


Questions for consideration
- What pathogens cause the disease malaria?
- How is malaria transmitted?
- Which form of malaria is the most dangerous and why?
- Which species of malaria have latent forms?
- Which disease(s) does malaria most commonly mimic, and what are the specific entities on the differential for acute fever in returned travelers?
- How is malaria diagnosed?
Malaria
For each of the following parameters, select whether values increase, decrease, or stay the same in severe malaria.
Decreased. Coma is a characteristic and an ominous feature of severe falciparum malaria. Cerebral malaria manifests as a diffuse symmetric encephalopathy; focal neurologic signs are unusual, but seizures are relatively common.
Decreased. Hypoglycemia, an important and common complication of severe malaria, is associated with a poor prognosis and is particularly problematic in children and pregnant women. Hypoglycemia in malaria results from both a failure of hepatic gluconeogenesis and an increase in the consumption of glucose by the host and, to a much lesser extent, the malaria parasites.
Increased. Acute kidney injury is common in severe falciparum malaria. The pathogenesis of renal failure is unclear but may be related to erythrocyte sequestration and agglutination interfering with renal microcirculatory flow and metabolism. Clinically and pathologically, this syndrome manifests as acute tubular necrosis.
Decreased. Acidosis, resulting from accumulation of organic acids, is an important cause of death from severe malaria, which in adults is often compounded by coexisting renal impairment. Hyperlactatemia commonly coexists with hypoglycemia.
Increased. Adults with severe falciparum malaria may develop noncardiogenic pulmonary edema even after several days of antimalarial therapy.
Unchanged. Severe malaria is generally a high-output state. Pulmonary edema, when present, is non-cardiogenic in nature.
Question
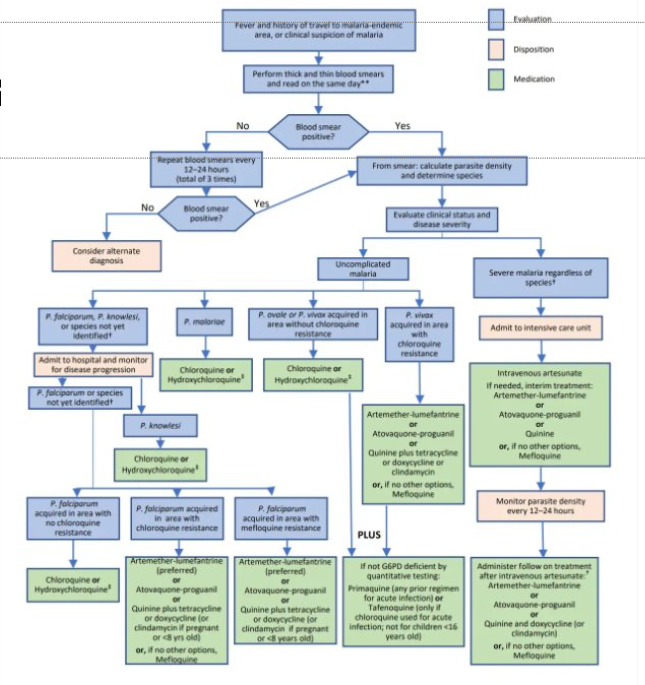
What are the recommendations for treatment of malaria, and what specific factors dictate the regimen of choice?
- Factors.
- Severity.
- Degree of parasitemia (Percent of RBCs infected with parasite per high-power field).
- Whether the patient can take oral medications safely (alert and protecting airway).
- Region of acquisition and risk for drug-resistance.
- What species of plasmodium will determine the need for treatment of the hepatic phase.
Test your knowledge
- Plasmodium falciparum.
- Plasmodium vivax.
- Plasmodium ovale.
- Plasmodium malariae.
- Bite of female anopheles mosquito.
- The mosquito transmits sporozoites—the infectious form. These mature in the human host, using RBCs to mature and asexually divide into thousands of merozoites—some of which further develop to gametocytes which are taken up by mosquitos during a blood meal. Sexual reproduction occurs in the mosquito—making humans an intermediate host.
P. falciparum is the most common and most dangerous species and can cause severe malaria, because P. falciparum can infect RBCs of all ages, while other species infect only immature RBCs/Reticulocytes.
In P. vivax and P. ovale infections, a proportion of the intrahepatic forms do not divide immediately but remain inert for a period ranging from 2 weeks to ≥1 year. These dormant forms, or hypnozoites, are the cause of the relapses that characterize infection with these species.
- The presentation of fever and jaundice can mimic the presentation of acute hepatitis.
- The differential diagnosis for fever in a traveler/returned traveler is very broad.
- Some key diseases to include on the differential for fever in the traveler/returned traveler without localizing signs/symptoms are diseases that may be life-threatening if not identified and include:
- Typhoid fever.
- Dengue fever.
- Rickettsial infections.
- The gold standard for diagnosis remains thick and thin smears that help identify the species of Plasmodium and can provide the degree of parasitemia.
- Rapid antigen detection kits are used as alternative where microscopy or expertise is unavailability.
Image credits
Unless otherwise noted, images are from Adobe Stock.