Comparing the upper and lower limbs: Mobility vs. stability
Although the two sets of limbs have important structural and functional differences, they are built upon a similar plan, and it is important that students recognize these similarities up front.
Upper limb:Mobility
The upper limb is built for positioning the hand in space so it can carry out its functions as a sensory and grasping organ. It has freedom of movement so the hand can roam, reach, and retrieve (MOBILITY).
Lower limb:Stability
On the other hand (hah), the lower limb has restricted freedom of movement—in humans, it is built for supporting the trunk and providing the power necessary for locomotion. When upright, the foot doesn’t roam since it is in contact with the ground (STABILITY).
In the upper limb, stability is sacrificed for mobility—it’s the opposite case in the lower limb.
Named parts of the limbs
Each limb is composed of a limb girdle and a free limb. The girdle provides the link between the free limb and the trunk. The free limbs in turn have three parts:
1
Proximal
2
Intermediate
3
Terminal segments
Table6.1
Limb
Limb girdle
Free limb segments
Proximal
Intermediate
Distal
UPPER
Pectoral (shoulder)girdle
Arm
Forearm
Hand
LOWER
Pelvic girdle
Thigh
Leg
Foot
Osteology of the limbs
Figure 6.1
Figure 6.2
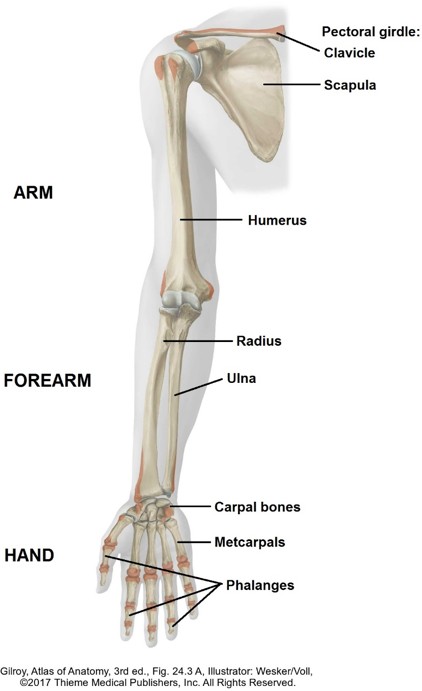
Upper limb
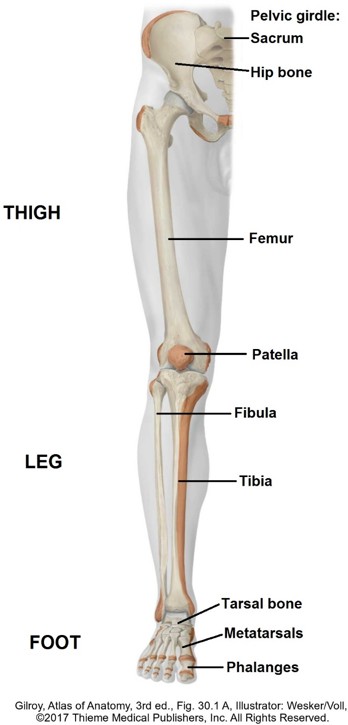
Lower limb
The pectoral girdle consists of the scapula (shoulder blade) and clavicle (collar bone).
Bones of the free upper limb:
Humerus in the arm.
Radius and ulna in the forearm.
Eight carpal bones arranged in two rows are in the proximal hand, five metacarpal bones are in the mid-hand, and phalanges are the bones of the digits (fingers). The metacarpal bones are identified by Roman numerals starting from the radial side of the hand = metacarpal I is that of the thumb (first digit), while metacarpal V is that of the little finger (fifth digit). The thumb contains two phalanges (proximal and distal) while the other four digits contain three phalanges each (proximal, middle, and distal).
The pelvic girdle consists of left and right hip bones plus the sacrum. The ring of bones is joined together as a unit by strong joints. During development and growth,three primary bones (ilium, ischium, and pubis) fuse to form each hip bone.
Bones in the free lower limb:
Femur in the thigh.
Tibia and fibula in the leg.
Seven tarsal bones are in the proximal foot (their arrangement into two rows is not as evident as the arrangement of carpal bones in the hand), five metatarsal bones are in the mid-portion of the foot, and phalanges are within the toes (digits). As in the hand, the metatarsals are identified by Roman numerals I to V, starting at the big toe. Two phalanges are present in the big toe (proximal and distal), while the other toes have three phalanges each (proximal, middle, and distal).
Introduction to joints
Joints (articulations) are the functional units of the musculoskeletal system. A joint is the union of two or more skeletal elements (usually bones). The Greek root “arthro” means “joint”—another name for a joint is an arthrosis—and the study of joints is arthrology.
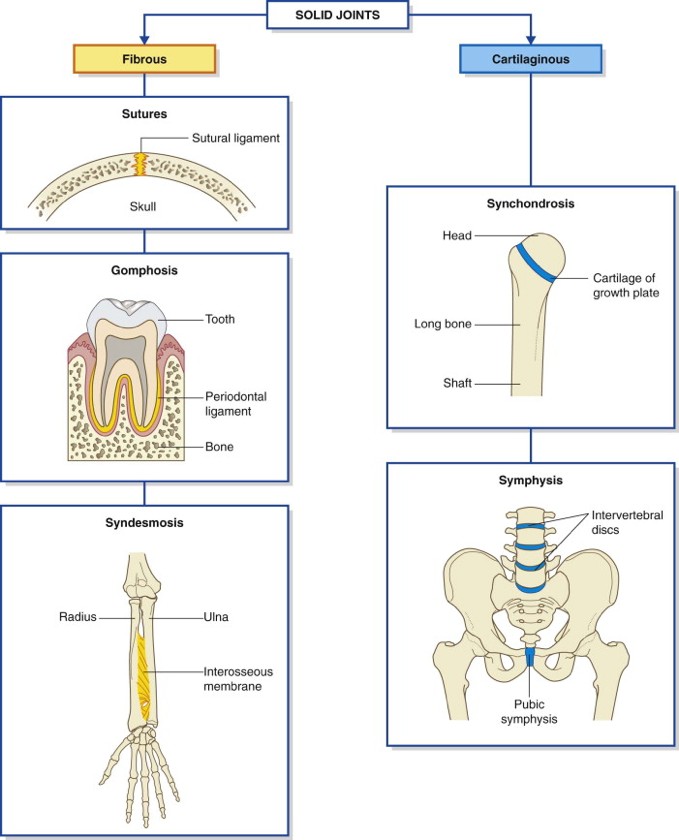
Three major types of joints, categorized by mobility, are fibrous, cartilaginous, and synovial. Fibrous and cartilaginous joints (solid joints) are immobile or semi-mobile and are common in the head and trunk, whereas synovial joints are freely moveable and are the main joint type in the limbs.
Figure 6.3 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., 1.22.
Fibrous joints
In fibrous joints, the skeletal elements are connected by fibrous tissue. These joints are either immobile or slightly mobile.
The skull bones in adults are held together firmly by a type of fibrous joint called a suture. Sutures are soft and moveable in the fetus and child, allowing the skull to change shape during delivery through the vaginal canal and to grow during childhood. Large fibrous membranes are present after birth at the intersections of sutures. These are called fontanelles (the “soft spots” in an infant’s head). The largest of these normally closes during the second year of life.
Another subtype of fibrous joint is a syndesmosis. This joint provides some movement—but its main function is to provide a stable union. You should know about the radio-ulnar syndesmosis in the forearm and the tibiofibular syndesmosis in the leg. These joints are formed by a band of fibrous tissue called an interosseous membrane that binds together the two bones in the forearm and leg, respectively. In addition, the tibiofibular syndesmosis has two ligaments that firmly unite the distal parts of the tibia and fibula—important stuff for the stability of the ankle region.
The union of a tooth to an alveolus (tooth socket) by the periodontal ligament is another type of fibrous joint.
Cartilaginous joints
In these joints, the bones are linked together by cartilage.
When joined by hyaline cartilage, the joint is a synchondrosis. Growth plates in the bones of children are an example of a synchondrosis. True synchondroses are temporary—they disappear with age, so adults don’t have these kinds of joints.
When joined by fibrocartilage, the joint is a symphysis. Two examples of symphyses are the intervertebral joints where intervertebral discs unite adjacent vertebral bodies and the pubic symphysis where an interpubic disc unites the hip bones.
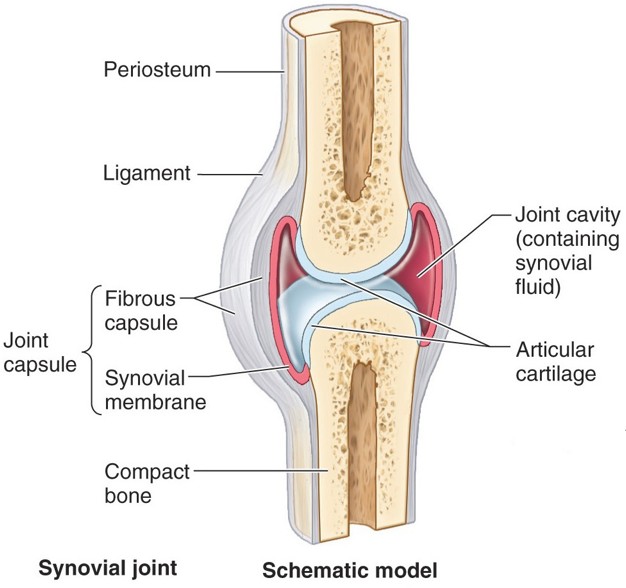
Synovial joints
These joints are the “Big Enchilada” in the limbs. Rather than having solid tissue between the skeletal elements that restricts movement, synovial joints are characterized by a greater range of motion afforded by a joint cavity between the articular surfaces. The joint cavity allows bones to move relative to one another, to slide, spin, or roll, for example.
An outer portion made of dense connective tissue. This surrounds the joint cavity and connects the bones together, preventing them from being pulled apart.
An inner layer of loose connective tissue, richly supplied with blood, called the synovial membrane. It manufactures synovial fluid, which lubricates and nourishes the articular surfaces. This “joint oil” is nature’s “WD-40.” The word synovial derives partially from the Latin “ovum” (= egg), a reference to synovial fluid having the consistency of egg white.
Usually hyaline cartilage, it covers the surfaces of the bones inside the joint capsule to resist and distribute compressive forces imparted on the joint by muscles and gravity. The synovial membrane attaches around the edges of the articular cartilage, but does not cover it. Since cartilage is radiolucent (transparent to X-rays), radiographs of healthy joints depict the joint cavity as much larger than it really is.
Ligaments reinforce the joint. Depending on the joint, these may be inside the articular capsule (intracapsular ligaments), localized thickenings of the articular capsule itself (capsular ligaments), or discrete ligaments outside the articular capsule (extracapsular ligaments).
A few synovial joints (TMJ, knee) also contain an articular disc. These are made of fibrocartilage and fit like shelves between the articulating surfaces of bones. In the knee, the articular discs are crescent-shaped, so they are known as menisci. These absorb compressive forces, improve the fit of articular surfaces, and facilitate complex movements such as simultaneous rotation and gliding of skeletal elements.
Clinical correlation
Since synovial joints are highly mobile, they must be stabilized to prevent dislocation. If dislocation occurs, the articular surfaces become misaligned and the joint loses function.
Three factors influence joint stability:
1. the shapes of the articular surfaces of bones,
2. the number and arrangement of reinforcing ligaments, and 3. the tone of the muscles that cross the joint.
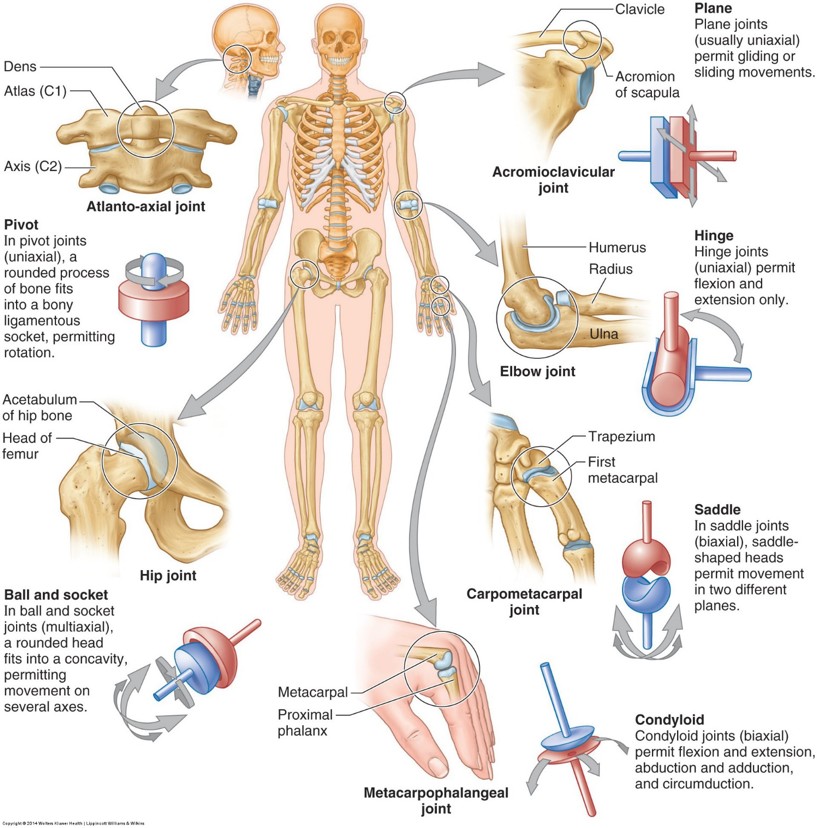
Movements that occur at synovial joints are largely determined by the shape and fit of the surfaces of the skeletal elements joined together. As you study joints, consider the shapes of the articular surfaces of bones. Below are common types of synovial joints categorized by their movements and the number of axes they move around.
The articular surfaces are flat, so skeletal elements can slide across one another in many directions, but no rotation occurs. The articulations between the carpal bones in the wrist (intercarpal joints) and between the distal clavicle and acromion of the scapula (acromioclavicular joint) are examples.
Movement around a single axis, transverse to the articular surfaces. Flexion and extension movements occur at hinge joints. Example: the articulation between humerus and ulna at the elbow.
Movement around a single axis, oriented along the shaft of a bone. Rotational movements occur at pivot joints. Examples: the proximal articulation between radius and ulna near the elbow allows the radius to rotate on the ulna (the axis is longitudinal, down the shaft of the radius); at the atlanto-axial joint, the first cervical vertebra (C-1—the atlas) rotates on C-2 below it (the axis), allowing one to shake their head to say “no.” The axis of rotation is longitudinal, down the vertebral column.
Movement around two axes. The articular surfaces are oval and complementary—one convex and one concave—like an egg resting in a spoon. Examples:
The articulation between the distal radius and the first row of carpal bones at the wrist
The “knuckle joints” of the hand (metacarpophalangeal joints).
Flexion, extension, abduction, and adduction can occur, as can a limited amount of circumduction, a combination of the above movements that circumscribes a cone shape in space.
Movement around two axes. Both articular surfaces have convex and concave surfaces—like saddles. Example: the carpometacarpal joint of the thumb. As in condylar joints, flexion, extension, abduction, adduction can occur. The thumb saddle joint combines these movements with rotation of the first metacarpal bone to permit the pulp surface of the thumb to contact the same surfaces of the other fingers of the hand, a special movement called opposition of the thumb.
Movement around multiple axes. One of the articular surfaces is round and the other is a cup-shaped socket. Found at the shoulder and hip joints. All the previously described movements can occur at these joints: flexion, extension, abduction, adduction, circumduction, and rotation.
Joints in the limbs
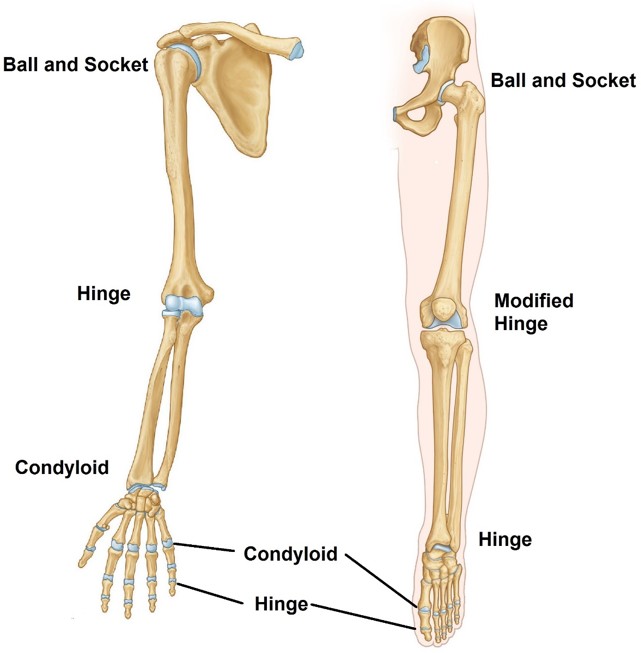
Figure 6.7 Compare the joint types of the limb girdles and segments of the free limbs in the two sets of limb; there are quite a lot of similarities. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURES 5.4 AND 6.3.
Limb girdles
Free limbs
Girdle is an old-fashioned term that means “belt that surrounds.”
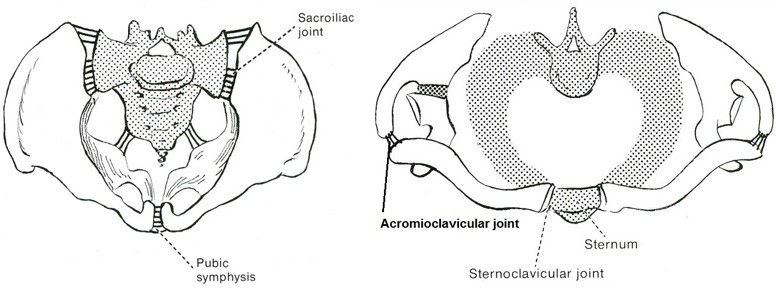
This seems appropriate when considering the pelvic girdle, which is composed of a complete ring of bones = the hip bones join to the sacrum posteriorly via the sacro-iliac joints and to one another anteriorly at the pubic symphysis.
But what about the pectoral girdles—do they form a belt around the axial skeleton? Not really—the belt is incomplete; the two pectoral girdles do not join to one another—anteriorly nor posteriorly. The clavicles attach to the axial skeleton (sternum) anteriorly via the sternoclavicular joints. The scapulae and clavicles articulate at the acromioclavicular joints. The scapulae are mobile since they have no direct attachment to the axial skeleton (but do have a motion interface with the ribs and body wall) or to one another (there is gap posteriorly between the two “shoulder blades”). Because of this, each upper limb can move independently, can be raised above the head (because the scapulae can rotate upward), and can explore a wide range of space anterior to the body (because the scapulae can slide forward around the cone-shaped rib cage).
Figure 6.6 Superior views: The pelvic girdle is a complete bony ring (left), the pectoral girdle is not (right) = Adaptations for stability and mobility of the two limbs. HOLLINSHEAD’S TEXTBOOK OF ANATOMY, 5TH ED., FIGURE 14-2. LIPPINCOTT.
Note joint similarities and differences in the two sets of limbs.
The proximal segments of the free limbs are linked to their respective girdles by ball-and-socket joints. The humerus is attached to the pectoral girdle at the glenohumeral (shoulder) joint while the femur is joined to the pelvic girdle at the hip joint.
A hingejoint is between the proximal and intermediate segments of both limbs—the elbow in the upper limb and knee in the lower limb. We will see later that the knee is a modified hinge joint and much more complex than the elbow.
The pairs of bones in the forearm and leg articulate with one another at both their proximal and distal ends. These are the radio-ulnar and tibiofibular joints (proximal and distal). They are different in the two limbs, reflecting the functional differences in forearm and leg.
In the leg, the tibia and fibula are fixed to one another rigidly by a plane joint (proximal) and a syndesmosis (distal)—so little movement occurs at either tibiofibular joint. This is important for stability of the ankle region.
Conversely, the radio-ulnar joints in the forearm are pivot joints so that the radius and ulna can move in relation to each other and move the hand through a 180 degree arc—producing the movements of supination and pronation. When the bones of the forearm are parallel, the palm of the hand faces forward in the anatomic position and the hand is supinated (palms facing up—a bowl of “soup in your hand”). Pronation turns the palm so it faces posterior and the thumb is medial—this occurs when the radius is crossed over the ulna. This motion cannot (and should not!) occur in the leg.
The joints between the intermediate and terminal segments of the upper and lower limbs are different, reflecting the differences in their mobility. In the lower limb, the ankle joint is a hinge joint where the most proximal tarsal bone (talus) articulates with both the tibia and fibula. The movements that occur in the ankle are dorsiflexion (toes point up) and plantarflexion (toes point down). In contrast, the wrist joint of the upper limb is a condyloid joint where carpal bones articulate with the distal radius. The movements here are many: abduction, adduction, flexion, extension, and circumduction.
Intercarpal joints in the hand and intertarsal joints in the foot are plane joints that permit slight gliding movements between carpal and tarsal bones, respectively. Movements at intercarpal joints augment movements of the wrist joint and increase range of motion and suppleness. Movements between tarsal bones help produce inversion and eversion of the foot—turning the sole of the foot medially or laterally, respectively. Note that inversion and eversion are much more limited and DO NOT correspond to supination and pronation in the hand, because the two bones in the leg do not cross as they do in the forearm.
The carpometacarpal and tarsometatarsal joints are plane joints that afford slight amounts of gliding. The articulating bones are tightly bound together by ligaments, so little movement occurs. The exception is the first carpometacarpal joint of the thumb between the trapezium and first metacarpal bone. This is a saddle joint (described earlier).
Metacarpophalangeal (MCP) and metatarsophalangeal (MTP) joints are condyloid joints. Flexion, extension,abduction, and adduction of the digits can occur—although the range of these movements is usually much greater in the digits of the hand.
Interphalangeal (IP) joints in the hands and feet are hinge joints that only permit flexion and extension.
Development of the limbs
Note
Lower limb development lags slightly behind that of the upper limb—a cranial-to-caudal pattern of development we have seen before.
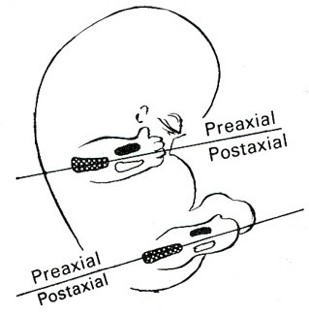
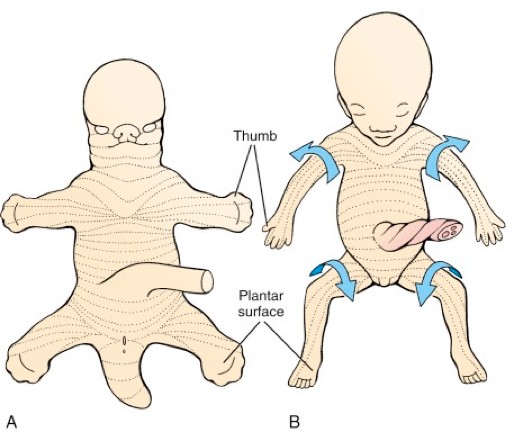
After folding of the embryo, two pairs of limb buds begin to grow from the ventrolateral body wall. Each limb bud is shaped like a ping-pong paddle with flattened ventral and dorsal surfaces. Separating these surfaces are rather sharp cranial and caudal edges called the preaxial border and postaxial border, respectively.
Figure 6.8 Developmental rotation of limbs. LARSEN’ S HUMAN EMBRYOLOGY, 5TH ED., FIGURE 20-28.
Limb buds elongate and lose their paddle shape. Even though they are now cylindrical in cross-section, the preaxial and postaxial borders can still be recognized:
Preaxial borders are indicated by the thumb and big toe
Postaxial borders are indicated by the “pinky” finger and little toe.
Preaxial bones are radius and tibia; postaxial bones are ulna and fibula.
Limbs rotate, but in opposite directions:
Upper limb rotates outward, from an elbows-out, palms toward belly, and thumbs up position to elbows facing posterior and palms facing forward position. The radius (preaxial bone) and thumb are now on the lateral side of the upper limb in the anatomic position.
Lower limb rotates in the opposite direction (inward), from a knees pointing out, soles of the feet facing in, and big toe pointing up position to knees facing forward and soles of feet facing down position. The tibia (preaxial bone)and big toe are now on the medial side of the upper limb in the anatomic position. The axes of the foot and the rest of the lower limb form a 90 degree angle, so that the sole of the foot can contact the ground.
Joints begin to develop as clefts filled with fibroblasts between the condensations of somatic mesoderm that produce the cartilage bone models.
Recall that the first eight weeks of human development are the embryonic period, when the body’s organ systems are developing—a period of rapid cell division and differentiation. This is the time when developmental processes are most vulnerable and congenital anomalies appear. For example, during week seven the digital rays in the hands and feet begin to separate into individual fingers and toes. If this process is faulty, syndactyly (fusion of digits) could occur, the most common congenital anomaly of limbs.
Limb musculature
Figure 6.10
There are functionally equivalent groups of muscles in the upper and lower limbs. Embryonic ventral and dorsal muscle masses, derived from paraxial mesoderm (somites), invade the limb buds prior to limb rotation.
The ventral muscle mass gives rise to the flexors and pronators of the upper limb and to the flexors and adductors of the lower limb.
The dorsal muscle mass gives rise to the extensors and supinators of the upper limb and to the extensors and abductors of the lower limb.
Example: Muscles in the anteriorarm (from the embryonic ventral muscle mass) produce flexion at the elbow joint. The corresponding joint in the lower limb is the knee—however, because of the rotation of the embryonic lower limb—muscles in the posteriorthigh produce flexion at the knee, even though they came from the embryonic ventral muscle mass of the lower limb!
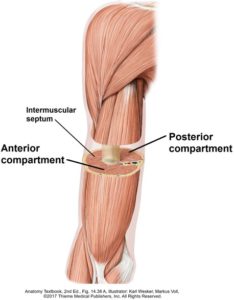
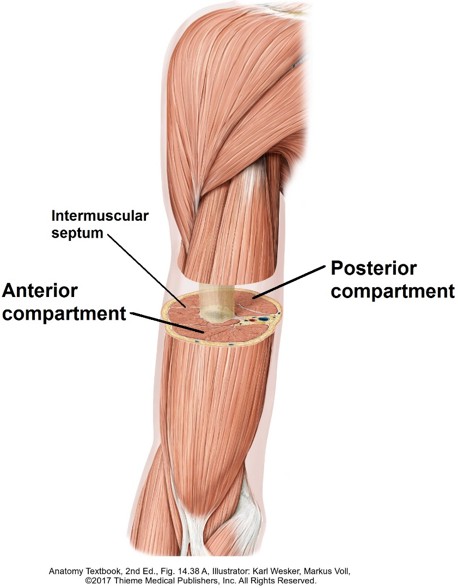
Functionally related muscles are organized into limb compartments. Let’s illustrate this by considering the upper limb. Muscles that flex the joints between the arm, forearm, and hand are located within the anterior compartments of the upper limb, in the part of the limb proximal to the joint moved. Muscles that extend the joints are in the posterior compartments. The compartments are defined by bones and deep fascia.
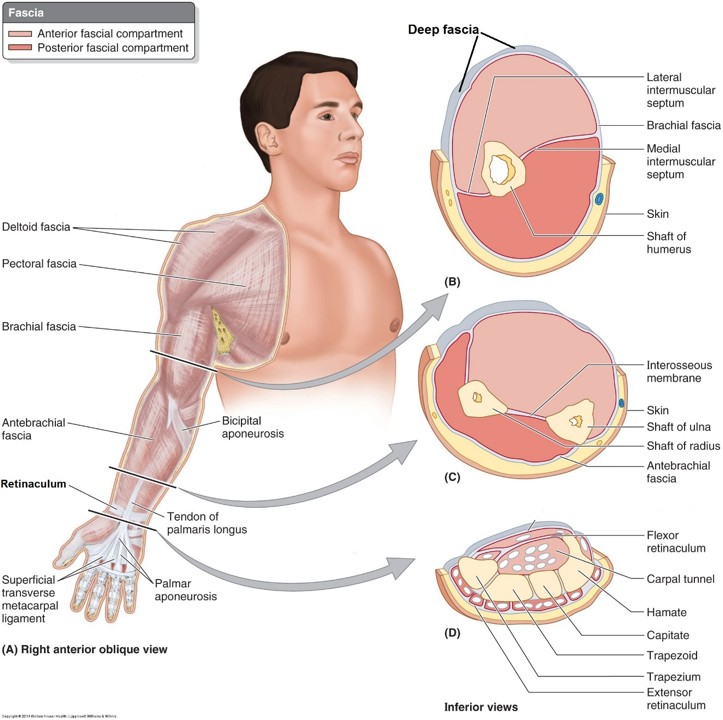
Limb fasciae
The superficial fascia is made of loose connective and fatty tissue. It contains cutaneous nerves and vessels, including large superficial veins.
The deep fascia is dense connective tissue that forms a snug-fitting sleeve around the entire limb, from proximal to distal. The deep fascia extends inward between muscle groups to attach to underlying bones, producing so-called intermuscular septa. The deep fascia, intermuscular septa, and bones of the limbs define the limb compartments.
The deep fascia of the limbs has several functions: it provides a surface for muscle attachment, protects the contents of compartments, prevents displacement of muscles within compartments so that they exert pull on their tendons in one direction, and produces pressure within compartments to encourage venous return to the heart.
Around the wrist and ankle, the deep fascia is thickened into bands called retinacula. These hold down the muscle tendons passing into the hands and feet, so they don’t come loose and “bowstring.”
Figure 6.11 The deep fascia of the upper limb forms an inelastic stocking around the muscle compartments. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 6.14.
Clinical correlation
The deep fascia is not elastic. Edema within closed muscle compartments (due to trauma, such as fractures) creates pressure. If the tissue pressure is high enough, it can compromise blood flow within the compartment, potentially leading to muscle and nerve ischemia and necrosis. This is called compartment syndrome and may have to be treated by incision of the fascia (fasciotomy) to relieve the pressure.
Innervation of limbs
Since the upper and lower limb buds grow from the ventral and lateral portions of the body wall, they become innervated by ventral rami of spinal nerves: C-5 to T-1 spinal nerves supply the upper limb while the lower limb receives spinal nerves L-2 to S-3.
As the ventral rami enter the limb buds they split into anterior and posterior divisions. Muscles derived from the embryonic ventral muscle masses are innervated by anterior divisions (flexor and adductor muscles), while muscles derived from the dorsal muscle masses are innervated by posterior divisions (extensor and abductor muscles).
The tissues that migrate into the limbs do so in a segmental fashion (e.g., muscle building mesoderm) and receive segmental innervation from the spinal cord. Before reaching muscles, the ventral rami of spinal nerves commingle and exchange nerves fibers, forming somatic nerve plexuses. The brachial plexus supplies the upper limb whereas the lumbosacral plexus innervates the lower limb. Muscle actions in the limbs are therefore usually the result of impulses carried in two or more spinal nerves from two or more spinal cord segments.
Innervation of joints
Joints are richly supplied with sensory nerves. Anyone who has experienced a joint injury knows this!
Hilton’s Law states:
Nerves that innervate muscles that move a particular joint also supply the sensory nerve fibers to that joint.
Myotomes
The concept of myotome is central to understanding the segmental innervation of limbs. A myotome is a mass of skeletal muscle supplied by a single spinal cord segment and the axons derived from the corresponding spinal nerve.
Most muscles in the limbs are made of several myotomes, so most muscles are innervated by axons from more than one spinal nerve.
For a particular joint, agonists (“prime movers”—the muscles supplying the major force to move the joint) and antagonists (muscles on the opposite side of the limb that relax when the agonist contracts) are innervated by spinal cord segments that are close together. For example, flexors of the elbow are controlled by C-5 and C-6 segments,while extensors are controlled by the next two contiguous segments at C-7 and C-8. Elbow flexors are in the anterior compartment of the arm—the antagonist extensors are in the posterior compartment.
Higher levels of the spinal cord control the more proximal joints of the limbs, whereas the more distal joints are controlled by spinal cord levels lower down. This reflects the segmental innervation of the limbs as they elongate and rotate. Refer to Table 6.2and Table 6.3.
Table 6.2 Key myotomes of the upper limb
Joint
Movement
Myotomes
Shoulder
Abduction
Adduction
C-5
C-6, C-7, C-8
Shoulder
Flexion
Extension
C-5, C-6
C-7, C-8
Elbow
Flexion
Extension
C-5, C-6
C-7, C-8
Wrist
Flexion and extension
C-6, C-7
Metacarpophalangeal (MCP) (digits)
Flexion and extension
C-7, C-8
Metacarpophalangeal (MCP) (digits)
Abduction and adduction
C-8, T-1
Table 6.3 Key myotomes of the lower limb
Joint
Movement
Myotomes
Hip
Flexion
Extension
L-2, L-3
L-4, L-5, S-1
Knee
Extension
Flexion
L-3, L-4
L-5, S-1
Ankle
Dorsiflexion
Plantarflexion
L-4, L-5
S-1, S-2
Clinical correlation
The segmental innervation pattern of limbs has clinical relevance. If a patient experiences symptoms of weakness, it could be the result of a problem at several possible levels: spinal cord, spinal nerve root, and/or peripheral nerve. Which one? Knowledge of anatomy and clinical testing can provide clues.
Let’s say the weakness is with elbow flexion. The biceps brachii and brachialis muscles are the prime movers, innervated by the musculocutaneous nerve (C-5 and C-6).
Are other muscles supplied by C-5 and C-6 weak?
C-5 and C-6 supply regions of skin in the upper limb—is sensation in those regions normal?
Are reflexes involving C-5 and C-6 normal—indicating normal reflex arcs through the spinal cord?
Dermatomes
Definition
A dermatome is a region of skin supplied by a single spinal nerve.
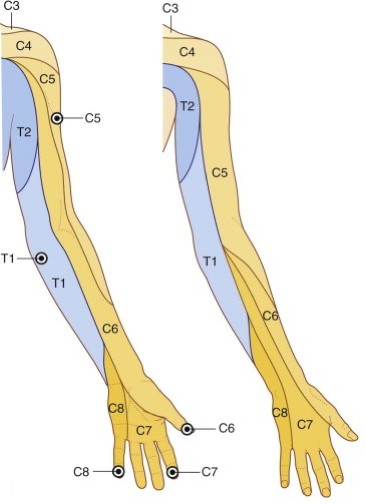
Figure 6.12 Dermatome map of the upper limb. The bulls-eyes are autonomous zones (key sensory points), where dermatomes don’t overlap and are best sites for clinical testing. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 7.15.
Recall that there was a nice clean segmented arrangement of dermatomes in the trunk—like stripes painted around the body. It is not that way in the limbs because of their developmental elongation and rotation.
The sensory nerve pattern was established early on in the “paddle-shaped” limbs, before rotation. Skin along the preaxial borders is supplied by spinal nerves from higher levels of the spinal cord, whereas skin along the postaxial borders receives nerves from spinal cord segments lower down.
Example: Upper Limb: Start at the shoulder and move along the preaxial (radial) border of the limb all the way down to the thumb, then move to the “pinky” finger, and then up the postaxial (ulnar) border of the limb to the axilla. Note the progression of dermatomes around the limb in topographic order: C-5, C-6, C-7, C-8, and then T-1.
As in the trunk, adjacent dermatomes overlap in places and are not separated by sharp clear-cut borders. The areas of skin where dermatomes do not overlap and are best for clinical testing are called autonomous zones.
Clinical correlation
Sensory problems can be caused by issues at several possible locations: spinal nerve (dermatome), peripheral nerve, or due to generalized pathologies that affect peripheral nerves (peripheral neuropathy).
If the pathology involves peripheral nerve entrapment, then the skin innervated by the peripheral nerve is the only area that will have sensory changes. Muscles innervated by that nerve would also be affected, although the sensory changes are usually seen before motor losses can be detected. Example: carpal tunnel syndrome.
The pattern of sensory loss presents distally in the limb initially—a region of numbness resembling a stocking or glove—then progresses more proximally (the area of sensory loss moves up the limb). Example: diabetic neuropathy.
Blood supply to the limbs
Without getting into too much detail, here are some interesting facts about the limb vessels. No need to memorize specifics yet, but, note the similarities in patterns of arteries and veins in the two sets of limbs. If you recognize this, it will make studying and comparing the limbs much easier.
Arteries
Veins
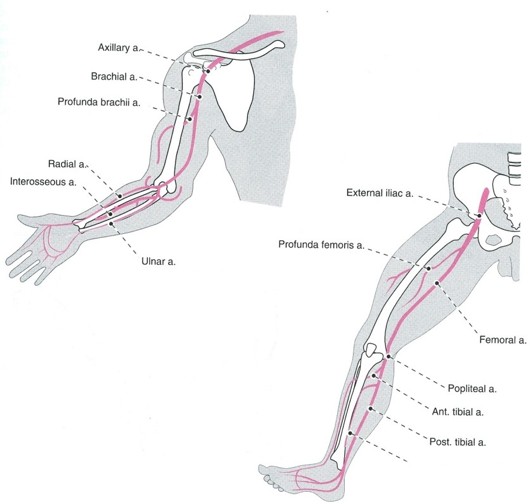
Figure 6.13 Similarities in the plans of arterial supply. Hollinshead’s Textbook of Anatomy, 5th ed., Figure 14-9.
The proximal segment in each free limb contains a single major artery: brachial artery in the arm, femoral artery in the thigh.
The arm and thigh receive a deep branch of the major artery: deep artery of the arm (profunda brachii artery) from the brachial artery and deep artery of the thigh (profunda femoris artery) from the femoral artery. The deep arteries are actually the major blood suppliers to the arm and thigh.
There are two arteries in the intermediate segments: radial and ulnar arteries in the forearm, anterior and posterior tibial arteries in the leg.
In the terminal segment of each limb, the two arteries of the intermediate segment join together to form superficial and deep anastomoses: superficial and deep palmar arches in the hand, superficial and deep plantar arches in the foot.This apparently insures blood supply to the hands and feet in the event that one artery becomes blocked or damaged.
The arterial arches give off arteries that supply the digits of the hands and feet.
Most venous blood from the hands and feet pass to their dorsal surfaces into venous plexuses that are visible just under the skin (look at the dorsum of your hands). This is due to the constant pressure exerted on the palms and soles.
The blood in the dorsal venous plexuses of the hands and feet are collected by large superficial veins that run along the preaxial and postaxial borders of the limbs. The preaxial veins are the cephalic vein in the upper limb and great saphenous vein in the lower limb. The postaxial veins are the basilic vein in the upper limb and small saphenous vein in the lower limb.
Smaller deep veins accompany arteries in the limbs. They are often paired and run immediately adjacent to the arteries; thus they are known as the venae comitantes (“companion veins”) of the arteries. For example, the brachial artery in the arm is accompanied by two brachial veins. The pulsations of the arteries in the limbs apparently helps propel the blood in the companion veins back to the heart.
The veins in the limbs contain valves that point toward the heart—these prevent backflow of blood that otherwise would occur due to gravity.
Lymphatic drainage of limbs
Most lymphatic vessels in the limbs course through the superficial fascia alongside the superficial veins (e.g., cephalic vein, great saphenous vein).
All lymph from the upper limb is filtered through nodes in the axilla.
All lymph from the lower limb passes through inguinal nodes in the groin.
Image credits
Unless otherwise noted, images are from Adobe Stock.