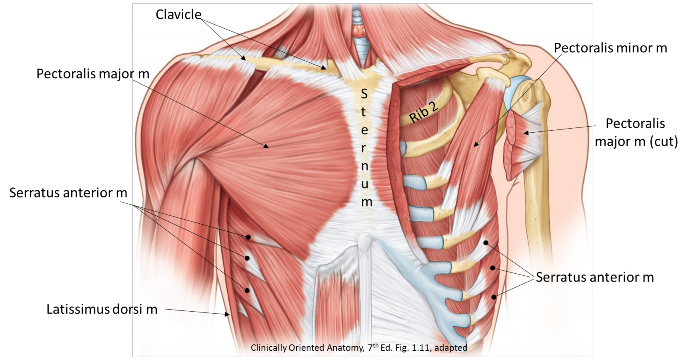
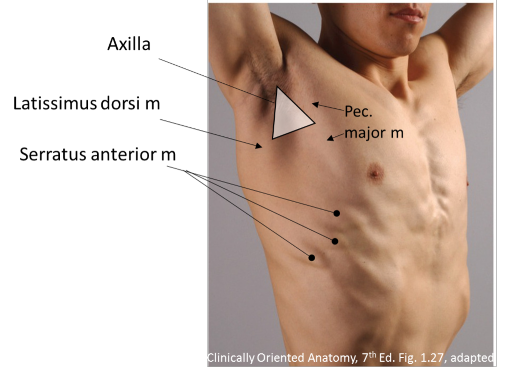
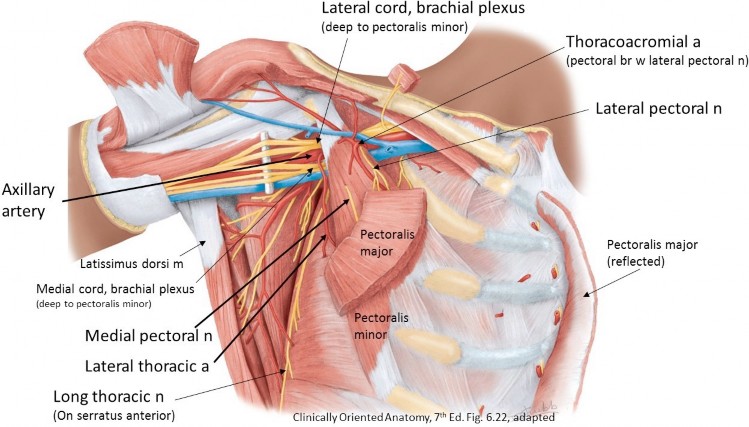
The axilla is the pyramid-shaped space inferior to the shoulder joint, where the arm meets the thorax. It is filled with nerves, vessels, and lymph nodes. Externally, the landmarks of the axilla are the anterior and posterior axillary folds, formed by the underlying pectoralis major and latissimus dorsi muscles, respectively. The depression between the folds is the axillary fossa (armpit). We will consider the axilla in much more detail when we study the upper limb.
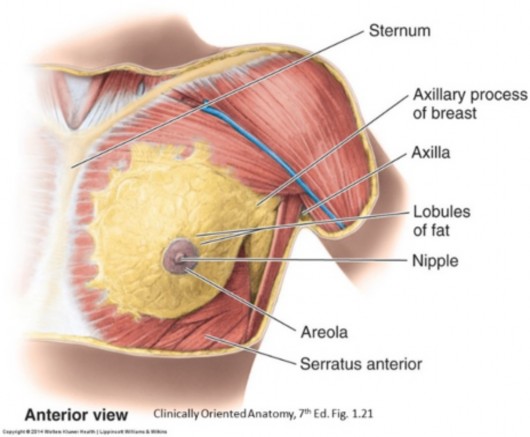
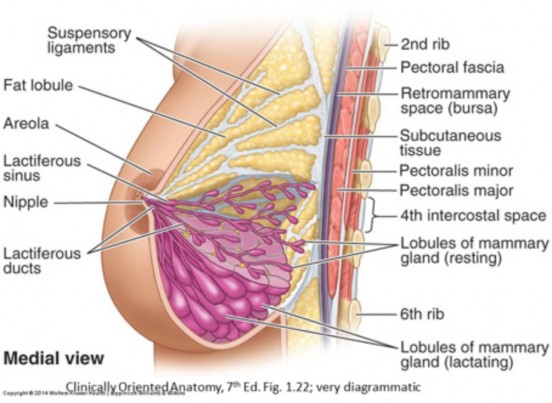
The breasts are modified sweat glands formed from ectoderm and specialized for milk production. They are contained entirely within the superficial fascia of the anterior thorax.
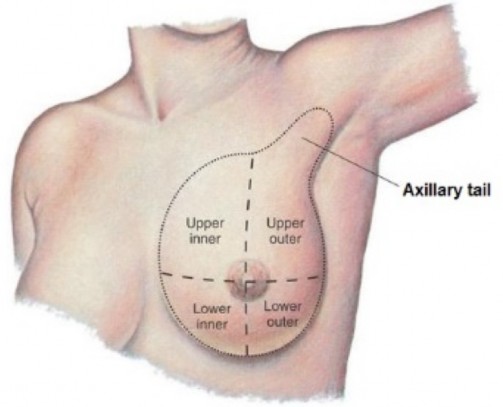
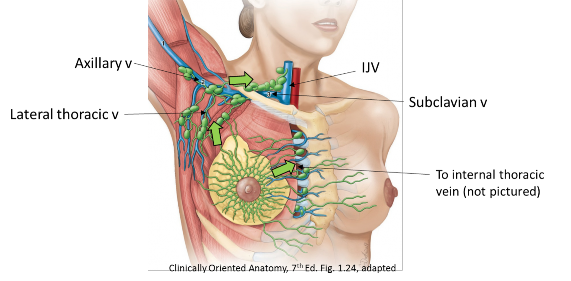
Deep plexuses of lymph vessels are formed around the glandular tissue and ducts. From here, drainage is into two sets of lymph nodes: parasternal and axillary. For descriptive and clinical purposes, the breast is subdivided into quadrants, using the nipple as the center of the clock face. The upper lateral quadrant contains more breast tissue than the other quadrants. Therefore, it is the most common site of breast cancer.
-
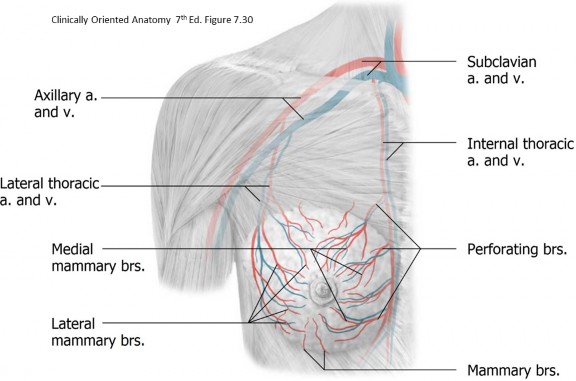
- The medial (inner) quadrants of the breast drain to parasternal nodes, located along the internal thoracic vessels on the internal surface of the anterior chest wall.
- The lateral (outer) quadrants of the breast drain to axillary nodes. These are 12 to 30 nodes forming a connected chain around the veins of the axilla. Since the lateral quadrants are larger, about 75% of the breast’s lymph percolates through the axillary lymph nodes. Besides the breast, axillary nodes receive lymph from the upper limb and the superficial tissues of the trunk wall as far inferiorly as the umbilicus.
After leaving the axillary and parasternal nodes, lymph flows through lymph trunks in the thorax and neck to reach the body’s two largest lymph vessels = the right lymph duct on the right and the thoracic duct on the left.