The vertebral column (“backbone” or “spine”) consists of a series of bones, the vertebrae, firmly connected together by joints and ligaments. The vertebral column is the “axis” of the body—the major component of the axial skeleton—which owes it segmented construction to the embryonic notochord and paraxial mesoderm. A comprehensive description of the functional anatomy of the vertebral column is beyond the scope of our course, so we will focus on its major structural components, regional characteristics, and relationship to the spinal cord.
Figure 5.1
Functions of the vertebral column
Protection of the spinal cord and spinal nerves
Supports the head and trunk
Transmits the weight of the trunk to the lower limbs via the pelvic skeleton
Provides attachments for postural muscles and limb muscles
Provides both a rigid and flexible axis for the body
Provides a pivot point for the head
Regions of the vertebral column
The vertebral column has 5 named regions:
cervical
thoracic
lumbar
sacral
coccygeal
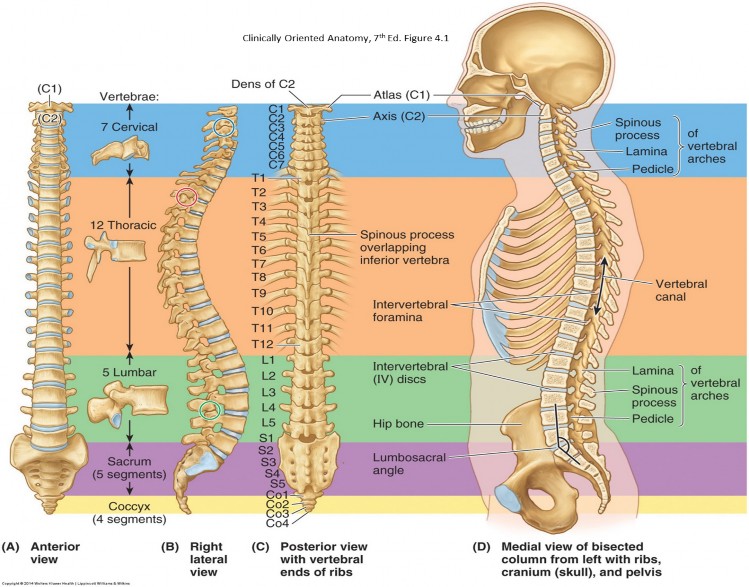
Each region has characteristic curvatures and specific features. The cervical, thoracic, and lumbar regions each have individual bones = 7 cervical vertebrae, 12 thoracic vertebrae, and 5 lumbar vertebrae. The sacrum is composed of five fused vertebrae. The first coccygeal vertebra is usually a separate bone, whereas the rest of the coccyx is formed by 3 fused vertebrae. Thus, is it generally agreed upon that the vertebral column is composed of 33 vertebral elements (individual vertebrae + fused vertebrae).
Curvatures of the vertebral column
Figure 5.2 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 162.
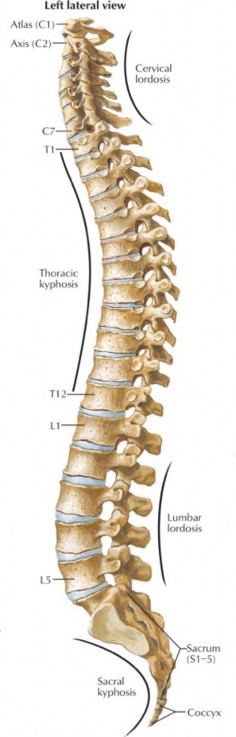
In the fetus, the entire vertebral column is curved in one direction: backward, with a concavity directed anteriorly (“fetal position”). Fully developed humans have four curvatures—one each in the cervical, thoracic, lumbar, and sacral regions.
The thoracic and sacral curvatures are curved backward, with concavities directed anteriorly, in the same direction as the original fetal curvature. Thus they are referred to as primary curvatures. A curving backward of the spine, as seen in the thoracic and sacral regions, is technically known as a kyphosis (Greek = hump).
The cervical and lumbar curvatures are curved forward, with concavities directed posteriorly. These curves are acquired after birth, so they are known as secondary curvatures. A curving forward of the spine, as seen in these regions, is known as a lordosis (Greek = bent backwards). The cervical lordosis is acquired during the first year of life, as a child learns to hold the head up. The lumbar lordosis develops later when a child learns to stand upright.
The curvatures are important for balance, flexibility, and the distribution of forces in the spine. All the curvatures together align the spine along the body’s center of gravity. The lordotic curves support weight better = the cervical lordosis supports the head and the lumbar lordosis supports the head and trunk above it.
Excessive curvatures can be a problem. Excessive thoracic kyphosis produces a “hunch back,” while too much lumbar lordosis leads to a “sway back.”
Abnormal lateral curvature of the spine is called scoliosis.
Features of a typical vertebra
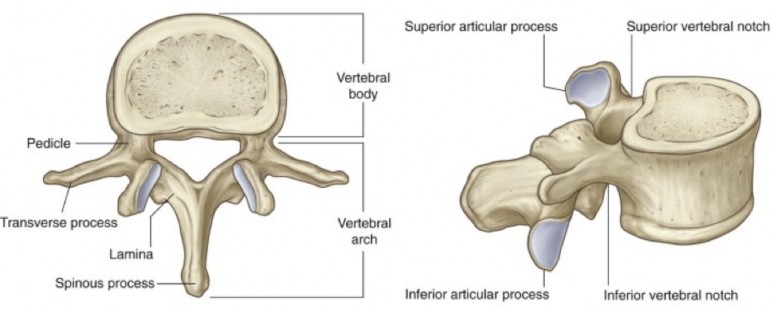
Vertebrae are made of spongy bone surrounded by a layer of compact bone. In all regions of the spine, vertebrae have two basic parts: a body and an arch.
Figure 5.3 GRAY’ S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.19.
The rounded, bulky, anterior part. Their superior and inferior surfaces are flat. Adjacent vertebral bodies are joined together by intervertebral discs.
2 pedicles: Extend backward from the body. Above and below the pedicles are superior and inferior vertebral notches. When two vertebrae are articulated, adjacent superior and inferior notches create an intervertebral foramen. These transmit spinal nerves.
2 laminae: Continue backward from the pedicles and fuse in the midline.
The pedicles and laminae surround a circular opening in the center of the vertebra, posterior to the vertebral body. This is the vertebral foramen. All the vertebral foramina together produce the vertebral canal within the spine.
Spinous process: Extends posteriorly from the union of the laminae.
Transverse processes (2): Extend laterally from the junction of the pedicle and lamina.
Articular processes (4): Extend upward and downward from the junction of the pedicle and lamina. Superior and inferior articular processes of adjacent vertebrae articulate to produce a “facet” joint.
Regional characteristics of vertebrae
Cervical region
Cervical vertebrae (7)
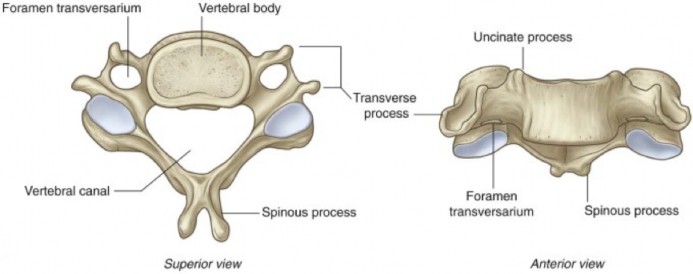
What sets these vertebrae apart from the other regions is the presence of a hole in their transverse processes = the transverse foramen (foramen transversarium)—this transmits the vertebral artery to the skull.
Cervical spinous processes are bifid (forked).
Most are covered by the thick nuchal ligament in the posterior neck, so they cannot be palpated.
C-7 spinous process is prominently visible and easily palpable; it is known as vertebra prominens.
Figure 5.4 Typical cervical vertebra. GRAY’ S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.20.
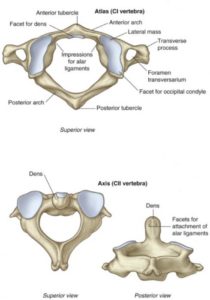
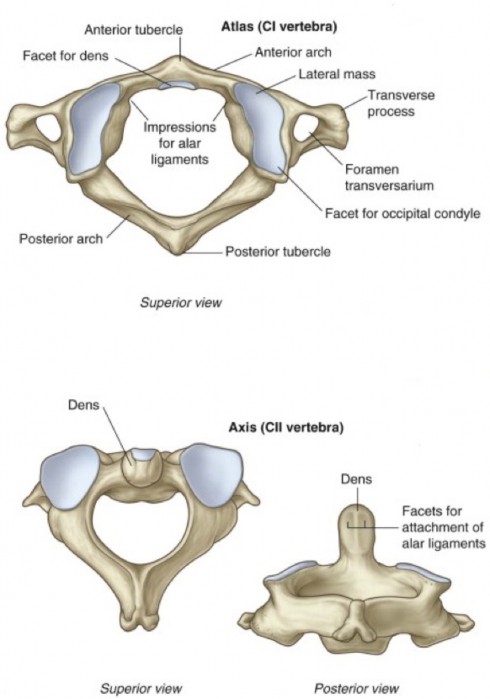
Figure 5.5 Atlas and axis. GRAY’ S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.20.Special cervical vertebrae:
Atlas (C-1): Articulates with the condyles of the skull; it has no body and there is no intervertebral disc between C-1 and C-2.
Atlanto-occipital joints: Between C-1 and the skull, allows flexion and extension of the head, as in nodding the head “yes.”
Axis (C-2): Its body is extended upwards, forming a nipple-like elevation that passes through the “donut hole” opening of C-1. This process is called the dens (as in “tooth”). Developmentally, it is the displaced body of C-1.
Atlanto-axial joint: Formed between C-1 and C-2: allows for rotation of the head, as in shaking the head “no.”
Thoracic region
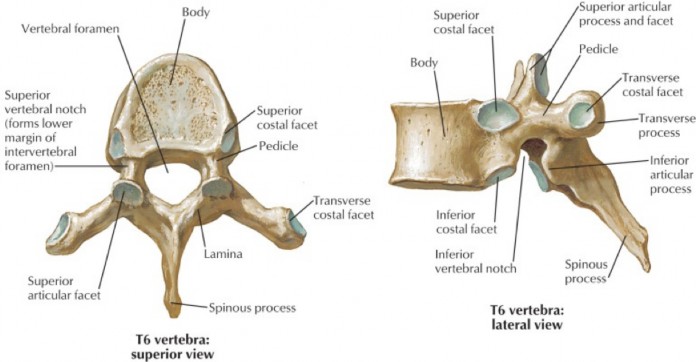
Thoracic vertebrae (12)
Thoracic vertebrae are distinguished by their association with ribs. Developmentally, the primordial elements that form the transverse processes elongate in this region to also form separate bones = the ribs.
All thoracic vertebrae articulate with at least one rib. Consequently, they have smooth articulating surfaces (costal facets) on their vertebral bodies and transverse processes where the ribs attach. These mark the locations of the costovertebral and costotransverse joints.
The bodies of thoracic vertebrae progressively enlarge from the 1st to the 12th.
They have long, slender, inferiorly angled spinous processes that overlap adjacent vertebrae. This makes palpation of thoracic spinous processes and counting vertebrae somewhat difficult in this region.
Figure 5.6 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 163.
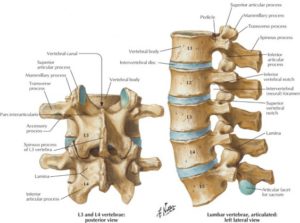
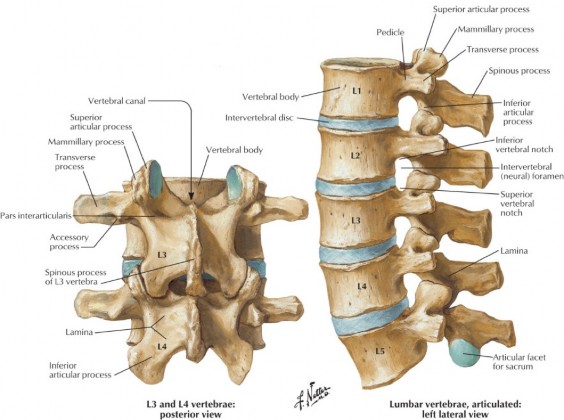
Figure 5.7 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 164.Lumbar region
The gap between laminae in adjacent lumbar vertebrae is very large compared with other regions. This gap gets even larger during spine flexion,allowing for a needle to be passed through this space to penetrate ligaments and enter the subarachnoid space to obtain cerebrospinal fluid—a procedure known as lumbar puncture.
Long, thin transverse processes are the embryonic equivalent of ribs.
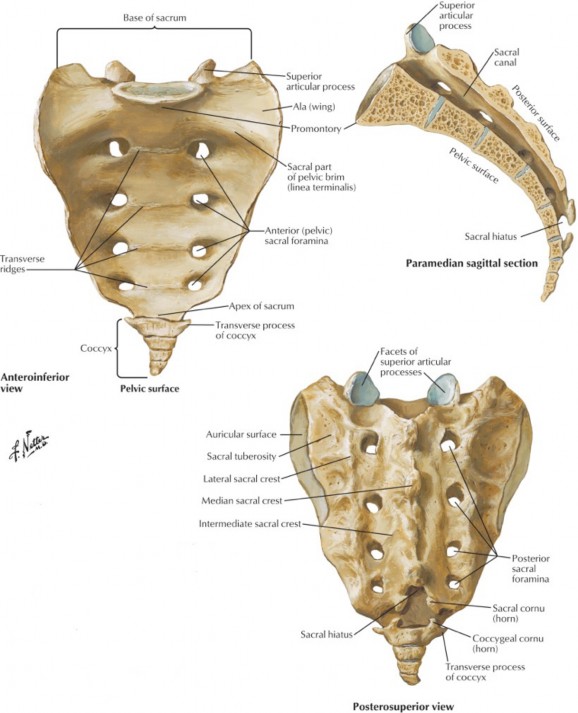
Figure 5.8 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 166.Sacral region
Sacrum (five vertebrae fused to form one bone)
Its five segments are still recognizable because of the transverse ridges (lines of fusion) visible on the anterior surface.
Wedged between the two hip bones—the sacrum functions to transmit the weight of the body above to the hip bones and lower limbs.
The anterior surface of the first sacral vertebra produces a prominent ridge that juts forward—this is the sacral promontory.
Anterior sacral foramina (8 holes on the anterior surface) transmit the ventral rami of S-1 to S-4 spinal nerves.
Posterior sacral foramina (8) transmit the dorsal rami of S-1 to S-4.
The core of the sacrum is hollow—this the sacral canal, the continuation of the vertebral canal from the lumbar region. It contains the cauda equina and associated meninges. The sacral canal terminates below as an opening = the sacral hiatus. It transmits the dorsal and ventral rami of S-5 and the coccygeal (Co-1) spinal nerves. Caudal epidural injections to treat sacral nerve root impingements are done here.
Coccyx (“tail bone”): The first coccygeal vertebra is usually separate—it articulates with the sacrum. The last three coccygeal vertebrae are fused into one piece.
Intervertebral foramina
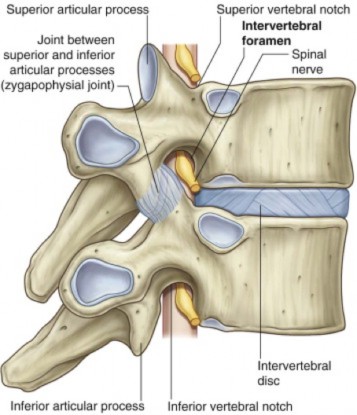
Figure 5.9 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.12.
Intervertebral foramina are formed laterally between adjacent vertebrae. They transmit spinal nerves and vessels out of and into the vertebral canal. The boundaries of each IV foramen are:
Superior and inferior: Superior and inferior notches of adjacent pedicles
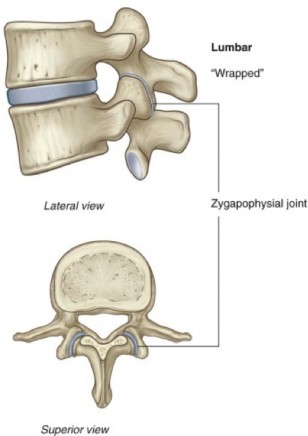
Posterior: Facet (zygapophyseal) joints between adjacent articular processes
Anterior: Intervertebral disc
Clinical correlation
Any pathological process that occludes or reduces the size of the intervertebral foramen (such as bony growth/stenosis or herniated vertebral disc) could affect the function of the spinal nerve. This condition is called radiculopathy. Symptoms can include muscle weakness and skin numbness/paresthesia. The site of injury is the intervertebral foramen, but the symptoms “radiate” to the parts of the body served by the particular nerve root affected.
Vertebral canal
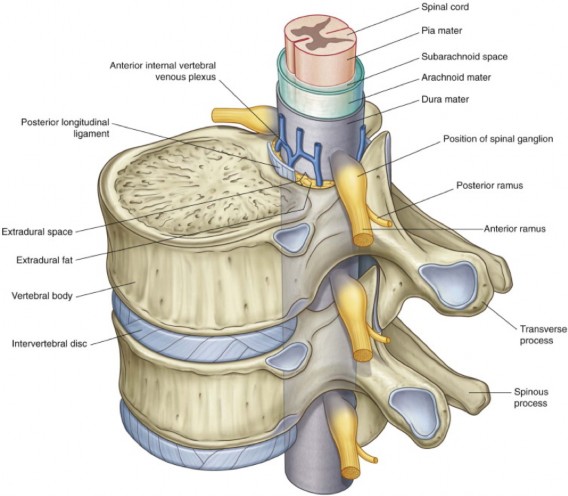
Figure 5.10 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.8.
The passageway in the center of the spine between vertebral bodies and arches is the vertebral canal. It is continuous above with the foramen magnum of the skull and ends below at the sacral hiatus. This contains the spinal cord and spinal meninges, as well as the epidural space containing fat and blood vessels.
Joints of the vertebral column
Joints of vertebral bodies
Intervertebral (IV) joints are a type of joint classified as a symphysis (the union of two bony elements by fibrocartilage). In this case, the bony elements are the vertebral bodies joined together by an intervertebral (IV) disc.
IV discs have two functions:
To resist the movements of vertebrae on one another
To absorb and dissipate forces transmitted along the vertebral column.
IV discs account for about 25% of the height of the vertebral column.
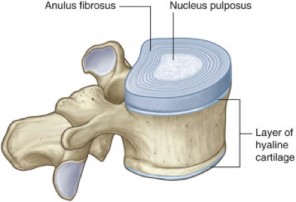
Two primary parts of an IV disc:
Outer annulus fibrosis: Many circular layers of collagen and fibrocartilage—these are arranged in sheets, and each sheet is oriented obliquely such that it criss-crosses the other sheets, giving the annulus super strength.
Inner nucleus pulposus: Gel-like consistency, highly hydrated (> 80% water), with scattered cells. Many of the cells are derived from the embryonic notochord. The nucleus pulposus absorbs water, but loses it when compressed. This is why an individual gains height at night—then loses it during the day.
Figure 5.11 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.28.
Figure 5.12 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.27.
Clinical correlation
Degeneration of the annulus fibrosis can lead to its rupture. If this happens, the nucleus pulposus can protrude through the opening—known as a disc herniation. A postero-lateral herniation is most common, owing to the annulus being relatively thin here and lacking support from the longitudinal ligaments. In the upper regions of the spine, a postero-lateral disc herniation affects the spinal nerve passing through the intervertebral foramen at the level of the herniation, because the disc is directly in line with the center of the intervertebral foramen.
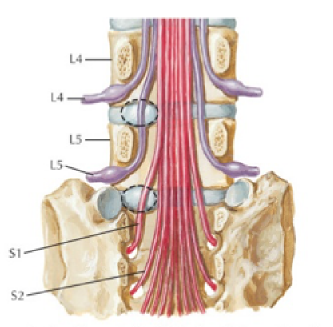
Figure 5.13 Lumbar disc protrusion (dashed ovals) does not usually affect nerve exiting above disc. Lateral protrusion at disc level L4–5 affects L5 spinal nerve, not L4 spinal nerve. Protrusion at disc level L5–S1 affects S1 spinal nerve, not L5 spinal nerve. NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 170.
However, in the lumbar region (where disc herniations are common) the herniated disc affects the spinal nerve that exits the intervertebral foramen below the herniation (one level down), not the nerve that exits the intervertebral foramen at the level of the disc herniation. This is because IV discs in the lumbar region are located opposite the lower half of the intervertebral foramen, and not the center. Thus, spinal nerves in this region pass through the IV foramina above the disc. Summary example: A herniated disc between L-4 and L-5 affects L-5 spinal nerve and not L-4. See Figure 5.13.
Joints of vertebral arches
Vertebral arch joints occur between adjacent articular processes (superior below and inferior above). These are known as zygapophyseal joints in anatomy textbooks, but are called “facet” joints by clinicians. These are synovial joints with capsules and joint cavities.
Facet joints allow sliding movements between adjacent vertebrae that facilitate flexion, extension, and lateral bending of the vertebral column.
Clinical correlation
With age, the intervertebral discs become thinner and collapsed. This “settling” of the vertebral bodies increases weight bearing on facet joints. This can produce pain in and of itself, but can also lead to reactive diseases like the formation of osteophytes (bone spurs) and osteoarthritis.
Craniovertebral joints
These are the atlanto-occipital (between skull and C-1) and atlanto-axial (between C-1 and C-2) joints, described earlier with the cervical vertebrae. They are specialized for moving the head. It should be noted that there are no intervertebral discs between C-1 and the skull and between C-1 and C-2.
Ligaments of the vertebral column
Figure 5.14 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.31.Anterior longitudinal ligament: Runs the length of the vertebral column, from skull to sacrum, on the anterior surfaces of the bodies of the vertebrae. Is broad and strong and functions to resist anterior displacement of vertebrae and limit extension of the vertebral column.
Posterior longitudinal ligament: Runs the length of the vertebral column, from skull to sacrum, within the vertebral canal, on the posterior surfaces of the bodies of the vertebrae. It is thinner than the anterior longitudinal ligament and functions to prevent posterior displacement of vertebrae and “check” excessive flexion of the spine.
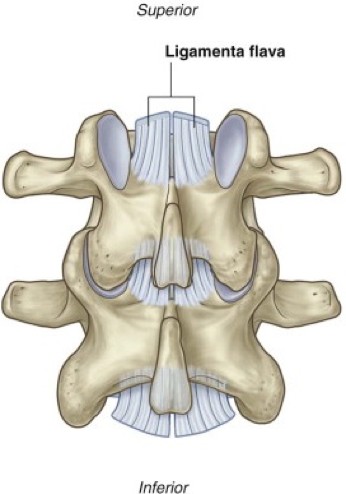
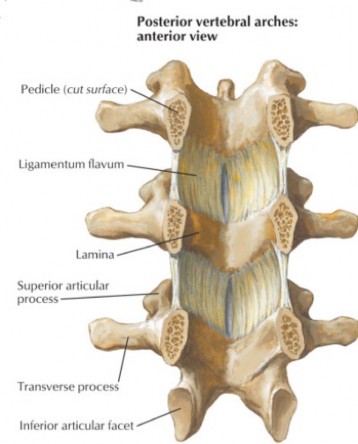
Ligamentum flavum (yellow ligament): Non-continuous, paired ligaments, in the posterior wall of the vertebral canal, connecting the laminae of adjacent vertebrae. They are composed mainly of elastic fibers, which give the ligaments their pale yellow appearance. These are strong ligaments that resist the separation of laminae during flexion of the spine. Their elastic recoil helps straighten the spine after it is flexed.
Note
Since the ligamenta flava occupy the gaps between adjacent vertebral laminae, they are penetrated during epidural injection or lumbar puncture procedures.
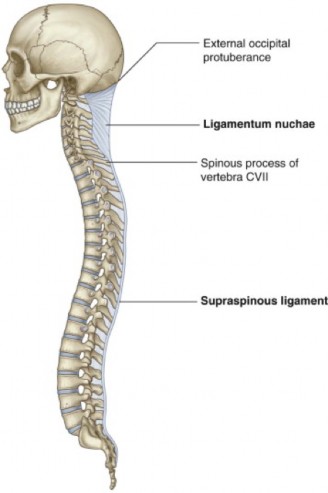
Supraspinous ligament: Extends from the sacrum to C-7 along the tips of vertebral spinous processes. In the cervical region, the supraspinous ligament is replaced by the nuchal ligament, a thick cord that runs between C-7 and the external occipital protuberance of the skull. Its deep fibers attach to the spinous processes of C-1 to C-6; because of the cervical lordosis, the nuchal ligament is deep and thick, forming a midline septum between the posterior muscles of the neck. The nuchal ligament supports the weight of the head against gravity when it is tipped forward. Grazing animals like cows have massive nuchal ligaments!
Figure 5.16 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 168.
Figure 5.17 GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIGURE 2.33.
Blood supply of the vertebral column
Arteries supplying the vertebral column and the contents of the vertebral canal are derived primarily from the segmental arteries of the trunk (posterior intercostal and lumbar arteries), which are branches of the descending aorta. Spinal arteries branch from these segmental arteries and enter the intervertebral foramina. After traversing the intervertebral foramina, the spinal arteries supply branches to the spinal cord, spinal nerves, vertebrae, ligaments, and meninges.
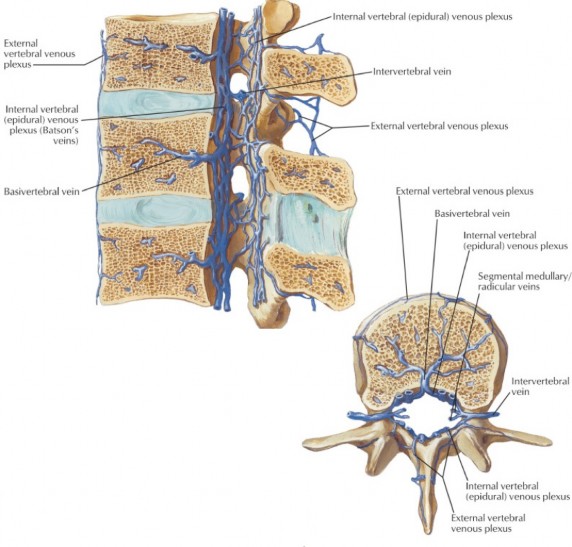
Vertebral venous plexuses drain the vertebral column, spinal cord, and meninges. The largest of these is the internal vertebral venous plexus, a network of interconnected veins within the vertebral canal, in the epidural space. The internal vertebral venous plexus forms a vertical channel of blood within the vertebral canal. At regular intervals, intervertebral veins pass through the intervertebral foramina, draining blood from the internal vertebral plexus into posterior intercostal or lumbar veins.
Figure 5.18 NETTER, ATLAS OF HUMAN ANATOMY, 7TH ED., PLATE 178.
Clinical correlation
The internal vertebral venous plexus has no valves. The amount of blood in the plexus fluctuates depending on pressures within the thoracic and abdominopelvic cavities. Increased pressures can push venous blood from segmental veins into the plexus in a reverse direction via intervertebral veins. Neoplasms of the prostate, lungs, and kidney have been known to metastasize into vertebrae through this venous route, because of the lack of valves in the system.