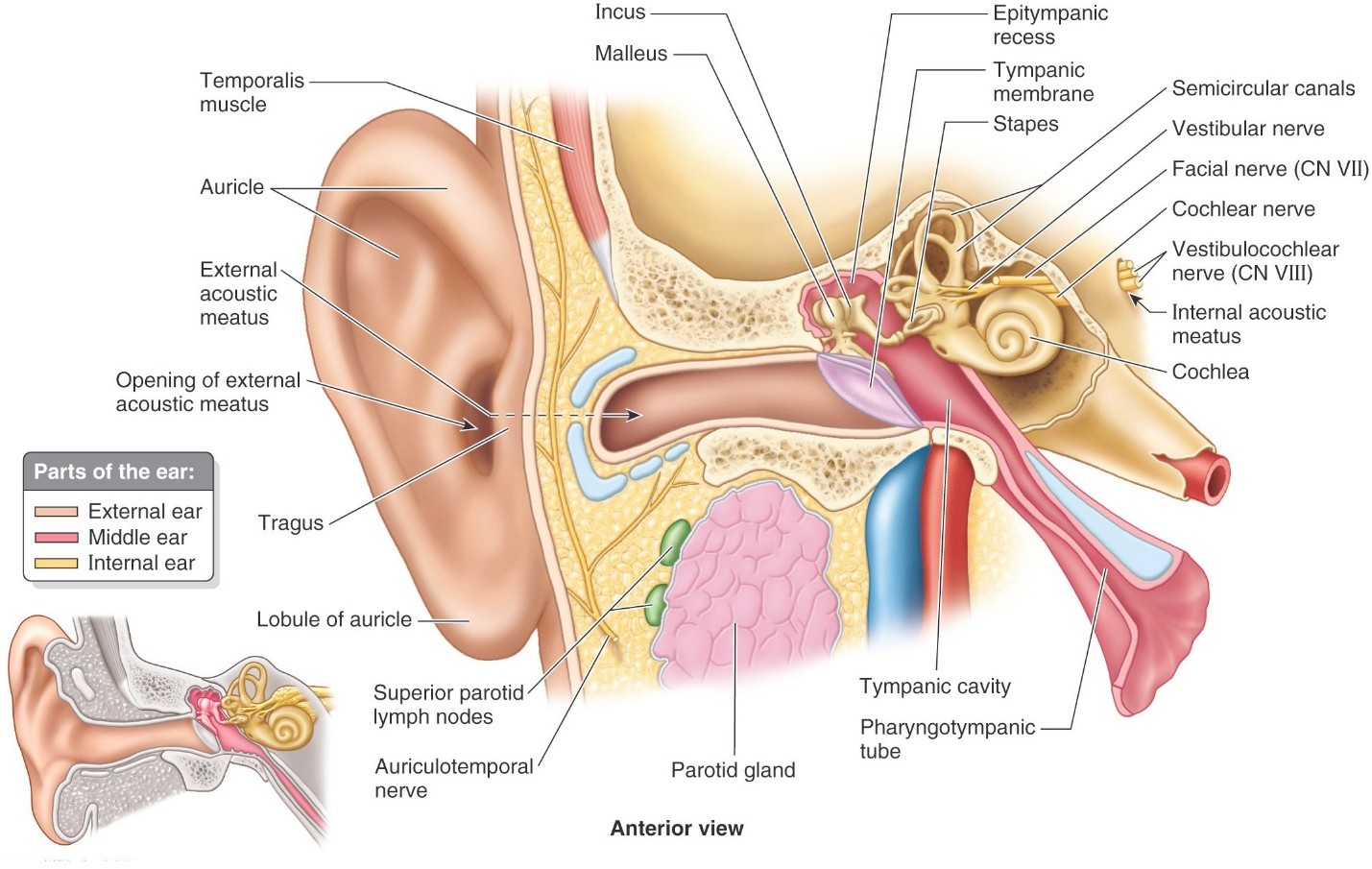
The ear is the part of the head that contains the structures associated with the special sensations of hearing and balance. For descriptive and functional purposes, anatomists and clinicians organize the ear into three parts: external, middle, and internal.
The ear has four functional mechanisms that allow us to hear and perceive sounds, and these mechanisms are related to the anatomic subdivisions of the ear.
Collecting sound waves
The external ear provides the parts for collecting sound waves and directing them into the head where they move the eardrum (tympanic membrane).
Amplifying sound
The middle ear contains tiny bones (auditory ossicles) that move when the eardrum moves, amplify the sound waves, and convert the movement of air into movement of fluid in the internal ear.
Transduction of vibrations into action potentials
The cochlea of the internal ear is a transducer that converts vibrations of fluid into action potentials in the cochlear nerve.
Transmission of action potentials to the brain
The cochlear part of the vestibulocochlear nerve (CN VIII) delivers the action potentials to the brain where sound it is perceived and interpreted.
External ear
Consists of:
The auricle (also called the pinna), which projects from the side of head in order to collect sound waves.
The external acoustic meatus, which directs the sound waves inside the head.
The tympanic membrane, separating the external acoustic meatus from the middle ear.
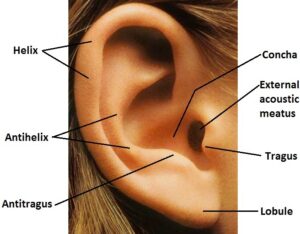
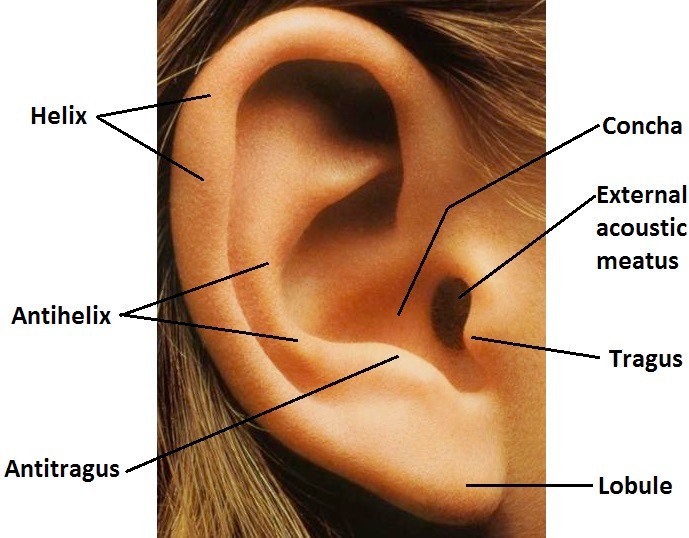
Auricle (pinna)
Figure 2. WIKIMEDIA COMMONS.
Consists of a core of elastic cartilage covered snuggly by thin skin.
The helix and antihelix are curved ridges that define the posterior margins of the auricle.
The concha is the central deep depression that communicates with the opening of the external acoustic meatus.
The tragus (Greek: goat, presumably because ear hairs resemble the beard on the chin of a goat) is the prominent projection just anterior to the opening of the external acoustic meatus.
The antitragus is a bump on the antihelix posterior to and opposite the tragus.
The lobule (ear lobe) is the fleshy inferior part of the auricle. It holds the distinction of being the only part of the auricle not supported by cartilage. It consists of skin and connective tissue.
Clinical correlation
If the skin and elastic cartilage become separated by hematomas (blood clots) due to chronic trauma—as occurs with boxers or wrestlers—the auricle can become distorted and wrinkled over time, a condition called cauliflower ear. Most of the auricle has little fat and connective tissue, so the ear is susceptible to frostbite.
External acoustic meatus
Figure 3.
Extends from the concha to the tympanic membrane.
The external acoustic meatus is not straight—it is curved in two planes:
When viewed from above it is S-shaped, with three parts.
The most lateral part is directed anteriorly (this is why you have the earpieces of a stethoscope pointed forward toward your nose when you place them in your ears).
The middle part is directed posteriorly.
The medial portion again turns anteriorly.
When viewed from the front, it is curved with a concavity facing downward.
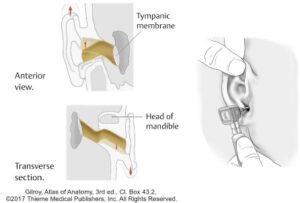
In adults
Due to the curvatures, clinicians viewing the tympanic cavity with an otoscope in adults must gently tug the auricle up and back to straighten the external acoustic meatus.
The lateral third of the meatus has a cartilage wall that is continuous with the cartilage of the auricle and it is lined by skin. The medial two-thirds of the meatus has a bony wall (tympanic portion of the temporal bone) lined by skin.
The skin lining the meatus contains hair follicles, sebaceous glands, and ceruminous glands (modified sweat glands). Ceruminous glands produce a brown, semisolid fatty/waxy substance called cerumen (ear wax!).
Tympanic membrane (eardrum)
The tympanic membrane (eardrum) is a three-layered oval structure that separates the external ear from the middle ear. It is attached to a ring of bone belonging to the tympanic part of the temporal bone. The external surface of the membrane is lined by skin; the internal surface is lined by a mucosa continuous with that of the tympanic cavity; while the central core of the membrane is a layer of connective tissue. The layers are thin, so the tympanic membrane is semi-transparent.
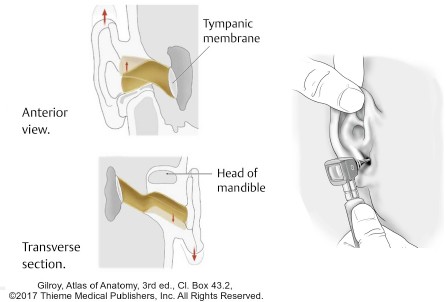
Since the medial third of the external acoustic meatus is directed anteriorly in the head, the tympanic membrane is positioned at an angle—it faces both forward and down.
The membrane is not flat; it is somewhat coned-shaped = the external surface is concave and the internal surface convex and bowed inward. The peak of the cone, called the umbo, is attached internally to the handle of the malleus, one of the tiny bones in the tympanic cavity. Superior to the umbo, the attachment of the tympanic membrane to the lateral process of the malleus produces visible creases called the mallear folds. Thus, the tympanic membrane attaches to the malleus in two places.
Sound waves are collected by the auricle and concentrated in the external acoustic meatus. The tympanic membrane moves in response to the sound waves in the air. Since the malleus is attached to the internal surface of the membrane, movements of the tympanic membrane produce movements in the tiny bones (ossicles) in the middle ear.
Clinical correlation
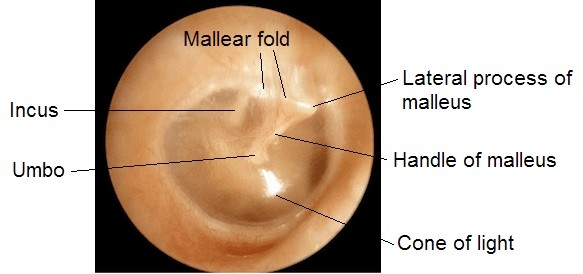
Examination of the tympanic membrane is done with an otoscope.
Figure 4. Otoscopic examination of normal tympanic membrane—lateral view.
When a healthy membrane is illuminated, it appears pearly gray and is transparent enough to allow the handle of the malleus and the long process of the incus to be seen on the other side. Due to its obliquity and concavity, a “cone of light” is usually produced by the otoscope in the anterior-inferior quadrant (5 o’clock position) of a healthy membrane.
Clinical correlation
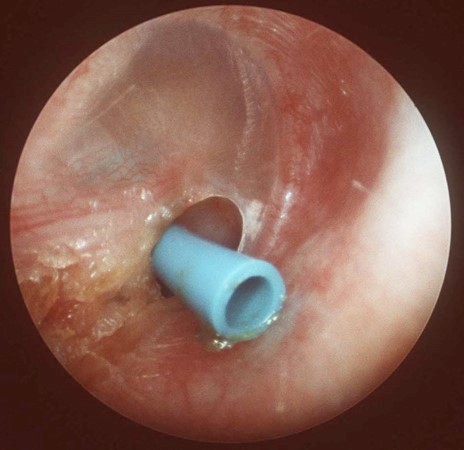
A surgical procedure called a myringotomy creates a tiny opening in the tympanic membrane to drain fluid or pus from the tympanic cavity due to otitis media. The membrane heals nicely afterwards.
Figure 5. Otoscopic view of myringotomy and ear tube.
In children with chronic middle-ear infections, myringotomy tubes (“ear tubes”) are placed in the tympanic membrane to ventilate the tympanic cavity.
Blood supply of external ear
Superficial temporal and posterior auricular arteries (both from the external carotid) supply the auricle.
Superficial temporal, posterior auricular, and deep auricular (from the maxillary) arteries supply the external acoustic meatus.
innervation of external ear
Auricle: Great auricular nerve (from the cervical plexus, C-2 and C-3) and auriculotemporal nerve (from V3). Small contributions in the concha are made by twigs from the facial and vagus nerves.
External acoustic meatus: Auriculotemporal nerve and the auricular branch of the vagus. Cleaning the external acoustic meatus may elicit a cough = thisis a vagal reflex and is explained by knowing that the vagus contributes sensory fibers.
Tympanic membrane: External surface is supplied by the auriculotemporal nerve and auricular branch of the vagus. Internal surface receives sensory innervation from the glossopharyngeal nerve.
Middle ear
Consists of the tympanic cavity and its contents:
Tympanic cavity, an air-filled space within the petrous portion of the temporal bone.
Three tiny bones called auditory ossicles.
Two tiny skeletal muscles that act on the ossicles.
Tympanic plexus of nerves.
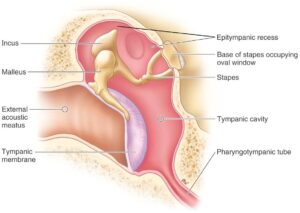
Tympanic cavity
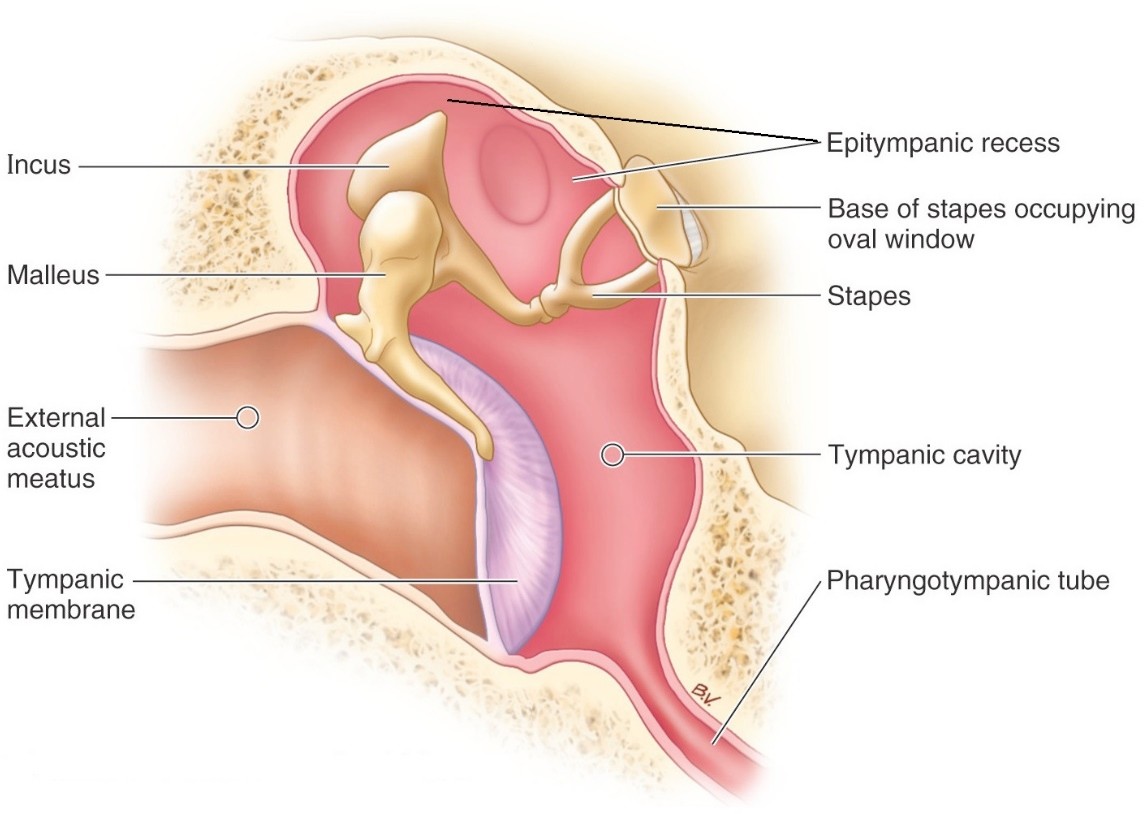
Figure 6. Coronal section—anterior view. CLINICALLY ORIENTED ANATOMY, FIGURE 7.116.
Separated from the external acoustic meatus by the tympanic membrane.
Lined with a mucous membrane, which also covers the internal surface of the tympanic membrane and the auditory ossicles.
Connected to the nasopharynx by the pharyngotympanic (Eustachian) tube.
The tympanic cavity is taller than the external acoustic meatus. The floor of the cavity is at the level of the inferior border of the tympanic membrane, but the roof rises well above it. This upper extension of the tympanic cavity is called the epitympanic recess, referred to by clinicians as the “attic”. This is the first part of the tympanic cavity seen when approached from a superior view in the dissecting lab.
Box visual analogy
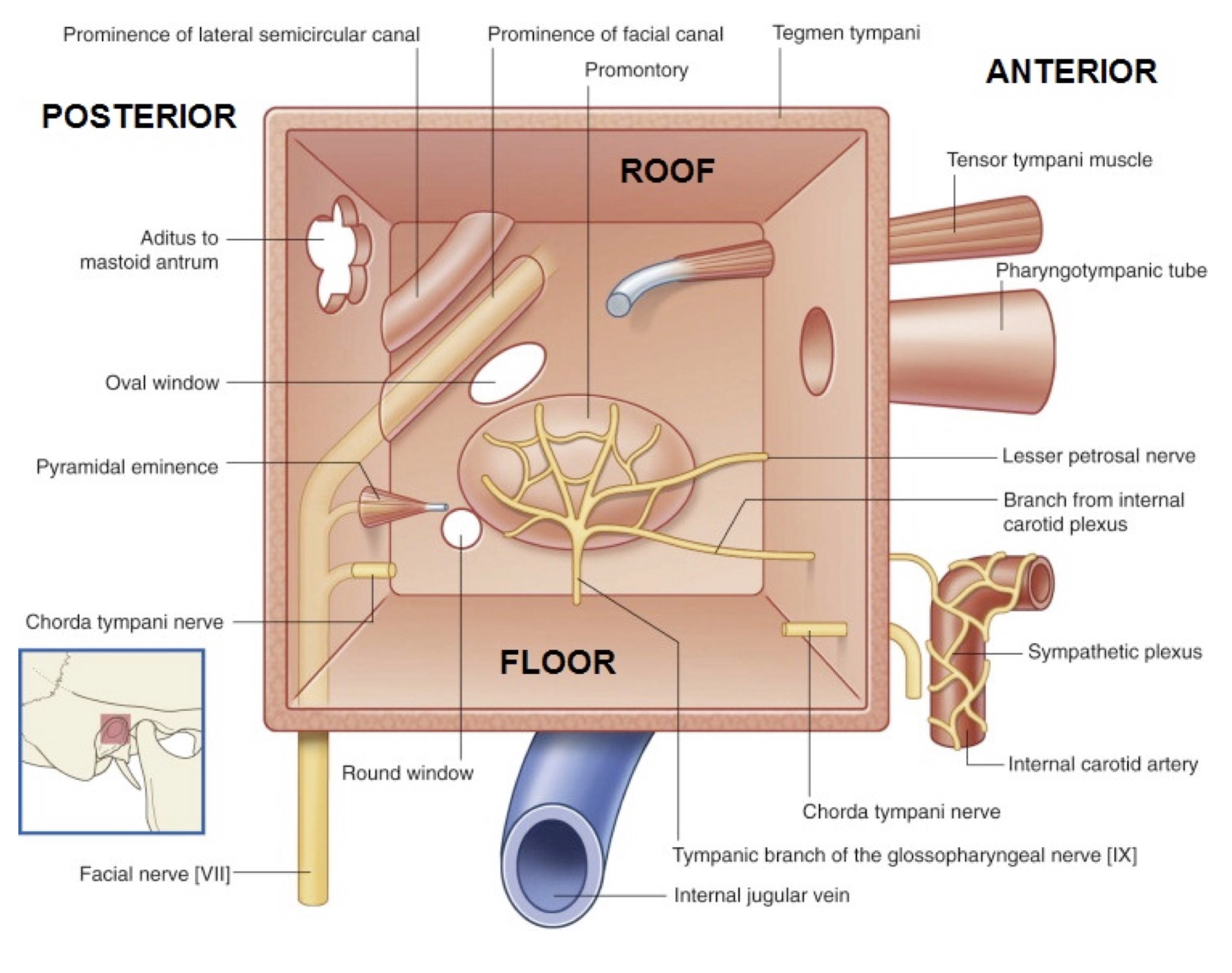
Figure 7. The tympanic cavity box. The tympanic membrane has been removed, so the viewer is looking into the box from lateral to medial. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.116.
Although the tympanic cavity is a narrow space whose long axis is parallel to the tympanic membrane, for descriptive and teaching purposes it is considered to be a BOX with anterior, posterior, medial, and lateral walls, a roof, and a floor.
Roof: A layer of bone called the tegmen tympani separates the tympanic cavity from the meninges and the temporal lobe of the brain in the middle cranial fossa above.
Floor: A plate of bone separates the tympanic cavity from the internal jugular vein.
Anterior wall (carotid wall): Bone here separates the tympanic cavity from the internal carotid artery. Two canals open on the anterior wall:
The lower opening leads into the pharyngotympanic tube (Eustachian tube), which runs anteriorly and medially from the tympanic cavity to the nasopharynx. This tube is normally closed, but when it opens (facilitated by yawning or swallowing) air can pass through, and this aerates the tympanic cavity and equalizes pressure with the atmosphere. (Ears go “pop!”)
The upper opening connects to a bony canal filled with the tensor tympani muscle.
Posterior wall (mastoid wall): Has two features:
Superiorly is an opening called the aditus to the mastoid antrum. The mastoid antrum is a common chamber that communicates with many small mucosa-lined cavities called mastoid air cells. The antrum and air cells are within the mastoid process of the temporal bone.
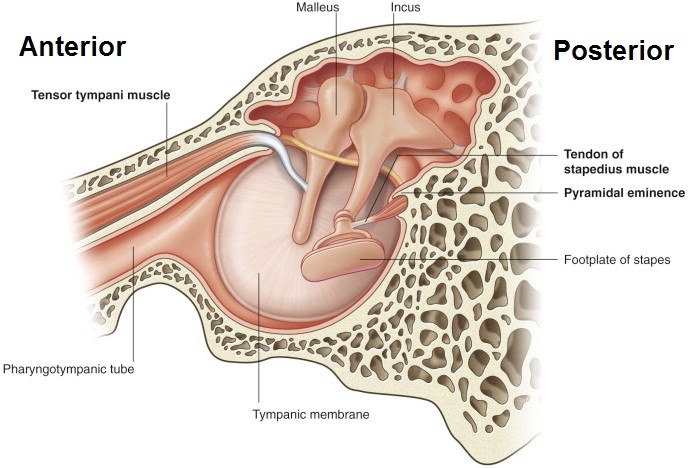
Below the aditus is a small, hollow, cone-shaped projection called the pyramidal eminence, from whose apex emerges the tendon of the stapedius muscle.
Lateral wall: Formed mainly by the tympanic membrane. The chorda tympani nerve crosses the lateral wall, passing between the handle of the malleus and the long process of the incus.
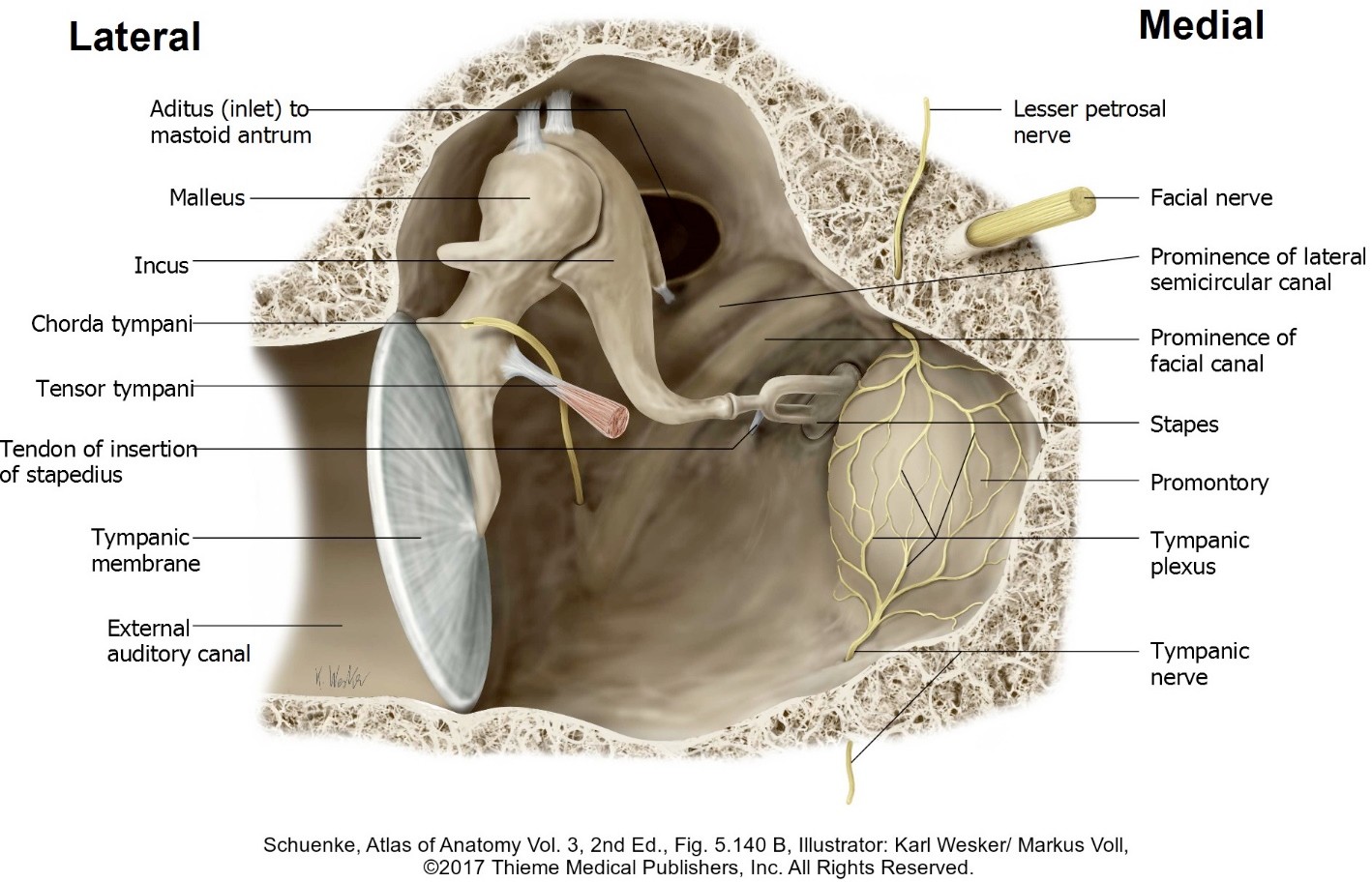
Medial wall: A thin layer of bone separates the tympanic cavity from the internal ear.
The most prominent feature is a bulge called the promontory, produced by the basal (first) turn of the cochlea (part of the internal ear).
On the surface of the promontory is the tympanic plexus of nerves.
Above and behind the promontory is an opening into the internal ear, the oval window. The footplate of the stapes fits into the oval window.
Below the promontory is a second opening into the internal ear, the round window. The round window is closed by the secondary tympanic membrane.
On the upper medial wall near the roof is a bony ridge, the prominence of the facial canal. It contains the facial nerve. Only a thin layer of bone separates the facial nerve from the mucosa of the tympanic cavity.
Figure 8. Relationships of the tympanic cavity. Superior view. The petrous temporal bone is transparent.
innervation of the tympanic cavity
The mucosa is supplied by the tympanic branch of the glossopharyngeal nerve. Thus, pain from a middle ear infection is carried in CN IX.
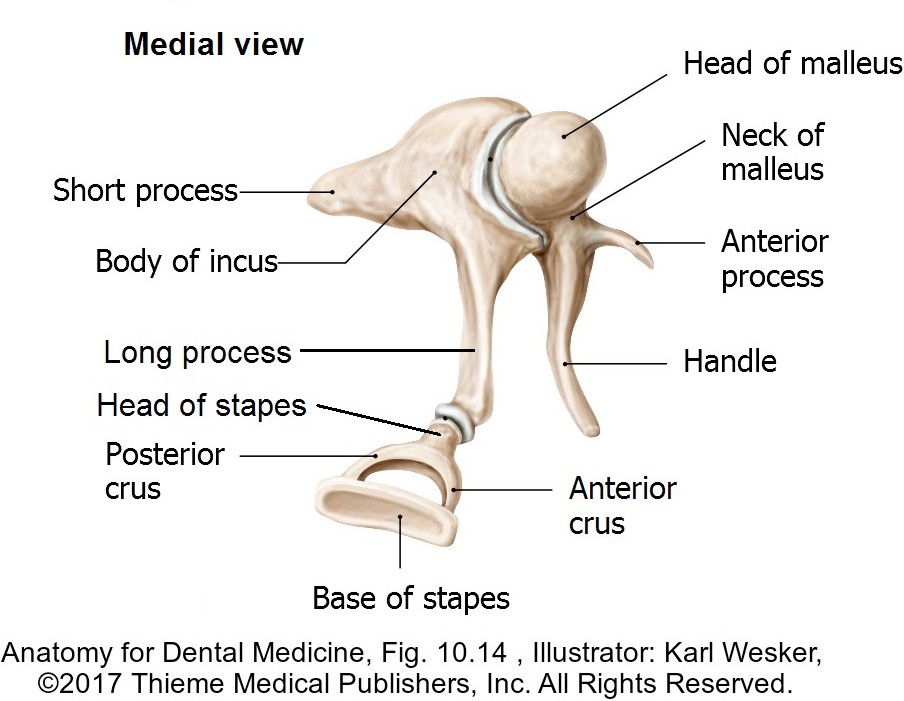
Three tiny bones extend across the tympanic cavity, covered in mucous membrane, from the tympanic membrane to the oval window. From lateral to medial these are the malleus, incus, and stapes.
Body is rounded and articulates anteriorly with the head of the malleus.
Long process projects inferiorly, behind and parallel to the handle of the malleus (where its shadow can sometimes be seen on otoscopic examination). Articulates with the head of the stapes.
Short process projects posteriorly and is attached to the posterior wall of the tympanic cavity by a ligament.
Head is very small and articulates with the long process of the incus—receives the attachment of the stapedius muscle.
Two limbs attach the neck to the base (footplate).
The edges of the base attach to the margins of the oval window by a ring of connective tissue called the annular ligament.
Given that the tympanic membrane has a much larger surface area than the base of the stapes, the ossicles act as levers to amplify the movements of the tympanic membrane (sources vary on this, but the amplification may be as much as 20 times), so that a substantial force can be produced at the oval window by smaller movements of the tympanic membrane.
Muscles of the ossicles
Figure 11. Tensor tympani and stapedius muscles. Lateral wall of tympanic cavity is seen—viewer is looking from medial to lateral. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.120.
The tensor tympani and stapedius muscles attenuate (reduce) the movements of the ossicles (and tympanic membrane) in response to loud noises, which might otherwise cause damage to the delicate sensory apparatus of the internal ear.
Tensor tympani
Origin
From the bony wall of its canal (opens on the anterior wall of the tympanic cavity) as well as from the cartilage of the pharyngotympanic tube.
Insertion
Its tendon turns around a bony shelf (pulley) to insert on the handle of the malleus.
Action
Pulls the stapes posteriorly and tightens up the annular ligament to prevent excessive movement of this tiny bone.
innervation
A branch of the mandibular nerve (V3).
Stapedius
Origin
From the pyramidal eminence on the posterior wall of the tympanic cavity.
Insertion
Near the head of the stapes.
Action
Reduces the vibrations of the malleus and movements of the tympanic membrane by pulling the malleus and tympanic membrane medially (thus tensing the tympanic membrane).
innervation
A branch from the facial nerve.
Clinical correlation
Facial nerve dysfunction (such as Bell's palsy) can paralyze the stapedius, leaving the patient with hypersenitivity to sound (hyperacusis).
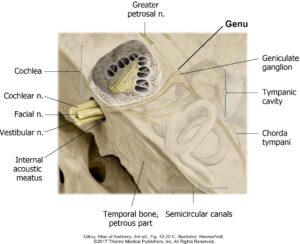
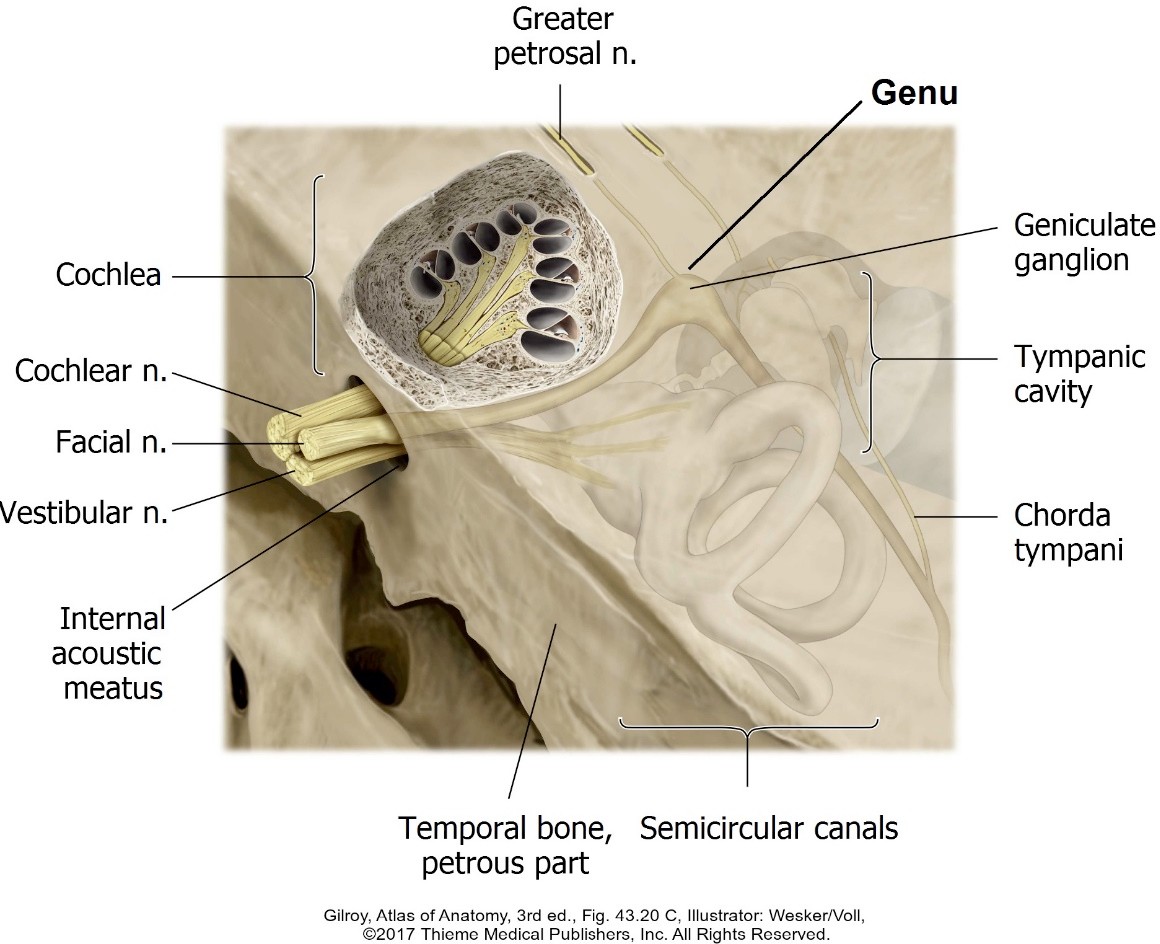
Figure 12. Course of the facial nerve. The petrous temporal bone has been rendered transparent. The view is looking from medial to lateral.
Leaves the cranial cavity and enters the petrous part of the temporal bone through the internal acoustic meatus along with the vestibulocochlear nerve (CN VIII). At the lateral end of the meatus, the facial nerve enters the facial canal.
Within the facial canal, the nerve passes between the cochlea and vestibule, which are both parts of the internal ear.
Lateral to the cochlea, the facial canal turns posteriorly, producing a sharp bend in the nerve = the genu (Latin = “knee,” because it is bent like a flexed knee). This is the location of the sensory ganglion of the facial nerve (geniculate ganglion).
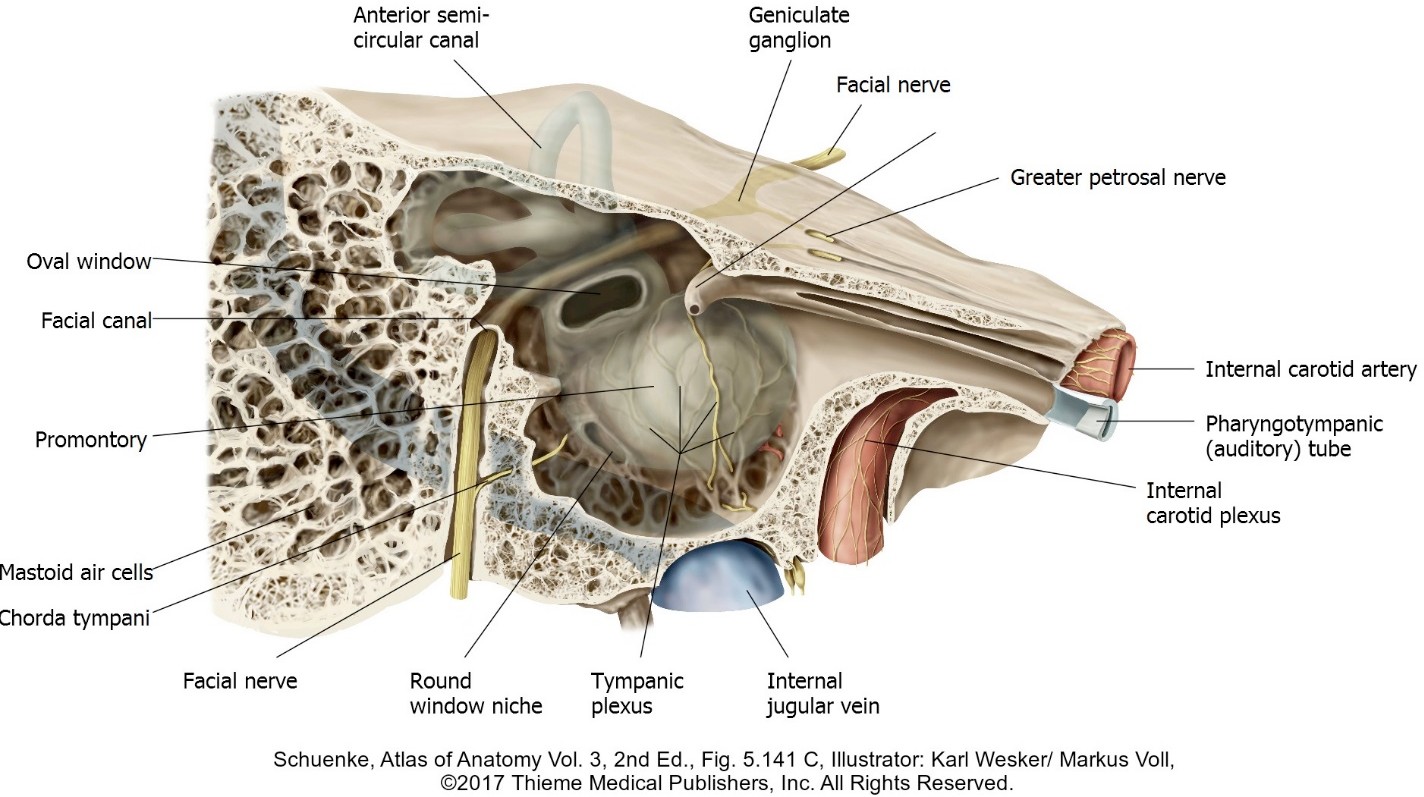
Distal to the genu, the facial nerve moves posteriorly in the facial canal midway between the tympanic cavity and the cochlea. Here the bony prominence of the facial canal is located in the upper medial wall of the tympanic cavity.
Posterior to the tympanic cavity, the facial canal bends inferiorly and descends between the tympanic cavity and mastoid air cells to the stylomastoid foramen, where it exits the skull and enters the parotid gland.
Arises from the facial nerve in the facial canal just above the stylomastoid foramen and runs superiorly through the temporal bone to enter the tympanic cavity from its posterior wall.
Runs across the internal surface of the tympanic membrane from posterior to anterior, where it passes between the handle of the malleus and the long process of the incus.
It leaves the tympanic cavity through a tiny slit in its anterior wall, the petrotympanic fissure, to enter the infratemporal fossa, where it joins the lingual nerve.
Chorda tympani carries taste information from the anterior 2/3 of the tongue (special sensory) and preganglionic parasympathetic fibers to the submandibular ganglion (visceral motor).
Branches from the genu of the facial nerve and travels anterior.
Leaves the petrous temporal bone through a bony fissure and enters the middle cranial fossa. Traverses the middle cranial fossa under the dura, then enters the foramen lacerum.
Carries preganglionic parasympathetic fibers to the pterygopalatine ganglion. Postganglionic fibers innervate the lacrimal gland and mucous glands in the nasal cavity.
Greater petrosal also carries taste fibers from taste buds in the palate.
Figure 13. Course of the facial nerve. The medial wall of the tympanic cavity is rendered transparent. The view is looking lateral to medial.
Located atop the promontory on the medial wall of the tympanic cavity.
Nerve fibers derived from these nerves form the tympanic plexus:
Tympanic nerve (Jacobsen’s nerve): Arises from the glossopharyngeal nerve in the jugular foramen and enters the tympanic cavity through its floor to join the tympanic plexus. The tympanic nerve carries sensory fibers that innervate the mucosa of the tympanic cavity and preganglionic secretomotor fibers that form the lesser petrosal nerve.
Postganglionic sympathetic fibers from the internal carotid plexus enter the tympanic cavity through its anterior wall and join the plexus. These supply smooth muscle in blood vessels.
These nerve fibers leave the tympanic plexus:
Sensory branches (from the tympanic nerve of CN IX) supply the mucosa of the tympanic cavity, inner aspect of the tympanic membrane, mastoid air cells, and the pharyngotympanic tube.
The lesser petrosal nerve leaves through the roof of the tympanic cavity. It contains preganglionic parasympathetic fibers from CN IX that synapse in the otic ganglion in the infratemporal fossa. From here, postganglionic parasympathetic fibers innervate the parotid gland.
Figure 14. Cut away view of tympanic cavity. The view is looking from anterior to posterior.
Clinical correlation
Infection of the tympanic cavity is called otitis media. It produces bulging, redness, and opacity of the tympanic membrane.
The tympanic cavity requires constant aeration for normal function. Infection and swelling of the pharyngotympanic tube blocks the source of air, creating a vacuum in the tympanic cavity and conditions favorable for growth of pathogens.
The pharyngotympanic tube in an infant is about half the length of the adult and is oriented more horizontally. Because of this, otitis media is more common in children.
Clinical correlation
Serious complications of otitis media can produce infections in the mastoid air cells (mastoiditis)—or worse, infections could spread through the thin walls of the tympanic cavity to the meninges in the cranial cavity (meningitis) or enter the blood stream by invading the nearby sigmoid venous sinus.
Internal ear
Optional reading: Here we will only discuss the basics of internal ear anatomy to get you up to speed in preparation for more heavy-duty information in your neuroscience course.
The internal ear contains the organs specialized for:
Reception of sound.
Detection of the position and movement of the head—information needed to maintain balance and equilibrium.
The internal ear is made up of a series of cavities carved out of the petrous part of the temporal bone (bony labyrinth) containing a network of membrane-lined ducts and sacs (membranous labyrinth).
Bony labyrinth
Interconnected hollow cavities within the petrous temporal bone lined by a periosteum and filled with a fluid called perilymph.
Components of the bony labyrinth
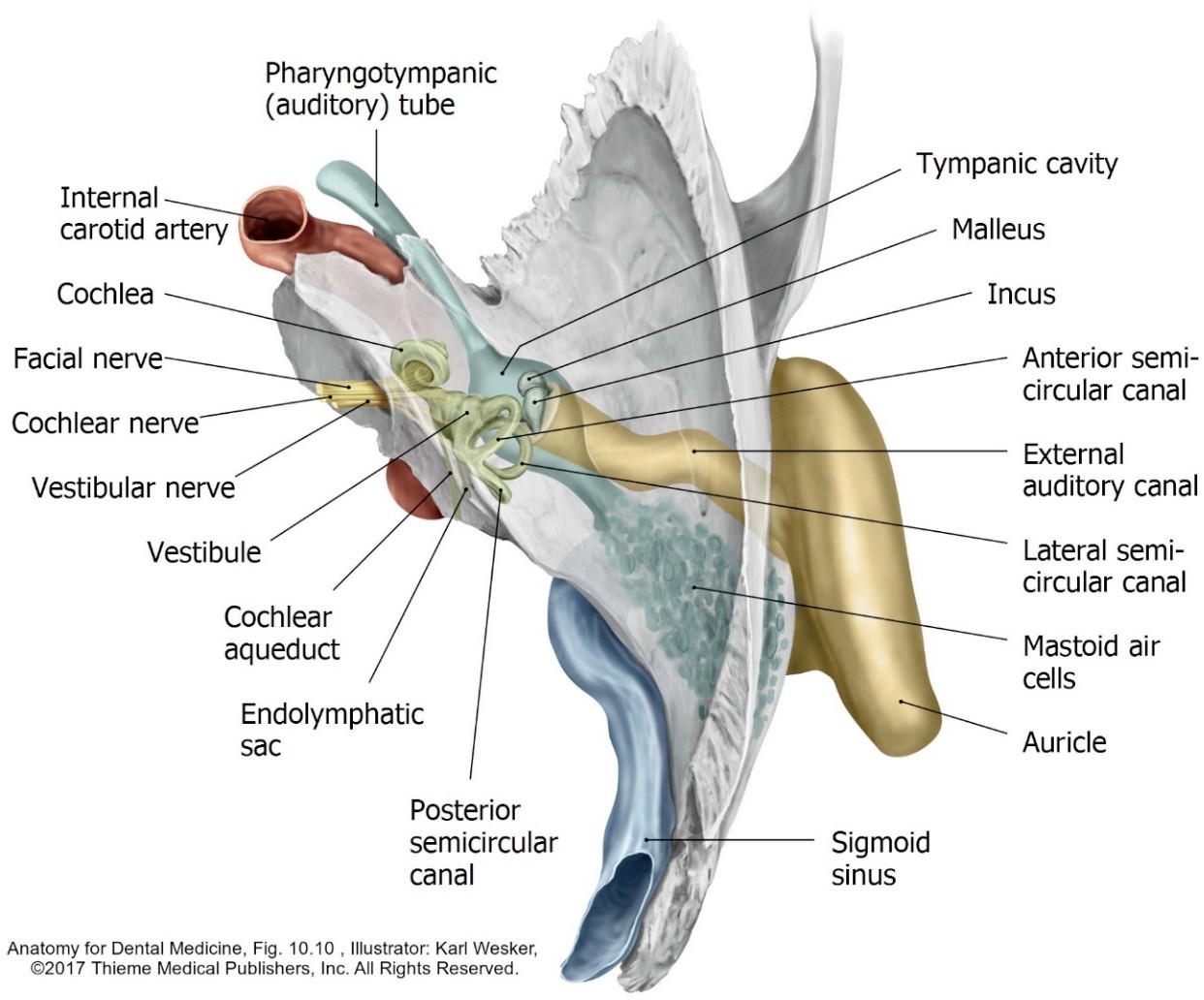
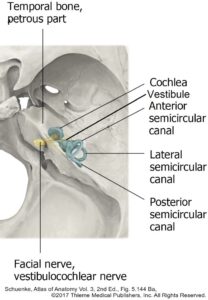
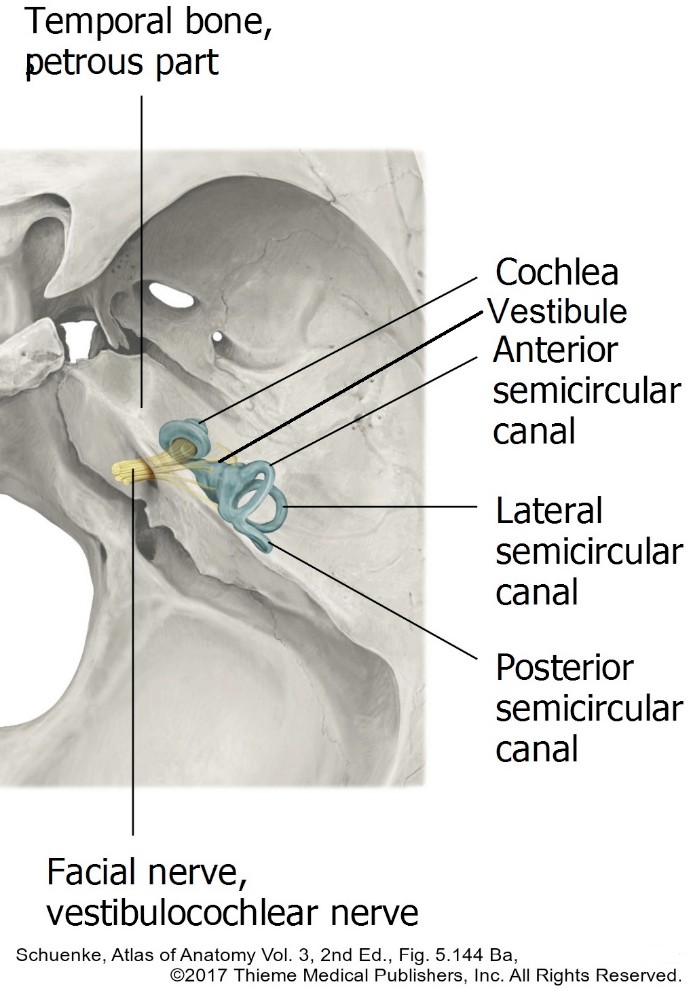
Figure 15. Position of bony labyrinth within the petrous part of the temporal bone.
Three semicircular canals (anterior, posterior, and lateral), oriented at right angles to one another.
Vestibule: A spherical cavity with the oval window in its lateral wall. The vestibule communicates with the semicircular canals and the cochlea.
Cochlea: A spiral canal shaped like a snail’s shell. It makes two and one-half turns around a central bony core called the modiolus. The round window is located in the lateral wall of the base (first turn) of the cochlea.
Membranous labyrinth
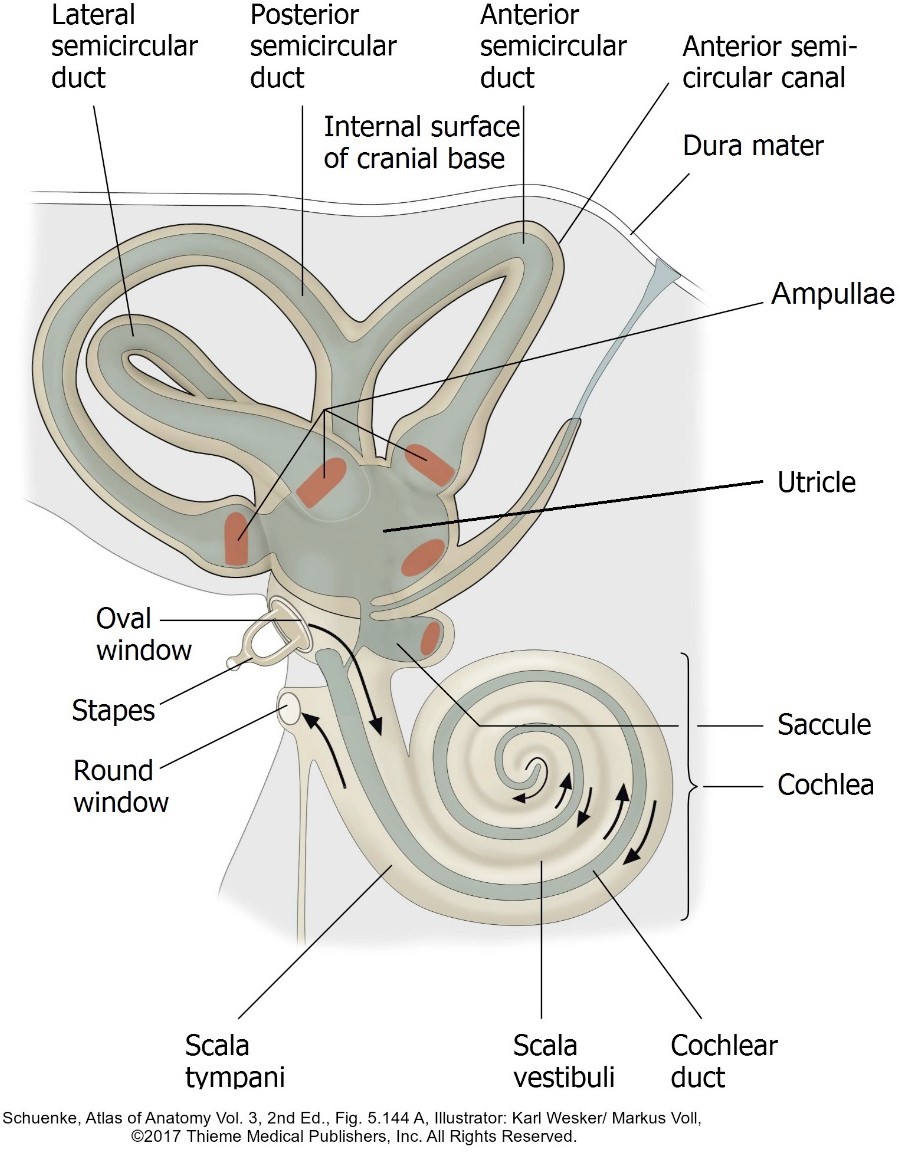
Figure 16. The parts of the membranous labyrinth shown within the bony labyrinth.
Interconnected series of ducts and sacs constructed of dense connective tissue and lined internally by an epithelium. The membranous labyrinth is suspended within the bony labyrinth and separated from its bony walls by the perilymph.
The membranous labyrinth is filled with a fluid called endolymph.
Components of the membranous labyrinth
Three semicircular ducts lie inside the semicircular canals. Where the ducts meet there are enlargements called ampullae. Receptors within the ampullae monitor angular acceleration of the head (side-to-side head rotation).
Utricle and saccule are within the vestibule of the bony labyrinth. Receptors within the utricle and saccule monitor
Static equilibrium (detecting the orientation of the head with respect to the ground when the head is stationary)
Linear acceleration (sensing when the body moves in a straight line).
Stimulation of receptor cells in the vestibular organs mentioned above produces action potentials in neurons of the vestibular division of the vestibulocochlear nerve (CN VIII). These are bipolar neurons with cell bodies in the vestibular ganglion (Scarpa’s ganglion), located within the internal acoustic meatus.
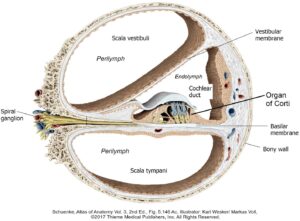
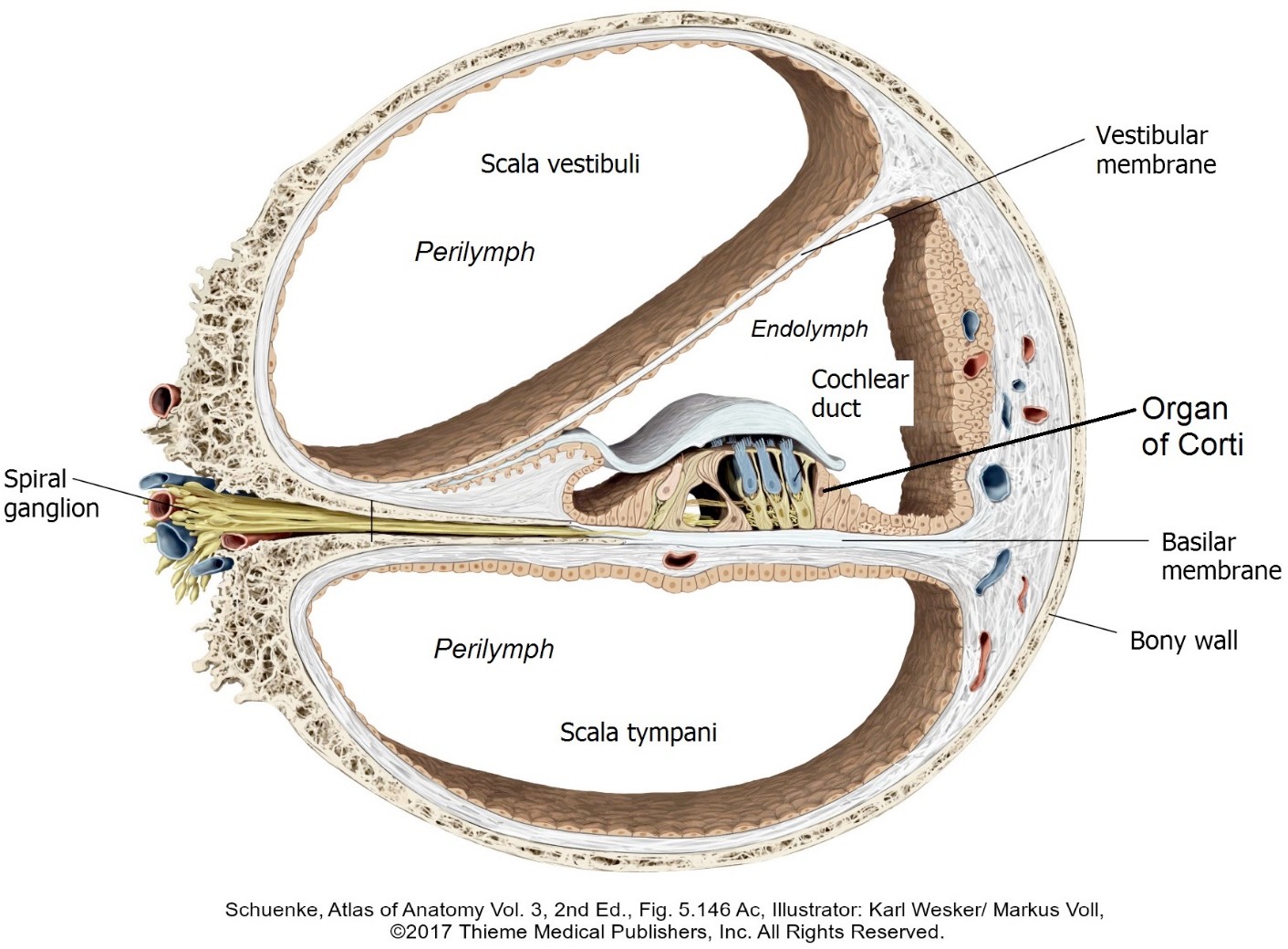
Figure 17. Cross section of one turn of the cochlea. The scala vestibuli and tympani belong to the bony labyrinth, while the cochlear duct is part of the membranous labyrinth.
The cochlear duct occupies a central position within the bony cochlea. It has a roof called the vestibular membrane and a floor called the basilar membrane. Because of its central location, the cochlear duct (containing endolymph) subdivides the cavity of the cochlea into two perilymph- filled channels: the scala vestibuli above and the scala tympani below. The cochlear duct contains the spiral organ (organ of Corti), where the special receptor cells for hearing are housed.
Stimulation of receptors in the Organ of Corti produces action potentials in neurons of the cochlear division of the vestibulocochlear nerve (CN VIII). These are bipolar neurons with cell bodies in the cochlear ganglion (spiral ganglion), located in the modiolus.