


- Fecal-oral spread of cysts.
- Resource-limited areas (i.e., Mexico, Africa, India, Central and South America).
- Male-male sex (Japan, Taiwan).
- Bloody or mucous diarrhea.
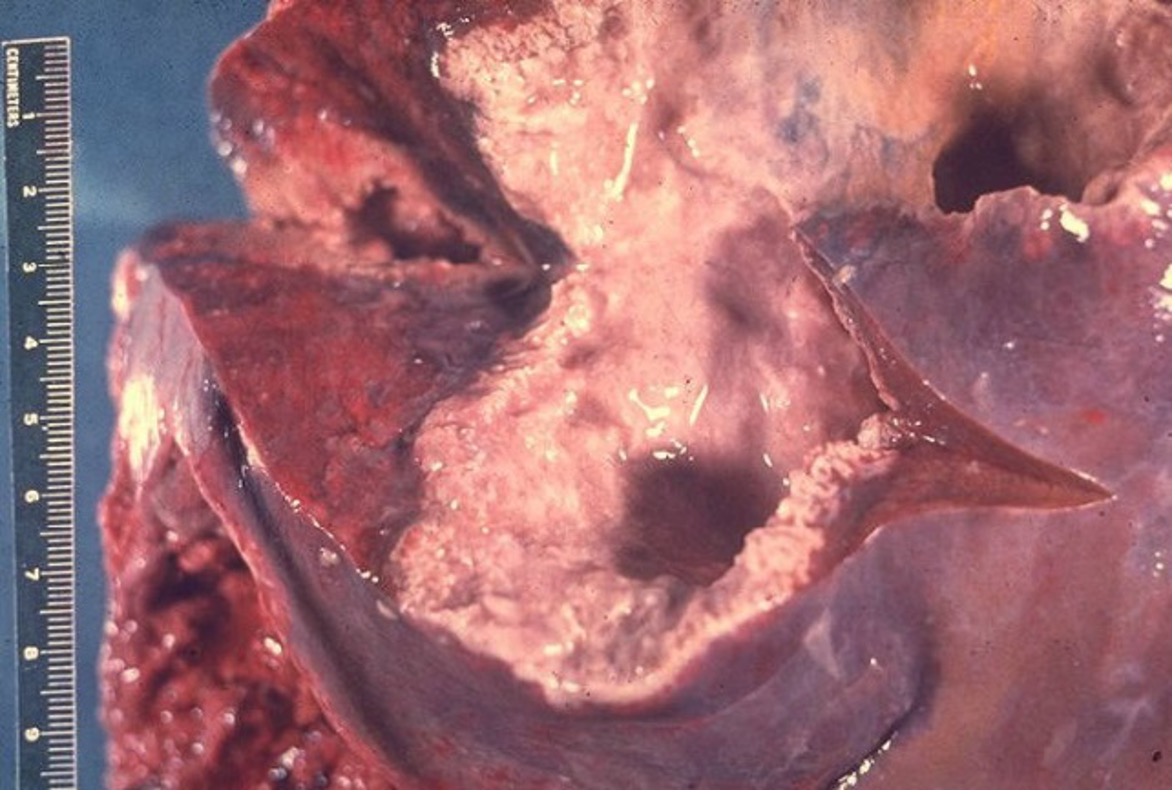
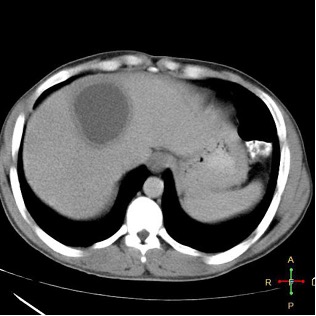
- Liver abscess in some cases.
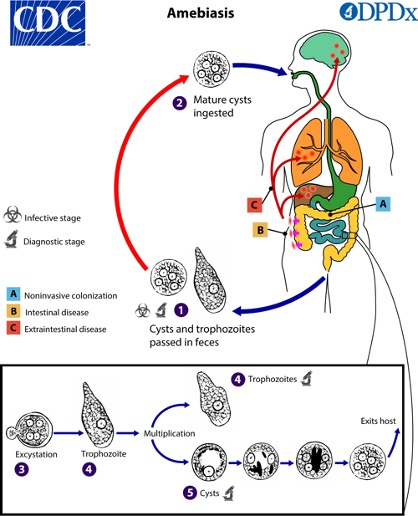
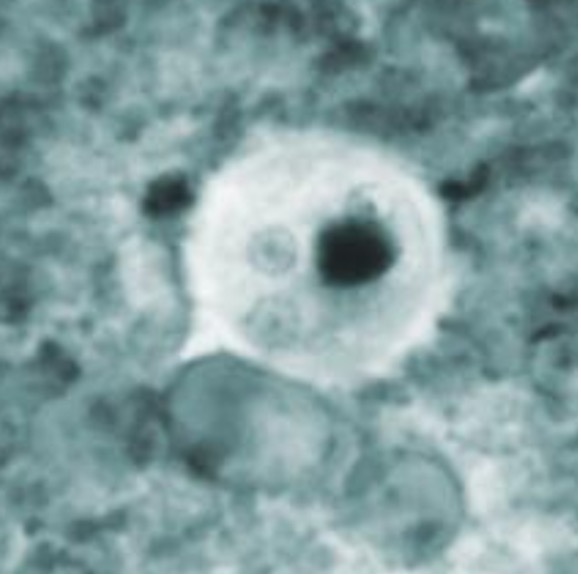

- Cysts are the infectious form.
- Note: Various non-pathogenic mimics: E. dispar, E. coli.
- Dysentery:
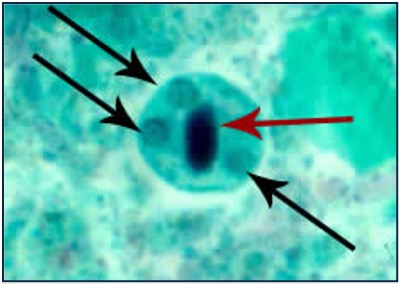
- O&P (trophozoites with ingested RBCs).
- Stool Ag.
- PCR.
- Colonoscopy.

- Liver abscess: Ultrasound or CT imaging plus serology (99% sensitive).
Metronidazole followed by paromomycin (or other GI intraluminal agent).