PhD · Clinical Assistant Professor, Department of Translational Medicine & Physiology
Office: PBS 41C
Table of Contents
Optional reading
Clinically Oriented Anatomy, 9th ed., Head chapter, Face and scalp section through Surface anatomy of face; Parotid and temporal regions, infratemporal fossa, and temporomandibular joint section through Infratemporal fossa.
The face is the anterior part of the head, located in front of the ears, above the margins of the mandible, and below the “hairline.” [Note: using this definition, it would seem that your anatomy professor has a rather tall face!] The term is derived from the Latin word facies (countenance), which refers to the features giving us our individual identify. Certain diseases alter the appearance of the face in distinctive ways (e.g., Parkinson’s disease).
Facial landmarks
Eyelids
The eyelids (Latin = palpebrae) are moveable folds of skin, connective tissue, and muscle that protect the eyeballs. The openings between them that we see through are palpebral fissures.
Lips
Lips (labia) surround the opening to the oral cavity (oral fissure). The upper and lower lips meet laterally at the labial commissures.
Philtrum
In the center of the upper lip is a depression called the philtrum (Greek: love charm).
External nose
Named parts of the external nose are: nares (nostrils), alae (sides, that can be “flared” when angry), apex (tip), root (between the eyes), and dorsum (bridge), connecting the apex and root.
Nasolabial sulcus
The bilateral groove passing downward from ala of nose to labial commissure is the nasolabial sulcus.
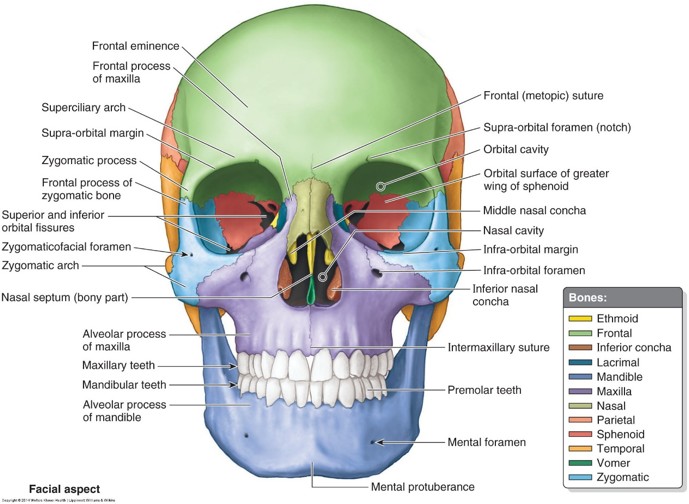
The neurocranium is the part of the skull surrounding and protecting the brain (“brain case”).
The other bones of the skull make up the facial skeleton (viscerocranium). The most important of these are the paired zygomatic bones (“cheek bones”), maxillae, nasal bones, and the mandible. The other bones of the facial skeleton support the nasal cavities. The appearance of the face is to a large extent determined by variations in shape and prominence of the underlying facial bones.
Clinical correlation
Facial fractures are the result of trauma to the face (MVA, falls, sports, fisticuffs).
Brokennose: Fracture of the nasal bones = the most common facial fracture.
Brokenjaw: Fracture of the mandible = second most common facial fracture
Broken cheekbone: Fracture of the zygomatic bone.
Midface fractures involve the maxillae, producing midface mobility.
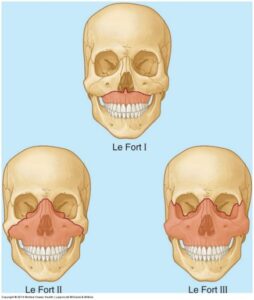
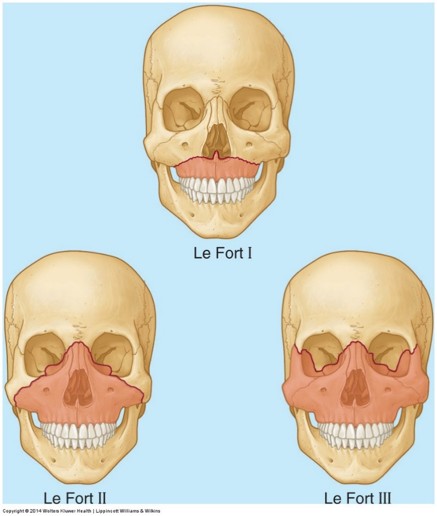
Dr. Le Fort, a French surgeon, developed a commonly used classification for these fractures (Le Fort fractures).
Figure 2. CLINICALLY ORIENTED ANATOMY, FIGURE B7.1.Le Fort Type I: Horizontal fracture through the alveolar process of the maxillae and nasal septum. The upper teeth become detached from the face with the bone fragment.
Le Fort Type II: Unilateral or bilateral fracture through the maxillae, infra-orbital foramina, lacrimal bones, and bridge of the nose. This produces a triangular fragment in the central face that is detached from the rest of the skull.
Le Fort Type III: Horizontal fracture through the greater wings of the sphenoid bones, superior orbital fissures, and ethmoid bone. If bilateral, this separates the facial skeleton from the cranial vault. Fracture of the ethmoid bone can cause leakage of cerebrospinal fluid (CSF) into the nasal cavity (CSF rhinorrhea).
Subcutaneous tissue
The face contains copious superficial fascia but little in the way of deep fascia. The superficial fascia of the face is unique since it contains skeletal muscles (mimetic muscles), whereas skeletal muscles in other parts of the body are invested by deep fascia. The subcutaneous tissue in the face consists of four blended components:
1. Superficial fat compartments
Separated by connective tissue septa (e.g., the nasolabial folds contain one of these fat compartments).
2. Loose connective tissue
Containing collagen fibers, elastic fibers, and fat cells that connect facial muscles to the overlying dermis of the skin.
3. Muscles of facial expression
(Mimetic muscles.)
4. Deep fat compartments below the mimetic muscles
Give shape and volume to the face and allow the muscles to glide and move freely. The largest of these is the aesthetically important buccal fat pad. Prominent in infants, it supports the cheeks during nursing and produces cute “chubby-cheeks”, a feature not so desirable in adults.
The construction of the subcutaneous tissue gives the skin remarkable mobility and aids in facial expression. The only discernable deep fascia in the face is an extension from the neck that covers the masseter muscle and parotid gland.
The pull of the underlying muscles produces temporary wrinkles and creases in the facial skin. Loss of collagen and elastic fibers in the face, a normal event with aging, causes these to become more noticeable and permanent, especially around the mouth, eyes (“crow’s feet”), and on the forehead (“worry lines”).
Aging also causes volume loss in the fat compartments, and this seems to occur at different rates in different areas of the face. The result is uneven facial contours and loss of the smooth transitions between facial regions that give the essence of youthfulness.
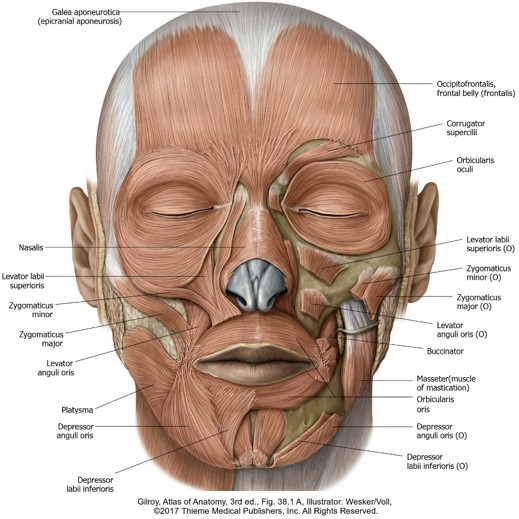
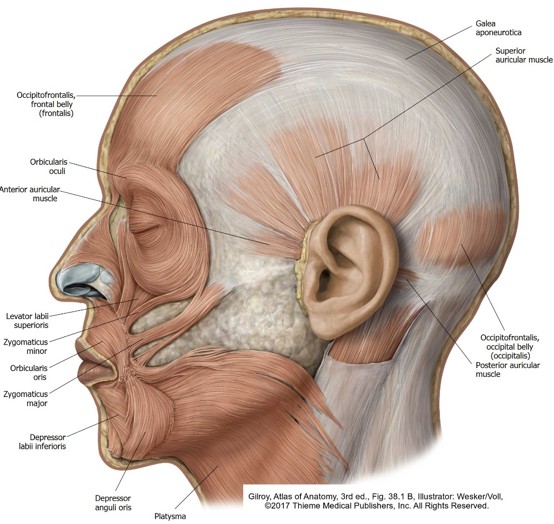
Muscles of facial expression (mimetic muscles)
Figure 3.
Figure 4.
All mimetic muscles are derived from the mesenchyme of the embryonic second pharyngeal arch. Therefore, all are innervated by branches of the facial nerve (VII). Second arch mesenchyme migrates into the scalp and neck as well, so muscles located there also impact facial expression.
The muscles of facial expression are thin and flat, originate from bone or fascia, and insert into the facial skin. They vary quite a bit in their size from person to person and many of them are blended together on the face. Some are quite small and not significant to medical students, so we will focus on the larger ones that can be seen in the lab. In general, mimetic muscles act as sphincters/dilators of facial orifices and elevators/depressors of the lips and eyebrows. We will group the major facial muscles as follows:
Peri-orbital facial muscles
Orbicularis oculi: Sphincter of the eyelids. The orbital part is arranged as concentric rings of muscle fibers outside the rims of the orbit. It forcefully closes the eyelids. The palpebral part is thin and located in the eyelids themselves. It gently closes the eyelids, as in blinking.
Peri-oral facial muscles
Zygomaticus muscles: Variably sized muscles (often 2) that attach to the zygomatic bone and corner of the mouth. Bilateral contraction pulls the corners of the mouth upward and backward, as in laughing and smiling. Unilateral contraction produces a sneer.
Levatorlabiisuperioris: Attaches to the maxilla and upper lip. Raises the upper lip and its medial fibers can also dilate the nostrils, as in snarling. Its actions deepen the nasolabial sulcus.
Depressor labii inferioris: Attaches to the mandible and lower lip. Depresses the lower lip as when pouting.
Levator anguli oris and depressor anguli oris: Arise from the maxilla and mandible, respectively, and insert into the corner of the mouth. These muscles curl the corner of the mouth up or down, when you are happy or sad.
Oribularis oris: Its circular fibers form the substance of the lips and interlace with all the other peri-oral facial muscles. It acts as a sphincter of the oral fissure to close the lips and can purse them as well.
Buccinator (Latin: trumpeter): Arises from the maxilla and mandible and a ligament called the pterygomandibular raphé. It merges with the muscles of the lips. Buccinator is located deep to the buccal fat pad in the cheeks, in a plane below the other mimetic muscles. The duct of the parotid gland penetrates the buccinator. It compresses the cheeks against the teeth, working with the tongue to keep food on the teeth during chewing. It also forces air from the mouth and through the lips. The buccinator is the “trumpeter’s muscle.”
Other facial muscles
Occipitofrontalis: Comprised of two muscle bellies (frontal and occipital) connected in the middle by a flat tendon (aponeurosis) in the scalp. The frontal belly (often called the frontalis muscle) attaches to the skin just above the orbits. It raises the eyebrows and wrinkles the skin of the forehead (the “muscle of surprise”). The occipital belly (occipitalis) attaches behind to the occipital bone. It produces backward movement of the scalp.
Platysma (Greek: “flat,” like the flat bill of the platypus): A broad, thin muscle originating from the fascia of the chest and shoulder and attaching above to the mandible and corner of the mouth, where it blends with the peri-oral muscles. When contracted, it can depress the mandible, but it is probably more important in drawing the corner of the mouth down and tensing the skin of the neck (“lizard neck”), as when expressing anger or horror. Aging causes its muscle fibers to thicken, producing vertical bands in the neck.
Fun fact
If you are talented enough to be able to wiggle your ears, you have well developed auricular muscles. These are important to animals who need to move their ears, but not so much for humans. We won’t see these in lab, but they are a novelty.
Masseter muscle
The masseter is not a muscle of facial expression, but a chewing (mastication) muscle. It is mentioned here because it is prominently located on the face and can be easily seen and felt when the teeth are clenched. It largely covers the ramus of the mandible. On its surface it is crossed by the zygomaticus muscles, parotid duct, and branches of the facial nerve. We’ll learn more about it when we study the muscles of mastication.
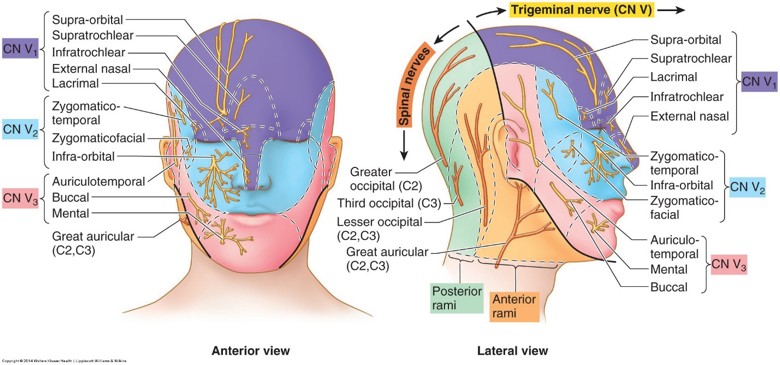
Branches of all three divisions of the trigeminal nerve supply the face. Study atlas figures to identify the specific nerves. Some of the larger ones will be seen in lab. It is important to understand the dermatome map of the face, since it is part of clinical testing of the trigeminal nerve.
Ophthalmic division (V1)
Supplies the forehead, upper eyelid, and dorsum of the nose through the supra-orbital, supratrochlear, infratrochlear, lacrimal, and external nasal nerves.
Maxillary division (V2)
Supplies the lower eyelid, midface, temporal region, and sides of the nose through the infra-orbital, zygomaticofacial, and zygomaticotemporal nerves.
Mandibular division (V3)
Supplies the chin, lower lip, cheek, external ear, and scalp via the mental, buccal, and auriculotemporal nerves.
The great auricular nerve, a branch of the cervical plexus (spinal nerves C-2 and C-3), supplies a small region of the facial skin over the angle of the mandible.
Clinical correlation
Herpes zoster (shingles) can affect the trigeminal nerve, producing vesicular lesions on the face.
V1 is the most commonly affected division (herpes zoster ophthalmicus, or HZO). V1 not only supplies sensory nerves to the forehead, bridge of the nost, and upper eyelid, it supplies the cornea of the eyeball, too. Ulcerations on the cornea can lead to scarring and vision loss. Shingles of the face affecting one division of CN V is particularly striking, as the lesions produce a map of the dermatome, usually unilaterally.
Lesions on the tip of the nose (skin supplied by the external nasal branch of V1) usually precede the full outbreak of the ophthalamic shingles—this warning signal is called Hutchinson’s sign.
Trigeminal neuralgia (also known as Tic douloureux, due to the facial twitches that accompany the disorder) is a neurologic condition affecting the trigeminal nerve that presents as extreme, sporadic, and sometimes incapacitating attacks of facial pain.
It is usually unilateral and typically occurs in the areas of the face served by the maxillary (V2) or mandibular (V3) branches of CN V. It can be triggered by simple things—brushing teeth, shaving, talking, or chewing—or it may occur spontaneously.
Current research suggests that, in many cases, the cause is compression of the main trunk of the trigeminal nerve near the pons by a blood vessel.
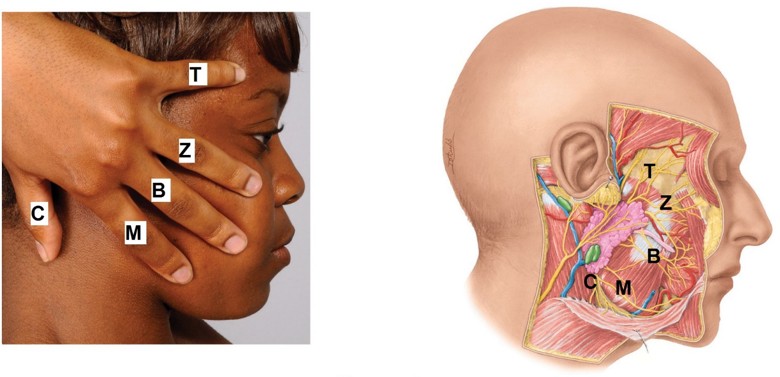
Motor innervation of mimetic muscles
Figure 6. Branches of the facial nerve on the face.
T: Temporal
Z: Zygomatic
B: Buccal
M: Marginal mandibular
C: Cervical.
CLINICALLY ORIENTED ANATOMY, FIGURE 7.23.
After emerging from the stylomastoid foramen, the facial nerve enters the parotid gland. Here it gives rise to five named branches that pass on to the face and neck: temporal, zygomatic, buccal, marginal mandibular, and cervical. These supply the mimetic muscles and are named for the regions of the face to which they are distributed. The cervical branch passes below the mandible into the neck to supply the platysma muscle.
Mnemonic
A time-honored mnemonic for remembering the branches of the facial nerve on the face is: “To Zanzibar By Motor Car.”
Clinical correlation
Bell's palsy is a form of facial paralysis due to facial nerve damage. Most cases are thought to be caused by a viral infection, such as the herpes simplex virus, that produces swelling and compression of the nerve in the facial canal.
Most cases are unilateral and temporary. Weakness or paralysis of mimetic muscles produces inability to close the eyelids, dropping of the corner of the mouth, and drooling. Other symptoms could include dry eye and mouth and taste impairment (why?). Diagnosis is made by clinical presentation and ruling out other possible causes of facial paralysis.
Vascular supply and lymphatic drainage of the face
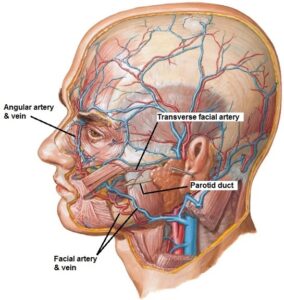
Arteries
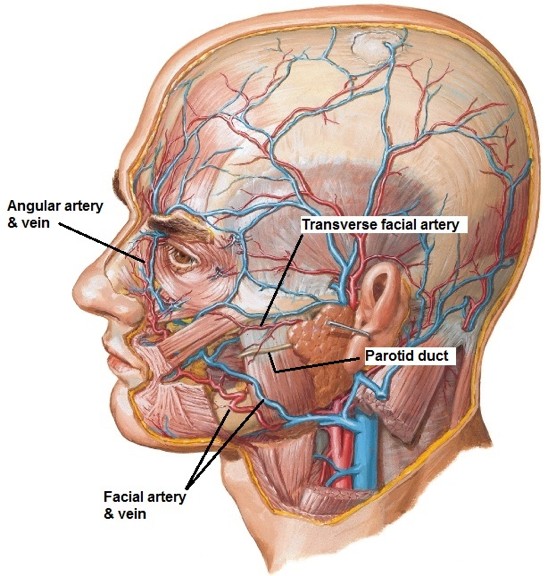
Figure 7. NETTER, ATLAS OF HUMAN ANATOMY, PLATE 3.
The face has a rich blood supply, primarily from the facial artery, a branch of the external carotid artery. Arising in the neck, the facial artery ascends and curves around the submandibular gland to cross the mandible, where its pulsations are palpable and it can be compressed to alleviate bleeding. On the face, it has an oblique course through the buccal fat pad deep to the muscles of facial expression. When it parallels the nose, the facial artery is called the angular artery. It terminates at the medial angle of the eye. Two important branches of the facial artery are the inferior and superior labial arteries to the lips.
The transverse facial artery, a branch of the superficial temporal artery, is the other significant source of blood. It courses across the face parallel to the zygomatic arch.
Veins
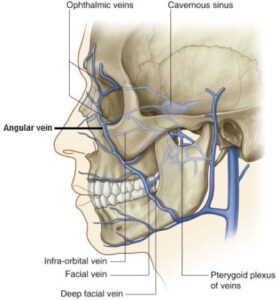
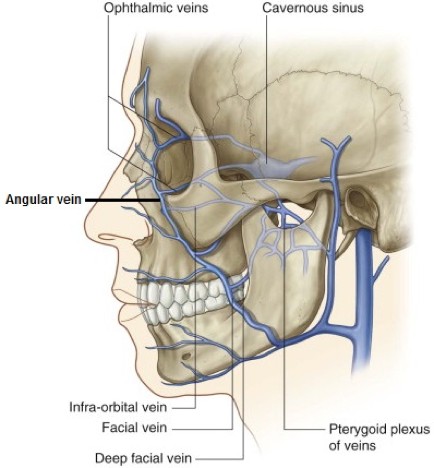
Figure 8. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.65.
The angular vein is formed at the medial angle of the eye by the union of the supra-orbital and supratrochlear veins; below the nose it becomes the facial vein, a tributary of the internal jugular vein. The course of the facial vein parallels the facial artery.
Clinical correlation
The veins of the face have clinically important venous connections to the cavernous sinuses.
Since these vessels have no valves, blood can course in either direction depending on pressure differences. This sets up a potential route for spread of infection from face to the cranial activity. The largest of these routes is through the ophthalmic veins in the orbit. These connect of the face to the angular veins and in cranial activity to the cavernous sinuses.
Lymphatic drainage
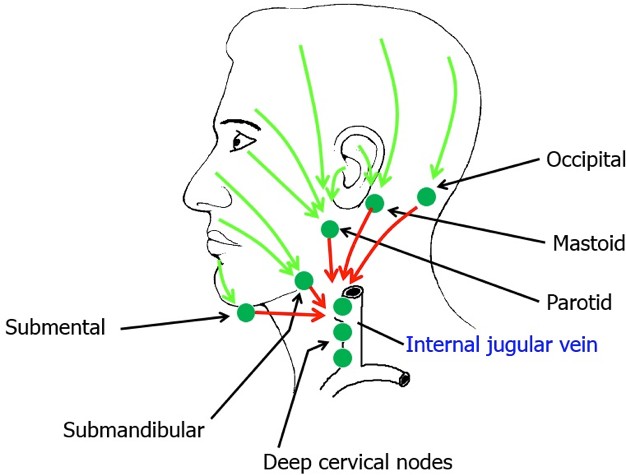
Figure 9. Schematic of lymph drainage from face and scalp. HAND-DRAWN CONLEY-GRAM.
Lymphatic vessels of the face and scalp parallel blood vessels, with lymph flowing downward toward a collar of lymph nodes at the base of the head. Nodes and their regions of drainage are:
Submental nodes: Central lower lip and chin.
Submandibular nodes: Nose, buccal region of cheek, upper lip, and lateral lower lip.
Parotid nodes: Eyelids, cheekbones, anterior and central scalp, external acoustic meatus, and anterior part of the auricle.
Mastoid nodes: Central and posterior scalp, posterior part of the auricle.
Occipital nodes: Posterior scalp and neck.
After percolating through these nodes, lymph from the face and scalp passes to the deep cervical lymph nodes along the internal jugular veins in the neck.
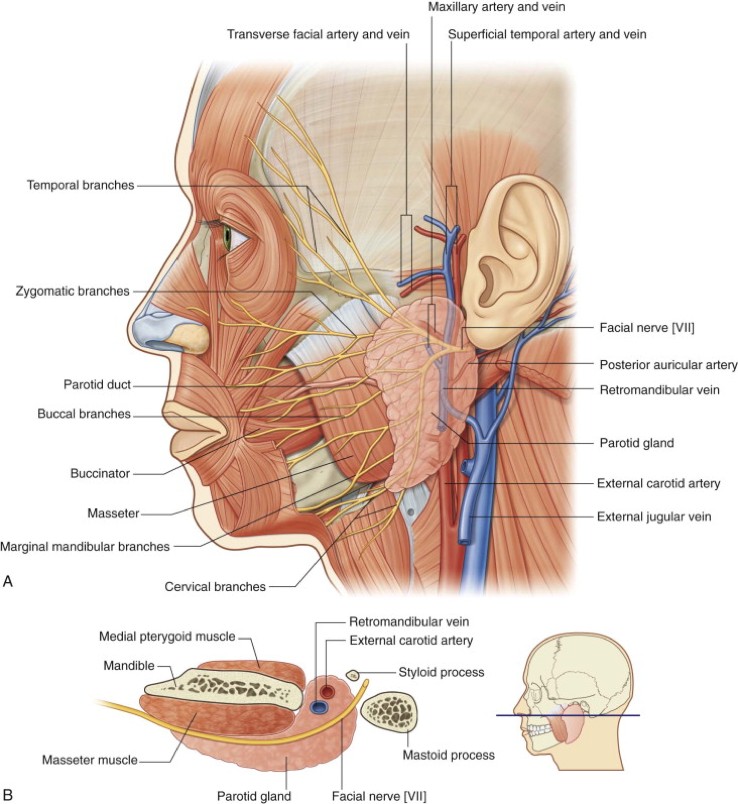
Parotid gland
Figure 10. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.59.
The parotid (Greek: “beside the ear”) is the largest of the major salivary glands. It lies in the depression between the ramus of the mandible and the sternocleidomastoid muscle, surrounded by a capsule of deep fascia. The parotid is a double pyramid:
When viewed on the face, it is wider above and tapers down to an apex near the sternocleidomastoid.
In horizontal section, it has a wide superficial part external to the mandible and masseter muscle, and a narrow deep part wedged between the ramus of the mandible, mastoid process, and styloid process.
Because it is compressed when the mouth is opened wide, pain may be elicited when the gland is swollen due to mumps or a blocked duct.
Several structures course through the gland. These are best learned in layers, from superficial to deep:
1. The facial nerve enters the parotid and divides into five branches (temporal, zygomatic, buccal, marginal mandibular, and cervical). These emerge from the gland on to the face to supply the mimetic muscles. Removal of the parotid thus requires meticulous surgical dissection.
2. The retromandibular vein is formed within the gland by the union of the superficial temporal and maxillary veins. Within (or below) the gland it divides into anterior and posterior divisions. The posterior division joins the posterior auricular vein to form the external jugular vein. The anterior division usually joins the facial vein.
3. The external carotid artery divides within the gland into its terminal branches, the maxillary and superficial temporal arteries.
4. The auriculotemporal nerve, a branch of V3 passes deep to the gland on its way to the scalp. Postganglionic parasympathetic fibers from the glossopharyngeal nerve innervate the parotid by hitching a ride with the auriculotemporal.
The parotid duct (Stensen’s duct) is located parallel to the tip of the ear lobe. It crosses the masseter muscle, pierces the buccal fat pad and the buccinator, and empties into the oral cavity adjacent to the second upper molar. Accessory glandular tissue may lie along its course.
Clinical correlation
Stumps of postganglionic parasympathetic fibers may remain after surgical removal of the parotid (parotidectomy), and they could regenerate and grow into the overlying skin.
Food in the mouth (or even the thought of food) can trigger these nerves to release acetylcholine into the skin instead of the gland, stimulating sweat glands and blood vessels. This facial sweating and flushing instead of salivation is called Frey’s syndrome (gustatory sweating syndrome).
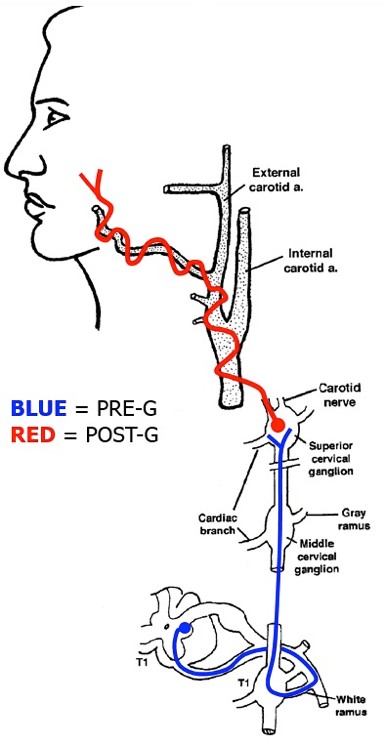
Appendix: Sympathetic innervation of the face
Figure 11. Pathway of sympathetic innervation to the face. HAND-DRAWN CONLEY-GRAM.
Sympathetic fibers supplying visceral structures in the face follow the same basic pathway as all sympathetic nerves to the head. This pathway is summarized and reviewed here.
Preganglionic sympathetic fibers destined for the head originate from the intermediolateral cell column (in the lateral horns of gray) of the upper thoracic spinal cord segments (T-1 and T-2). They enter the sympathetic trunk through white rami communicantes.
Preganglionic fibers ascend through the sympathetic trunk to the superior cervical ganglion, situated opposite C-2 vertebra. Here they synapse on postganglionic sympathetic neurons.
Postganglionic fibers leave the superior cervical ganglion as several carotid nerves. These pass onto the internal and external carotid arteries, forming carotid plexuses. Postganglionic sympathetic fibers follow branches of the external carotid artery (e.g., facial artery, superficial temporal artery) onto the face and scalp, and then hitch rides on branches of CN V to reach and innervate sweat glands, arrector pili muscles, and smooth muscle in blood vessels.