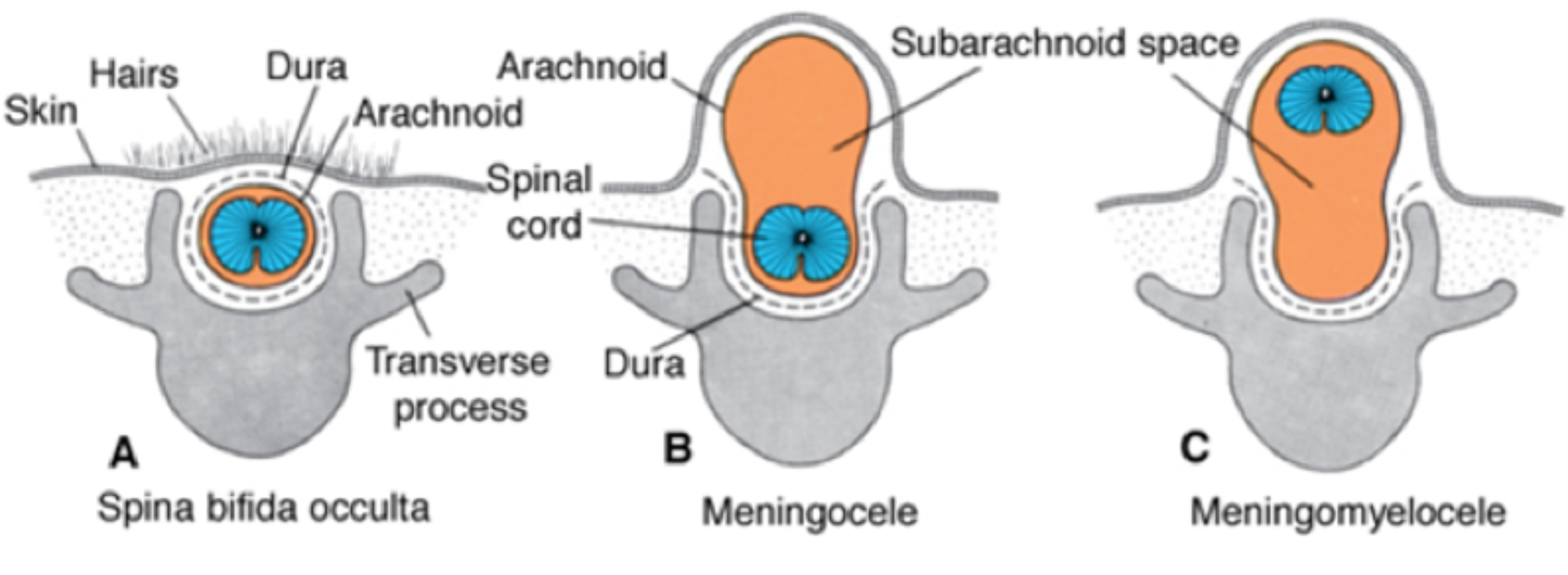
Spina bifida is a defect associated with the closure of the caudal neuropore (neural tube). Spina bifida literally means “split spine.” Grossly, it is caused by the failure of the vertebral arches to fuse and has an incidence of 1.8:1000 births.
Too much retinoic acid or not enough folic acid may be related genomic DNA methylation defects, which may cause of spina bifida and other neural tube defects.
Errors in neural crest cell migration are thought to be a potential cause of spina bifida.
One form of spina bifida is asymptomatic neurologically and presents as a tuft of hair in the lumbar region (spina bifida occulta) (Figure 1.11).
Figure 1.11. Spina bifida forms. From Central Nervous System Langman’s Medical Embryology, 13e, 2014.
More severe forms of spina bifida include a meningocele (where the meninges is exposed) and meningomyelocele where the spinal cord and nerve roots are contained within a meningeal sac on the posterior surface of the body. In this form of spina bifida, paralysis caudal (inferior) to the level herniation is common.
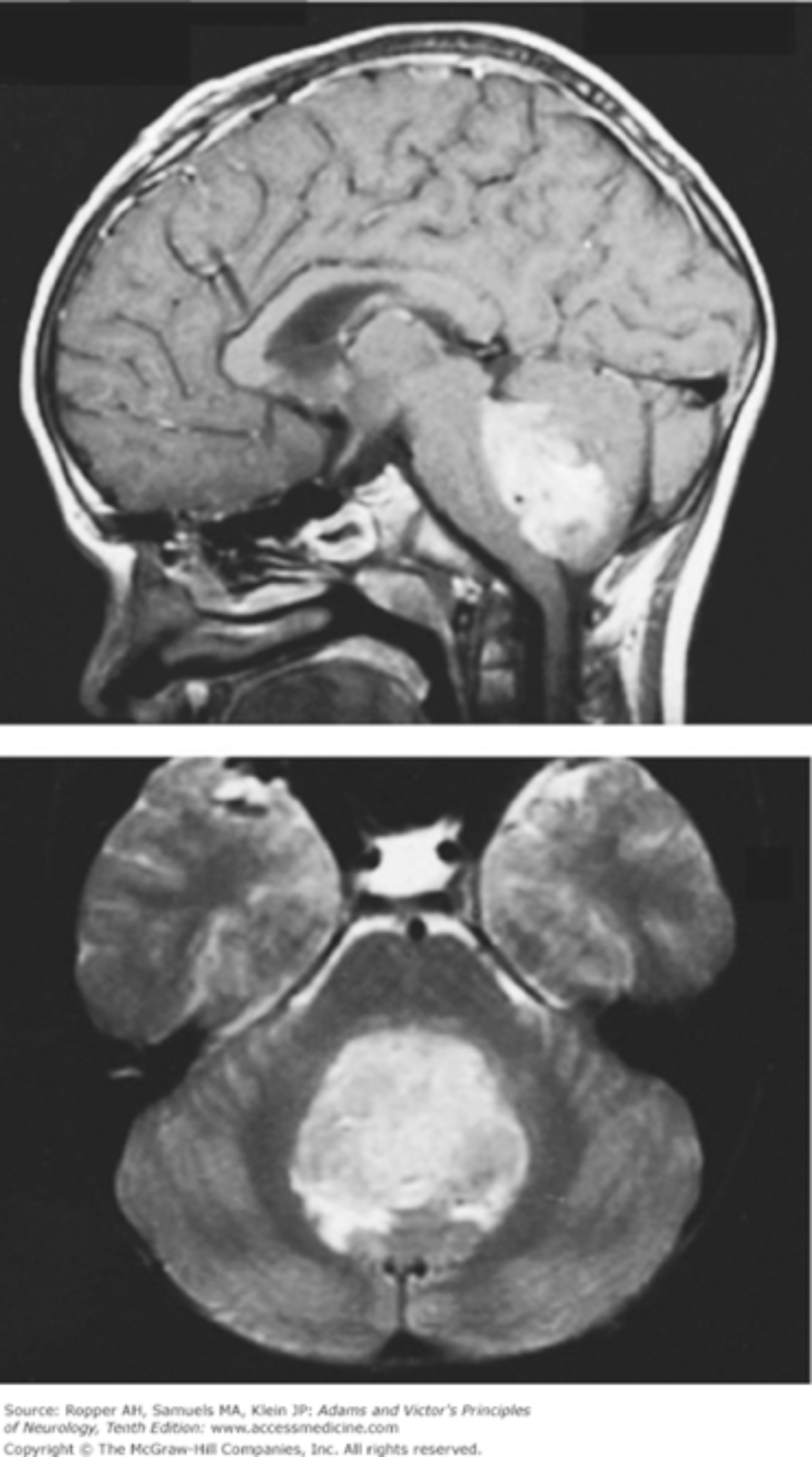
Figure 1.12. Medulloblastoma. Chapter 31. Intracranial Neoplasms and Paraneoplastic Disorders, Ropper AH, Samuels MA, Klein JP. Adams and Victor’s Principles of Neurology, 10e; 2014. Accessed July 17, 2018.Medulloblastoma is the most common malignant brain tumor in children, accounting for ~20% of brain tumors. The etiology of this defect is a neuroepithelial-derived tumor. Current research shows that this form of tumor arises for pluripotent stem cells of the cerebellum.
One cause of medulloblastoma may also be related to the SHH signaling pathway: overexpression of SHH leads to medulloblastoma in mice, and suppression of SHH leads to inhibition of medulloblastoma.
Complications from medulloblastoma may include hydrocephalus related to a blockage of CSF flow between the ventricles. As the tumor progresses, there may also be disturbances associated with gait and balance which are both related to cerebellar dysfunction. See Figure 1.12, showing the tumor occupying the entirety of the 4th ventricle, and on the transverse section note that it has compressed and obliterated the vermis of the cerebellum.
Thought question If the vermis of the cerebellum were affected, what type of signs could a child exhibit?