


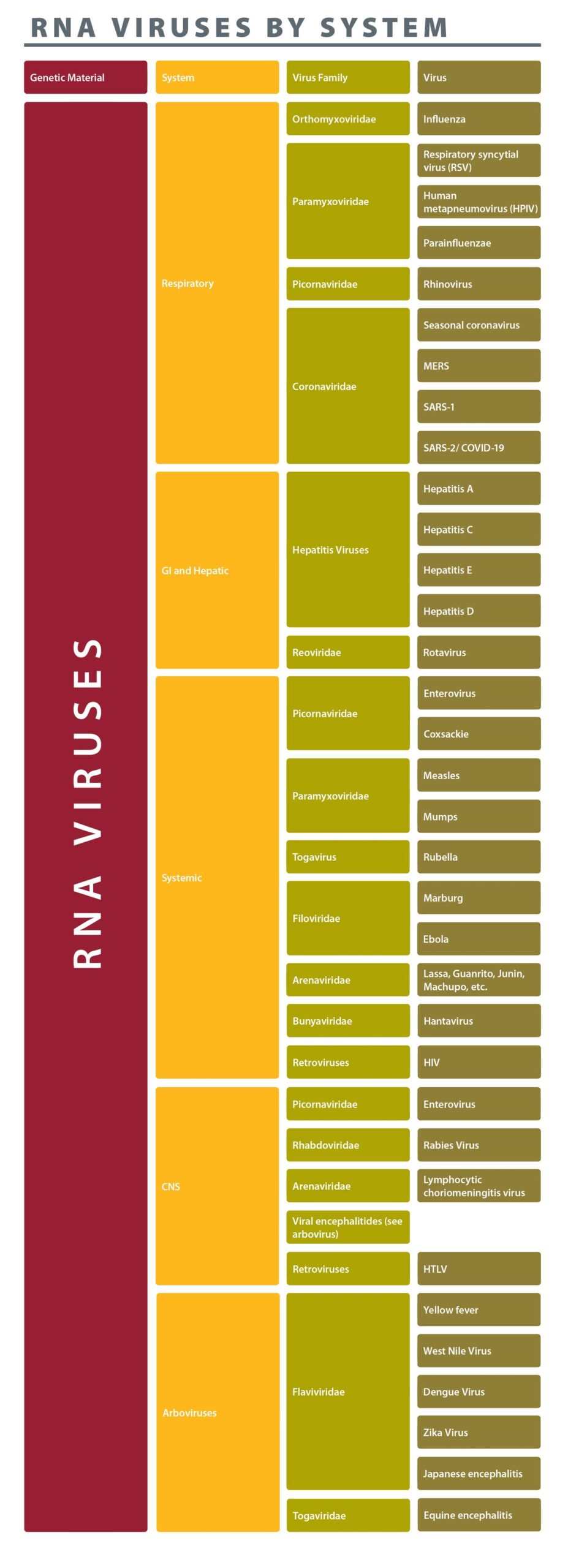
dsRNA
Rotavirus
Segmented dsRNA virus.
The segmented RNS allows for genetic reassortment and is utilized in vaccine formation. It is transmitted by fecal-oral route where its double-layered capsid resists digestion by stomach acid. Primary site of infection is duodenum and proximal jejunum where villi are destroyed, leading to decreased absorptive surface.
It is one of the most important causes of diarrheal illness in children and can cause severe disease and death due to dehydration in infants. Interestingly, newborns (0–2months) are relatively resistant to disease caused by rotavirus infection. Diagnosis is made by viral PCR of the stool during acute infection.
Treatment is supportive. A live vaccine is given to infants with 85–98% efficacy in preventing disease.
Retroviruses
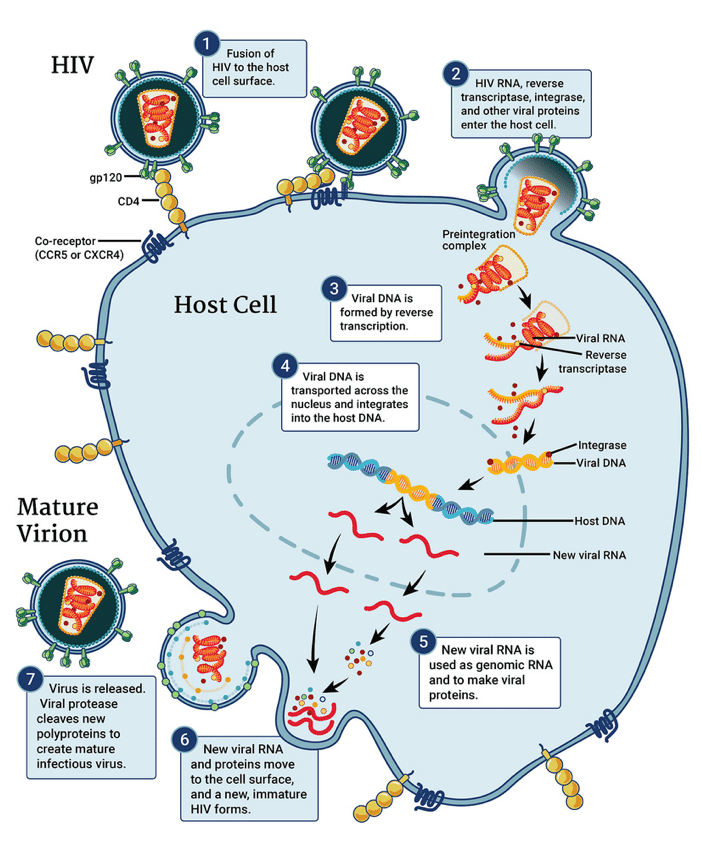
Retroviruses also uniquely carry integrase enzymes that allow insertion of proviral DNA into the host cell genome. Host cell machinery is used for transcription and translation. While there are numerous orders and families of retroviruses that have co-evolved with living organisms for millions of years, the most important retrovirus in human disease is HIV infection and HTLV infection is also worth note. The steps in viral replication are important targets for treatment of HIV virus.
Human T-lymphocytic Virus
Oncoretrovirus.
While it appears the virus has a worldwide distribution, clinical disease is rare and more commonly found in Japan, Africa, and Caribbean. HLTV-1 causes a rare adult T-cell leukemia and lymphoma that is associated with cutaneous disease (Sezary syndrome). Infection is also associated with neurologic disease known as tropical spastic paresis.
Human Immunodeficiency Virus (HIV)
Enveloped virus with diploid ssRNA genome.
The virus requires 2 receptors to enter a cell:
-
- The CD4 protein
- A co-receptor (CCR5 or CXCR4 depending on the tropism of the virus).
While CD4 lymphocytes are the most abundant viral target, and their depletion is the primary mode of disease, a plethora of other cells have available receptors, including astrocytes, macrophages, and cells in the reproductive tract and colon. HIV is transmitted through blood and body fluids (sex, blood products, shared needles, transplacentally, peri-natal, breast milk).
After initial infection, the virus establishes widespread infection throughout hematopoietic system. Acute retroviral infection may be asymptomatic, but may also cause symptoms of acute viral syndrome with fevers, pharyngitis, lymphadenopathy, and a rash. It then remains clinically quiescent for several years. If untreated, CD4 depletion occurs leading to defects in cell-mediated immunity as well as dysfunction of adaptive immunity. Opportunistic infections are myriad and are the primary cause of death.
Current diagnosis of HIV infection uses serologic testing for antibodies to HIV as well as the presence of p24 antigen. Confirmation is with PCR to detect viral RNA in the blood. In established infections, the viral load is used to monitor therapy. The goal of therapy is a sustained undetectable viral load.
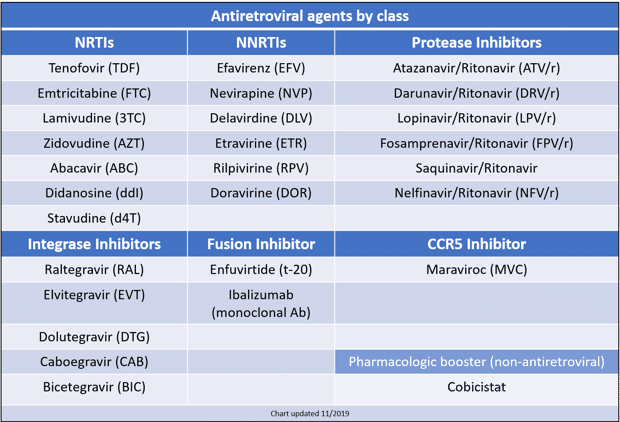
Treatment of HIV infection requires multiple anti-retroviral (ARV) agents with different mechanisms of activity to avoid rapid adaptation of the virus through mutations. There are six main classes of ARVs:
-
- Nucleot/side reverse transcriptase inhibitors (NRTIs)
- Non-nucleotide reverse transcriptase inhibitors (NNRTIs)
- Integrase strand transfer inhibitors (INSTIs)
- Protease inhibitors (PIs)
- Co-receptor CCR5 inhibitor
- Fusion inhibitors
Most common regimens involve a backbone of 2 NRTIs, plus one agent from INSTI, PI, or NNRTI. CCR5 inhibitors and fusion inhibitors are used as salvage therapy.
Patients with HIV and AIDS can develop disease in nearly every organ system, and the differential diagnosis for any chief complaint in persons with immunodeficiency is much more broad compared to those with intact immunity. In the case of HIV infection, in addition to common and unusual opportunistic infection, clinical disease can arise from direct effect of the virus itself and importantly, side effects and complications of disease treatment must also be considered. It is helpful to think about the types of infections and conditions that present primarily in certain systems.
Opportunistic infections/HIV manifestations by system
-
Pulmonary
Opportunistic infections
- TB
- Pneumocystis jirovecii
- Recurrent bacterial pneumonias: Typical and atypical
- Non-TB mycobacterium (rapid growers)
- Endemic fungi
- Cryptococcus
- Nocardia
- Aspergillus
- CMV
HIV-related disorders
- Pulmonary hypertension
- Lymphocytic interstitial pneumonia (peds)
Neoplasms
- Kaposi sarcoma (HHV8)
- Primary effusion lymphoma (HHV8)
- Lung cancer
-
Ophthalmic
Opportunistic infections
- CMV
- Toxoplasmosis
- VZV ophthalmicus and retinopathy
- HSV keratitis and acute outer retinal necrosis
- Syphilis uveitis
- TB uveitis
- Candida endophthalmitis and keratitis
- Cryptococcus chorioretinitis
- Pneumocystis choroiditis (rare)
HIV-related disorders
- HIV retinitis
Neoplasms
- Kaposi sarcoma (HHV8)*
*AIDS-defining malignancy
-
Neurologic
Opportunistic infections
- TB: Meningitis
- Toxoplasmosis
- Cryptococcus: Meningitis (cryptococcoma, rare)
- HSV/VZV
- CMV
- JC virus: Progressive multifocal leukoencephalopathy
- Bacterial meningitis
- Neurosyphilis
- Nocardia
- Caccidioidomycosis
HIV-related disorders
- HIV-associated neurocognitive disorder (HAND): Dementia
- Polyneuropathy
- Mononeuritis multiplex
- Aseptic meningitis
Neoplasms
- Primary CNS lymphoma (EBV)
Medications
-
NRTIs: Peripheral neuropathies
- EFV: Psychiatric symptoms
-
Heme-Onc
Opportunistic infections
- Bone marrow infections
- Mycobacterium avium complex
- Parvovirus B19
- Endemic fungi (histoplasmosis, coccidioidmycosis, blastomycosis)
- Cryptococcus
- Tuberculosis
- Anemia of chronic disease (any systemic infection)
HIV-related disorders
- Persistent generalized lymphadenopathy
- Immune thrombocytopenic purpura (ITP)
- Thrombotic thrombocytopenic purpura (TTP)
Neoplasms
- Kaposi sarcoma (HHV8)
- Non-Hodgkin lymphoma (EBV)
- Invasive cervical cancer
- Hodgkin lymphoma (11 increased risk)
- Hepatocellular carcinoma (HBV, HCV) (5 increased risk)
- Anorectal squamous cell Ca (HPV 16, 18) (29 increased risk)
Medications
-
AZT: Anemia
-
Digestive
Opportunistic infections
- TB
- Candida (thrush)
- Oral hairy leukoplakia (EBV-related)
- HSV stomatitis
- CMV
- Enteric bacterial infection: Shigella, salmonella, campylobacter
- Mycobacterium avium complex
- Histoplasmosis
- Crytosporidium, cyclospora, microsporidium
- Anorectal warts
- Hepatobiliary
- Chronic hepatitis (HBV, HCV)
- Infectious cholangiopathy: MAC, cryptosporidium
HIV-related disorders
- Chronic diarrhea/AIDS enteropathy
- HIV cholangiotherapy
Neoplasms
- Kaposi sarcoma (HHV8)
- Non-Hodgkin lymphoma (EBV)
- Hepatocellular carcinoa (HBV, HCV)
- Anorectal squamous cell Ca (HPV 16, 18)
Medications
-
Most of them! Protease inhibitors most commonly implicated.
-
Dermatologic
Opportunistic infections
-
Bacillary angiomatosis (KS mimic): Bartonella
- Staph aureus SSTIs
- HSV
- VZV
- Secondary syphilis
- Crusted scabies
- Molluscum contagiosum
- Warts
- Adverse drug reactions
HIV-related disorders
- Pruritic popular eruption (tropics)
- Seborrheic dermatitis
- Xerosis (dry skin)
- Psoriasis
- Eosinophilic folliculitis
Neoplasms
- Kaposi Sarcoma (HHV8)
- Basal cell carcinomas
- Squamous cell carcinoma
Medications
-
Drug rash: NNRTIs, Darunvir (sulfa-moiety)
-
Renal
Opportunistic infections
-
Acute renal failure
- Systemic infections, sepsis
- Medication to treat infections
HIV-related disorders
- HIV-associated nephropathy (HIVAN)
-
Collapsing focal segmental glomerular sclerosis
-
Medications
-
Tenofovir: Renal proximal tubular acidosis (Fanconi syndrome)
- TMP-SMX: Nephtotoxic in high doses
-
Cardiac
Opportunistic infections
-
Pericarditis: TB, viral, bacterial, primary effusion lymphoma (HHV8)
HIV-related disorders
- Dilated cardiomyopathy
-
Early coronary artery disease
Neoplasms
- Kaposi sarcoma (HHV8)
Medications
-
? Cardiovascular disease with NRTI exposure
-
Endocrine/Metabolic
Opportunistic infections
-
Adrenal failure
- TB (most common)
- CMV, cryptococcus
HIV-related disorders
-
Hypogonadism
- Low testosterone
Medications
- Lactic acidosis: NRTIs
- Dyslipidemia: Protease inhibitors
-
Rheumatologic and Musculoskeletal
Opportunistic infections
-
Pyomyositis: S. aureus
-
TB: Osteomyelitis, arthritis
HIV-related disorders
-
Sjogren’s-like syndromes (Diffuse infiltrative lymphocytosis [DILS])
-
Polymyositis
-
Osteonecrosis/avascular necrosis of the hip
Medications
-
AZT: Myopathy
-
Tenofovir (TDF): Decreased bone density
ssRNA
Respiratory
Enveloped segmented ssRNA virus.
There are three types, A, B, and C. Segmented genome allows for reassortment between viruses that infect different mammals this is called antigenic shift and accounts for major epidemics- Influenza A is the only type capable of this as others are restricted to humans only. Mutations in RNA segments leads to antigenic drift and accounts for the seasonal variations. Two important antigens are Hemagglutinin (HA) and Neuraminidase (NM) that facilitate viral attachment to respiratory epithelium and release of new particles respectively.
Transmission of influenza is by respiratory droplets. Clinical disease is characterized by abrupt onset of fevers, chills, myalgias and cough. Severe disease can in the very young, elderly, immunocompromised, co-morbid cardiac or pulmonary disease, and pregnant females. Severe disease includes viral pneumonia, respiratory distress, and multi-organ failure – most of which is mediated by a dysregulated immunopathologic response.
Diagnosis in symptomatic persons is PCR from nasopharyngeal swab.
Primary treatment is neuraminidase inhibitors, though their efficacy in treating severe disease is relatively limited.
Several vaccination options are available and are adjusted seasonally to reflect circulating strains while aiming to maintain immunogenicity.
Enveloped ssRNA virus in the same family as influenza. Unlike influenza, the antigenicity of hemagglutinin and neuraminidase is stable.
There are four sub-types. Transmission is via respiratory droplets and is a common infection in children.
Clinical infection causes fever and cough. In young children, parainfluenza is the most common cause of croup, which is characterized by a barking cough that is frequently worse at night. In infants, parainfluenza can cause bronchiolitis and respiratory distress similar to RSV. In adults, infection is generally limited to symptoms of the common cold.
Treatment is supportive.
Enveloped ssRNA virus that is transmitted via respiratory droplets.
Unlike other paramyxoviridae, RSV does not have hemagglutinin. Instead a fusion protein facilitates attachment and accounts for the cytopathologic features of fused cells that form multinucleated giant cells. There are two serotypes.
It is the most important cause of bronchiolitis and pneumonia in the first year of life. Sloughing of respiratory epithelial cells in the tiny airways of the infant lung leads to air-trapping, wheezing, and respiratory distress. In older children, RSV is a common cause of otitis media. Diagnosis is made by PCR of respiratory secretions. Therapy is mostly supportive, and aerosolized ribavirin is used for severely ill.
Naked ssRNA virus that is transmitted by aerosolized droplets and hand-to-nose contact.
Infection is limited to the respiratory epithelium. And since virus replicates best at cooler temperatures, lower respiratory infections do not occur. There are over 100 serotypes.
Clinical disease is the common cold: rhinorrhea, congestion, pharyngitis.
Enveloped ssRNA virus with 2 serotypes. Transmission is via respiratory droplets and immunity is not sustained, so reinfection can occur.
Most common clinical disease is simple common cold. Novel mutants have been associated with outbreaks and severe disease (e.g., SARS and MERS). These are frequently zoonotic in origin; viral mutation allows the ‘jump’ to humans and limited immunity facilitates outbreaks.
Enveloped ssRNA virus that is transmitted via respiratory droplets.
Similar to RSV, a fusion protein on the envelope facilitates attachment and creates fused multinucleated giant cells.
Most common clinical disease is the common cold. In infants, bronchiolitis similar to RSV is possible, and viral pneumonia in immunocompromised patients is a risk.
Diagnosis is by PCR of respiratory secretions. Treatment is supportive.
GI/Liver
See dsRNA viruses above.
Nonenveloped ssRNA virus and part of calcivirus family.
In contrast to the respiratory viruses of similar structure, norovirus is resistant to destruction by stomach acid. Transmission is fecal–oral route. There are many serotypes, and immunity is brief.
Norovirus is the most common viral cause of acute diarrheal gastroenteritis. The virus is highly infectious and outbreaks are common, especially among families or closed settings (cruise ships, hospitals, schools, etc.).
Treatment is supportive. There is no vaccine available.
Naked ssRNA virus with single serotype.
Transmission is fecal–oral. The virus replicates in GI tract, then spreads to liver during brief viremic phase. Replication within hepatocytes incites immune response, which leads to fevers, immune mediated cellular injury, and jaundice. Infection is generally self-limited, and viral clearance occurs with subsequent immunity (no chronicity). Diagnosis is made based on serology.
Treatment is supportive. Vaccination is recommended for those at risk. Hepatitis A immune globulin is available and may mitigate disease when given after exposure in a non-immune person.
Enveloped virus with single piece of ssRNA that is part of flavivirus family.
There are multiple serotypes. It is transmitted primarily through blood; sexual and perinatal infection is also possible, though less common route. It is the most prevalent blood-borne pathogen in the United States.
The natural history is dependent on age of infection and is the opposite of that seen for hepatitis B. Acute infection in children is more often symptomatic and progression to chronic infection is the exception. In contrast, adult infections (most common in the United States) are usually asymptomatic and progression to chronic infection occurs in 80–90%. Chronic hepatitis C leads to progressive hepatocellular injury and cirrhosis. The chronic inflammatory state in cirrhosis is linked to increased risks of hepatocellular carcinoma (in contrast to hepatitis B which is has direct oncogenic transformation potential).
Diagnosis begins with screening IgG antibody and confirmatory RNA PCR for those with positive results.
There is no vaccine for HCV. Treatment of hepatitis C has greatly simplified in the last 10 years. Interferon is rarely, if ever, used anymore, though it may have a role for patients with confirmed acute HCV. Direct acting antivirals that inhibit viral enzymes include NS5A, NS5B (polymerase), and viral protease. Combination therapy is highly successful at achieving cure.
Defective virus with one piece of ssRNA.
It is transmitted through blood and body fluids. HDV requires Hepatitis B protein coat. It can only replicate in cells that are infected with Hepatitis B and chronic carrier state can occur.
HDV is an important risk in persons with chronic HBV infection, where it can cause flare or decompensation of liver disease during acute infection with HDV. There is no specific treatment for HDV, but immunization and prevention of HBV infection reduces HDV infection as well.
RNA virus that is similar to HAV in many ways: transmission is fecal-oral, and infection is limited/no chronic carrier state exists. HEV is more common in low–middle income countries where outbreaks can occur. Acute infection is usually mild, and symptoms are due to immune response during viral clearance.
Also an arbovirus; is enveloped with ssRNA that is part of flavivirus family.
It is geographically distributed in tropical areas through Caribbean, central America, and central zone of Africa. It is spread by Aedes aegypti mosquito and is a threat to southwestern United States where that mosquito is endemic. Clinical infection is often asymptomatic but can cause abrupt onset fevers, chills, myalgias, and hepatocellular injury leading to jaundice. Multiorgan failure and bleeding diasthesis can occur in severe disease and associated with up to 50% mortality. There is generally no long-term sequelae for those that recover. Treatment is supportive. A live virus vaccine is available and recommended for travelers to endemic areas.
See also in the Micro-ID session guide
Rashes/Systemic
Enveloped ssRNA virus with single serotype.
It is spread via respiratory droplets, where it initially infects respiratory epithelium, then spreads to local lymph nodes and then disseminates in the blood. Measles is one of the most contagious viruses among humans and was a common childhood infection prior to vaccination campaigns.
Initial symptoms of measles are cough, coryza, and conjunctivitis with fever. Koplik spots can be seen on buccal mucosa in first day or two of illness. As the fever resolved, a diffuse maculopapular rash erupts that spreads from head and neck downward. Severe complications can develop during initial infection and include pneumonia, encephalitis, meningitis, sinusitis, and bleeding disorders. Infants, immunosuppressed, and malnourished persons are at greatest risk of severe infection. Infection with measles specifically downregulates IL-12 and cell-mediated immunity, and secondary opportunistic infections with bacteria, fungi, or mycobacteria contributes to the high morbidity/mortality of measles worldwide. Late immunologic sequelae such as blindness or subacute sclerosing panencephalitis are rare but untreatable, irreversible, and devastating.
Diagnosis of measles requires high index of suspicion; PCR of pharyngeal swab is preferred during acute symptoms. There is no specific treatment for measles. Vaccination with live attenuated vaccine is highly effective at preventing infection.
Enveloped ssRNA virus with single serotype and member of the Togavirus family.
It is transmitted via respiratory droplets and transplacentally from mother to fetus. Similar to measles, after respiratory transmission, the virus replicates in nasopharynx, spreads to local lymph nodes, then disseminates through bloodstream. Symptoms are generally mild with fever, rash, and arthralgia (overall arthritis can be seen). Severe sequelae are uncommon.
The serious risk with Rubella is congenital syndromes. When transmitted to a fetus early in pregnancy, it can cause severe malformations:
-
- Cardiac and ocular defects
- Deafness
- Microcephaly
- Hepatosplenomegaly
- Thrombocytopenia
There is no specific treatment. Live attenuated vaccine is highly effective.
Member of the Enteroviruses and is naked ssRNA virus.
There are multiple serotypes. It is transmitted via fecal–oral route where it replicates within GI tract, crossing into bloodstream where it disseminates. Acute febrile syndrome can occur. Coxsackie viruses can cause several different clinical syndromes and most closely associated with:
-
- Herpangina
- Hand, Foot and Mouth disease
- Myocarditis
- Pericarditis
- Aseptic meningitis
Treatment is supportive. There is no vaccine.
Flavivirus with 4 serotypes (DEN 1–4) with widespread geographic distribution in tropical climates across the world.
It is transmitted through Aedes aegypti mosquito. Symptoms of Dengue fever are characterized by high fever, severe headache, retroorbital pain, myalgias, and bone pain. Progressive disease can occur leading to capillary leak syndrome and shock with bleeding diathesis, Dengue hemorrhagic fever. Children are at higher risk of severe disease. Immunity is life-long, but serotype specific. Subsequent infection with different serotype is risk for severe disease, due to antibody-dependent enhancement.
Treatment is supportive. Dengue vaccine is actively sought among researchers.
Enveloped ssRNA filamentous and pleomorphic filoviruses.
Both cause highly fatal hemorrhagic fevers with rapid viral replication in vascular endothelial cells and profound suppression of normal immune responses. They are zoonotic with animal reservoir in mammals such as monkeys and bats. Geographically, they have been found mostly in the African continent. Major outbreaks of Ebola have occurred in Africa with mortality rates of nearly 50%. Transmission mechanisms from animals are incompletely understood. Transmission between humans is through blood and bodily fluids.
Treatment is supportive. The 2015 outbreak in West Africa stimulated aggressive and fast-tracked research for Ebola vaccine and treatments.
Central Nervous System
Bullet-shaped enveloped ssRNA virus.
Zoonotic transmission to humans occurs from the bite of an infected animal (urban cycle = unimmunized dogs/cats; sylvatic cycle = bats, skunks, raccoons). The viral receptor is Acetylcholine receptor. After transmission, the virus replicates locally in muscle tissue, then enters the peripheral nerves, then is transported retrograde up axon to the CNS, where viral replication rapidly occurs in the grey matter, where it causes encephalitis. Anterograde transportation takes virus to salivary glands, adrenals, kidneys, and other organs.
Clinically, rabies has a prolonged incubation period (up to 90 days), followed by a prodromal stage with nonspecific flu-like symptoms. The acute neurologic stage presents with acute encephalitis, often with agitated state including hallucinations, hyperactivity, aggression, and hydrophobia that results from difficulty swallowing and diaphragmatic spasm after drinking water—leading to the classic description of “foaming at the mouth.” Symptoms progress to coma and death in over 90%. There is no specific antiviral treatment. Rabies vaccination and immunoglobulin is given after a suspicious bite in effort to prevent viral infection of the CNS. There have been no deaths in the United States when post-exposure prophylaxis was given promptly after exposure.
Picornaviruses, naked capsid with ssRNA.
The group includes coxsackie viruses and polioviruses. Unlike rhinoviruses that are also picornaviruses, enteroviruses are resistant to the acidic pH of the stomach and transmission in humans is fecal–oral. Disease outbreaks are more common where hygiene may be sub-optimal or more frequent chances for exposure: among young children, daycares or long-term-care facilities, crowded households, or other group-living. There is seasonal variation with dominant epidemic strains that come and go and are responsible for particular outbreaks. After replication in respiratory or GI mucosa, viruses are capable of widespread dissemination. Clinical disease depends on viral tropism, but may include disease in the CNS, heart, synovial tissues, skin, mucous membranes.
Enteroviruses are the most common cause of viral (aseptic) meningitis that tends to occur in summer or fall. Symptoms include abrupt onset of headache, fever, photophobia, and meningismus. Clinical disease is generally mild compared to other forms of meningitis, and long-term sequelae is very uncommon.
Transmitted to humans through arthropods and have tropism for the CNS and come from a variety of viral families.
All CNS arboviruses maintain a sylvatic life cycle that includes non-human vertebrates, which may serve as reservoirs or blind end hosts. Humans are incidental hosts.
Notable CNS Arboviruses include:
-
- St. Louis encephalitis
- Eastern and Western equine encephalitis
- California encephalitis
- Japanese encephalitis
- LaCrosse virus
They are all spread via mosquitos (differing species) and geographically distributed according to their names. All cause a febrile syndrome with variable degrees of encephalitis.
West Nile virus is notable for broad distribution across the northern hemisphere. It is spread by mosquito virus, with birds as the principle host. It can be transmitted by bodily fluids during viremic phase. There are three clinical outcomes of infection:
-
- Asymptomatic
- West Nile fever (self-limited febrile illness)
- Neuroinvasive disease
Neuroinvasive disease can manifest as meningitis, encephalitis, or a combination of both. Certain neurologic manifestations of interest are described: Asymmetric flaccid paralysis, Tremor, Myoclonus, and Parkinsonism symptoms distinguish neuroinvasive WNV from other CNS arboviruses.