


Transmission to humans
- Ingestion of infected or contaminated food/water.
- Oocysts in soil from cat feces.
- Raw/undercooked meat.
- Transplacental.
- Blood transfusion or organ transplantation.
Tissue cysts remain latent in tissue.
- Can reactivate during immunosuppression.
Adapted from RWJF Slides on Medically Important Protozoa. The predominant mode of transmission for Toxoplasma varies by region. For instance, in France raw/undercooked meat is the predominant mode. In Central America, stray cats shed oocysts that survive in soil. United States prevalence of seropositivity: 22.5%.
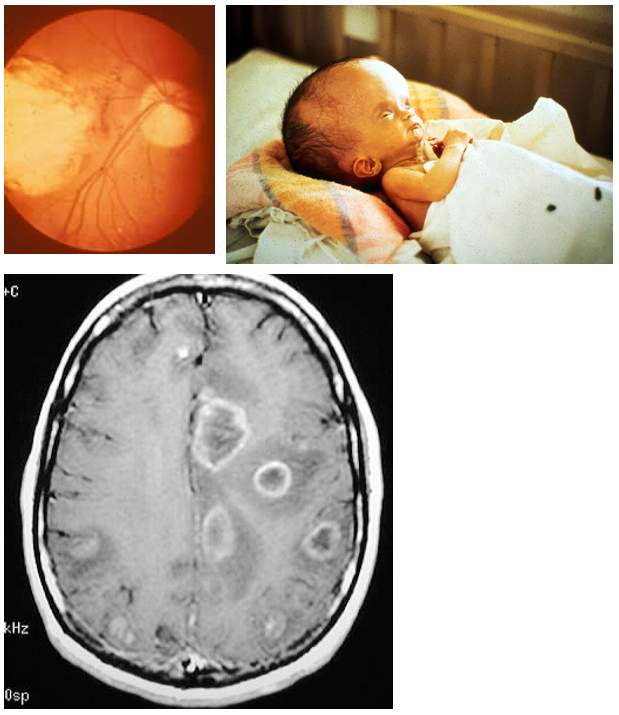
Congenital infection
- Hydrocephalus/intracranial calcification/chorioretinitis
Normal hosts
- Asymptomatic > fever/lymphadenopathy.
- Chorioretinitis.
Immunocompromised (HIV > others)
- Ring-enhancing brain lesions.
- Disseminated infection.
Presumptive Dx
- Neurologic symptoms in patient with low CD4 (AIDS), ring-enhancing lesions in brain on CT scan and + serology.
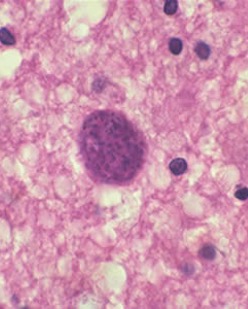
Direct identification of organisms
- Tissue biopsy
Serologic testing
- IgM for primary infection.
- IgG for reactivation.
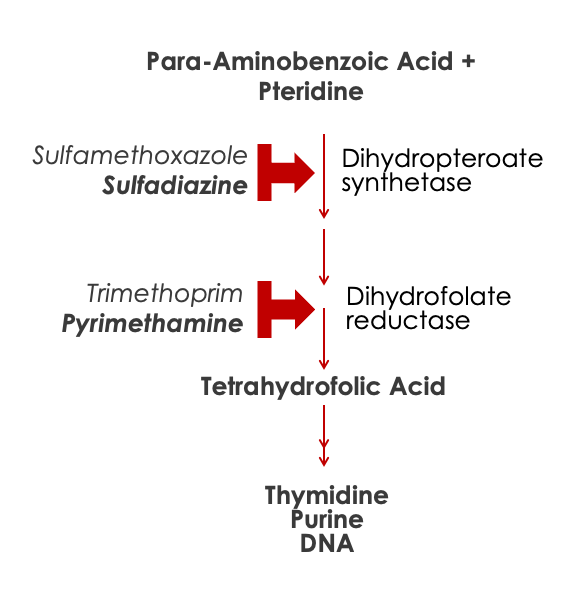
Pyrimethamine-sulfadiazine.
HIV
- (CD4 < 100) Prophylaxis with TMP-SMX if IgG+.
Pregnant women
- Avoid cats and raw meat.
Micro: Tissue protozoa; disseminate and encyst.
Epidemiology: Oocysts from cat feces, or undercooked meat.
Clinical:
- Congenital:
- Hydrocephalus.
- CNS calcifications.
- Chorioretinitis
- Normal Immunity:
- Flu-like illness with adenopathy.
- Chorioretinitis.
- Immune Suppressed:
- Seizures.
- Ring-enhancing lesions on head CT.
Diagnosis: Mostly clinical dx; CT imaging; serology
Treatment: Pyrimethamine-Sulfadiazine.
Prevention:
- Cook meat well.
- Take care with cat feces.
- TMP-SMX in AIDS.
