


Tropics, esp. children, where autoinfection is common.
- Nematodes (roundworms) hookworm-like adults, fecal-soil-skin transmission, plus lung migration and autoinfection
- Closely related to Hookworm.
- Skin penetration (not oral), with lung phase.
- Parasite does not need to exit the body to complete life cycle—autoinfection.

- Skin migration: Rash is common (“larva currens”).
- Lung migration: Similar to Ascaris and hookworm.
- GI upset: Abdominal pain or diarrhea.
- May persist for years or decades via autoinfection.

- Hyperinfection.
- T-lymphocyte depletion (immunosuppression post-solid organ transplant, chemotherapy, steroids, or HIV).
- Faster reproduction cycle.
- Migration to ectopic sites.
- Spread of fecal bacteria to sterile sites (blood, CNS, peritoneum, lungs . . .)
Strongyloides stercoralis late infection
- Rash.
- “Larva currens” on exam.
- Eosinophilia common (but not always).
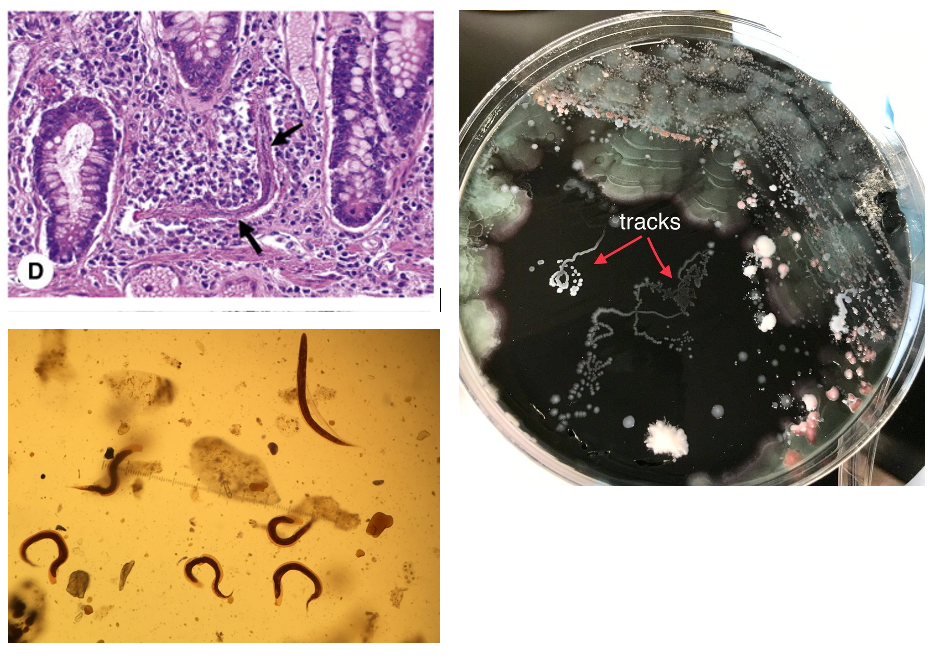
- Look for larvae in stool (<50% sensitive), sputum culture (“tracks”), or tissue.
- Serology (ELISA IgG) if immunocompetent.
Ivermectin (treat before immunosuppression).
- Improved sanitation.
- Wear shoes.
AKA: “Strongy.”
Micro:
- Nematodes (roundworms) hookworm-like adults.
- Fecal-soil-skin transmission.
- Lung migration and autoinfection.
Epidemiology: Tropics, (esp. children), autoinfection common.
Clinical:
- Larva Currens.
- Loeffler’s.
- GI upset.
- Hyperinfection.
Diagnosis:
- Rash.
- Eosinophilia.
- Sputum or CSF for larvae.
Therapy: Ivermectin (treat before immunosuppression).
Prevention: Preemptive Rx. Improved sanitation, wear shoes.