


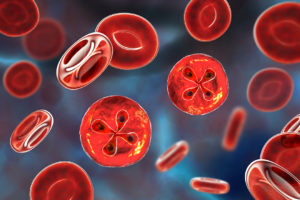
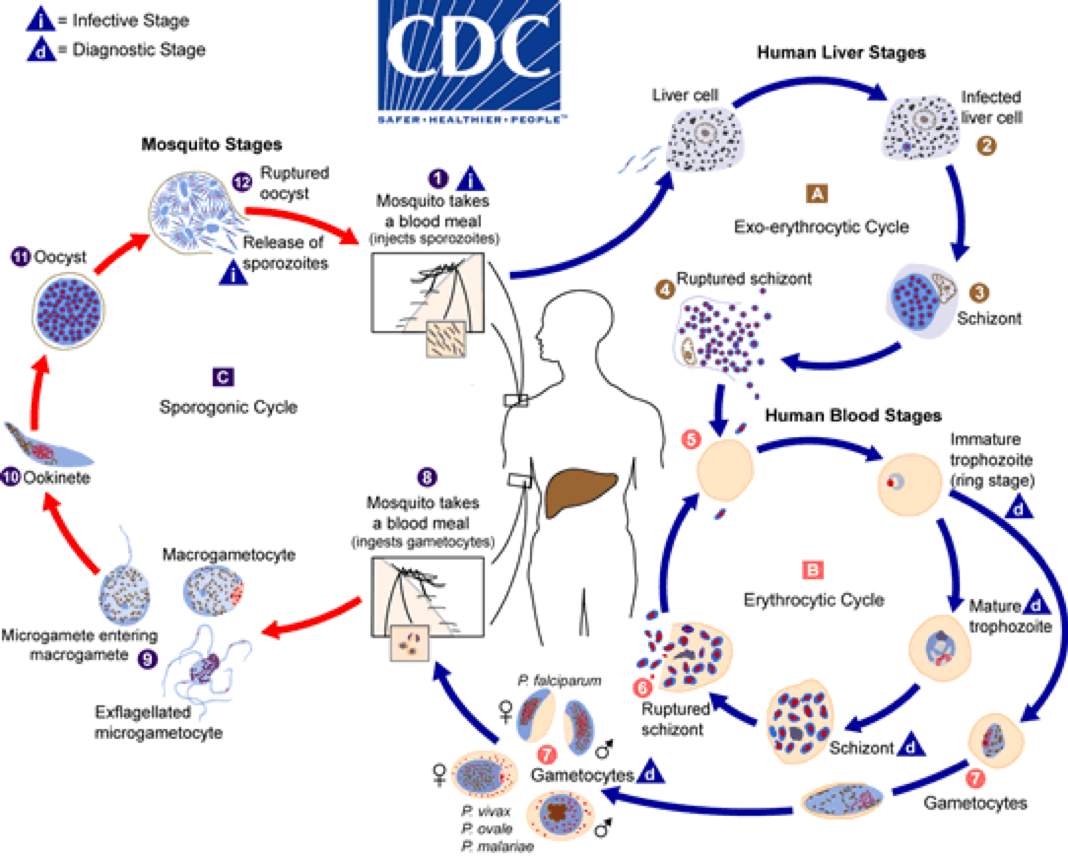
Causes most fatal cases, cerebral malaria; parasites inside RBCs cause hemolysis.
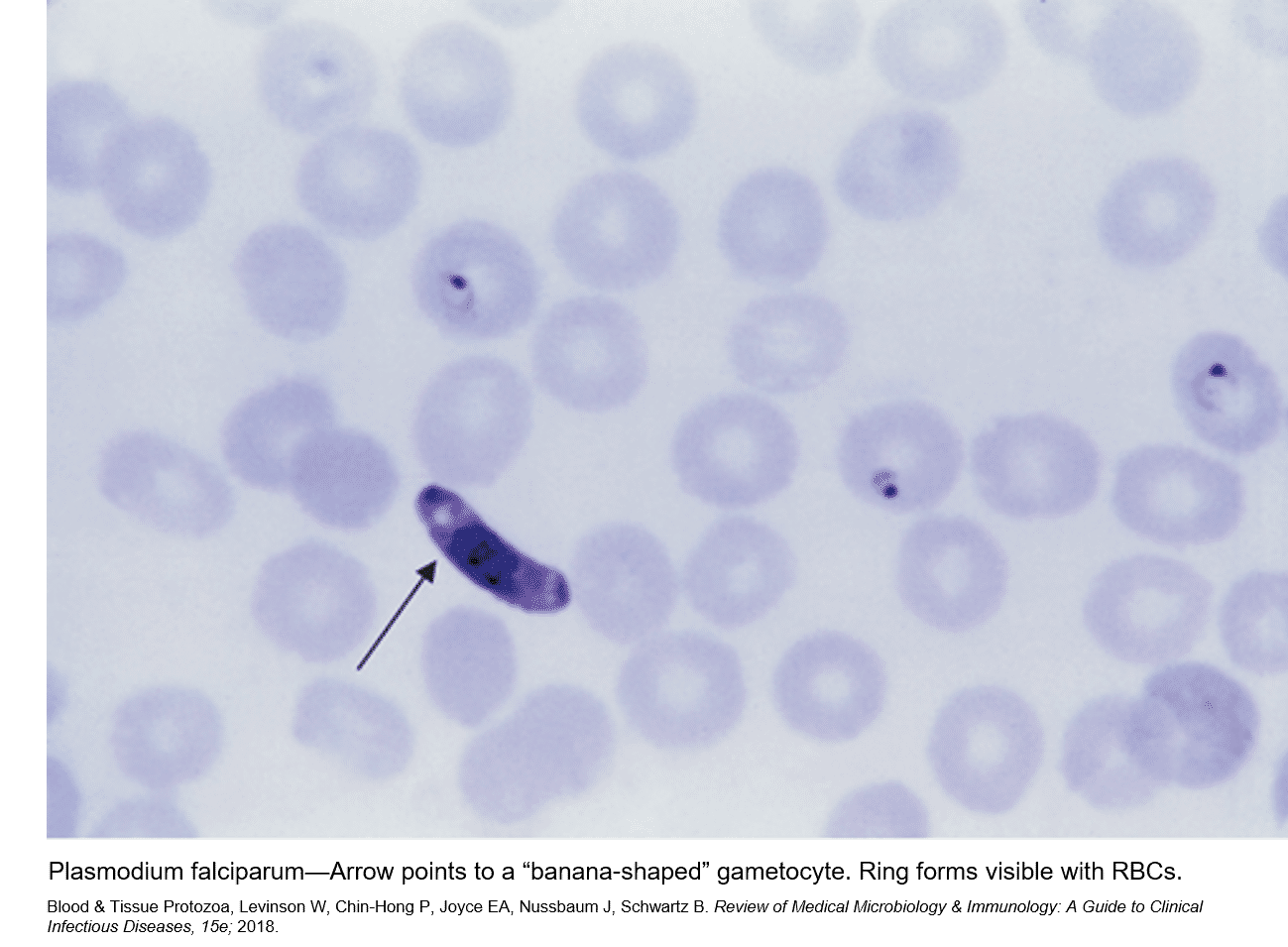
Banana gametocytes. Increased resistance to chloroquine and other antiparasitic drugs except in Central America and Caribbean areas (such as Haiti). No hepatic latent stage, so no relapsing form.
Prevention with atovaquone-proguanil (expensive), mefloquine (side effects psychiatric and cardiac), or doxycycline.
Therapy with artemether combination drugs (e.g., artemether-lumefantrine), especially for severe malaria. Other options atovaquone-proguanil, quinine, mefloquine. Chloroquine rarely appropriate.
Relapsing forms due to hypnozoites in the liver.
P. vivax infects younger RBCs (larger size). P. ovale is only in West Africa.
Erythrocyte stage is usually sensitive to chloroquine, but liver stage for these two species requires primaquine Rx after treatment of the erythrocytic stage. Check for G6PD deficiency, especially before using primaquine.
Infects older RBCs (smaller size).
Malaria variant seen in South Pacific region (from monkeys).

See also in the Micro-ID compendium