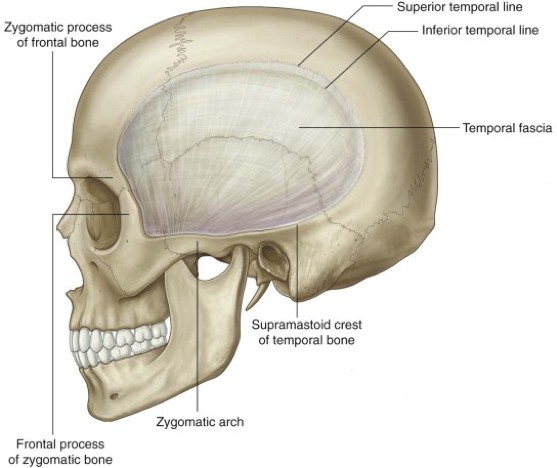
Figure 1. Attachments of temporal fascia. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.138.
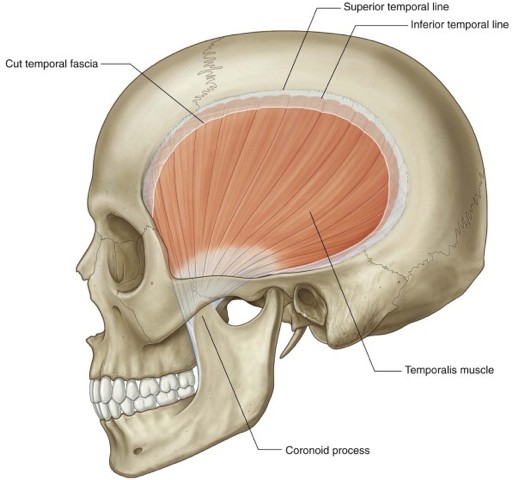
Figure 2. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.139.
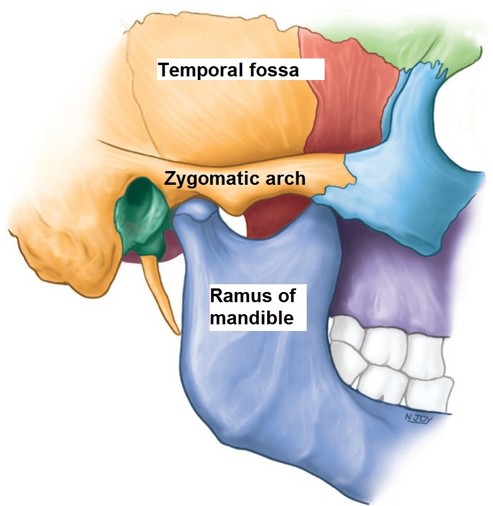
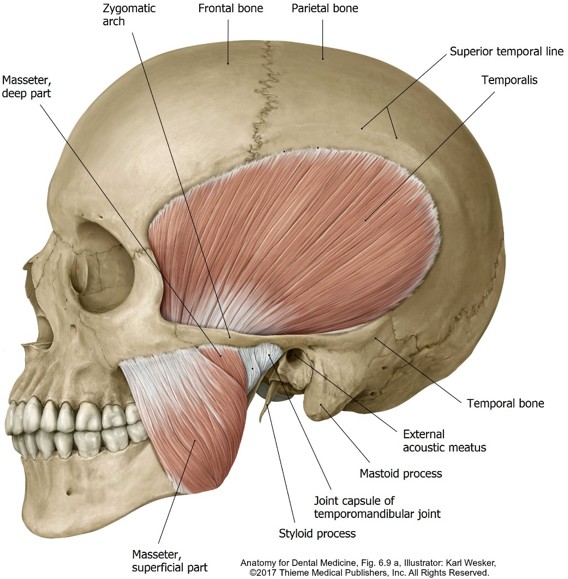
The temporal fossa is the sunken area located on the lateral skull above the zygomatic arch.
Boundaries
Its floor contains portions of the frontal, parietal, temporal, and sphenoid bones.
The upper boundary is the curved superior temporal line. The inferior boundary is the zygomatic arch.
contents
The temporal fossa is occupied by the temporalis muscle and its fascia, nerves, and vessels.
Origin
Temporalis arises from the bony floor of the fossa and from the deep surface of the stout temporal fascia, which covers the muscle externally. The temporal fascia attaches above to the superior temporal line and below to the zygomatic arch. The scalp is external to the fascia.
Insertion
The muscle fibers are arranged like a fan. They converge below on a tendon that attaches to the coronoid process of the mandible.
Actions
Temporalis is a chewing muscle. Its vertical fibers elevate the mandible to close the jaw. The horizontal fibers retract the mandible after it has been protruded.
innervation
The deep temporal nerves (from V3) and deep temporal arteries (from the maxillary artery) enter the deep surface of the muscle, passing upward between the muscle and the bony floor of the temporal fossa.
Infratemporal region
The infratemporal fossa (ITF), as its name implies, is located inferior to the temporal bone and temporal fossa. It is wedge-shaped: wider at the top and tapered at the bottom. The infratemporal fossa is not easily visualized externally since it is located deep to the masseter muscle and ramus of the mandible.
Bony anatomy
Imagine the infratemporal fossa as a bony box, tipped upside-down, with its lid open. We will begin our discussion with an empty box, and then add its contents.
Boundaries
The boundaries of the ITF are:
Lateral: Ramus of mandible.
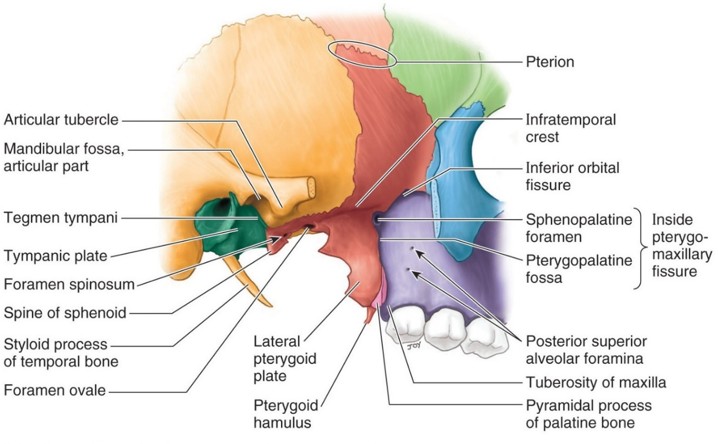
Medial: Lateral surface of the lateral pterygoid plate (sphenoid bone). The pharynx is also in the medial wall.
Anterior: Posterior surface of the body of the maxilla.
Posterior: Tympanic plate (the shelf of bone below the external acoustic meatus) and styloid process—both are parts of the temporal bone.
Superior: Infratemporal surface of the greater wing of the sphenoid bone. The gap deep to the zygomatic arch connects the infratemporal fossa to the temporal fossa above. It is filled with the temporalis muscle.
Inferior: Has no bony boundary—it is closed by the attachment of the medial pterygoid muscle to the mandible.
The bony box has openings through which the ITF communicates with other regions of the head. It’s fun to spend some time with your skull and locate these openings with a pipe cleaner. You should know the structures that pass through each of these openings:
There are four chewing (mastication) muscles: one in the temporal fossa (temporalis), one on the face (masseter) and two in the infratemporal fossa (medial and lateral pterygoid).
All are derived from the mesenchyme of the embryonic first pharyngeal arch.
All are innervated by the only branch of the trigeminal nerve that carries motor fibers = the mandibular nerve (V3).
All receive their blood supply from the maxillary artery.
Located on the face and largely covered by the parotid gland.
Origin: Its two heads arise from the zygomatic bone and zygomatic arch.
Insertion: External surface of ramus of mandible.
Action: Elevates the mandible to close the jaw and clench the teeth.
Innervation: Masseteric nerve from V3.
Medial pterygoid muscle
Figure 6. NETTER, ATLAS OF HUMAN ANATOMY, PLATE 49.
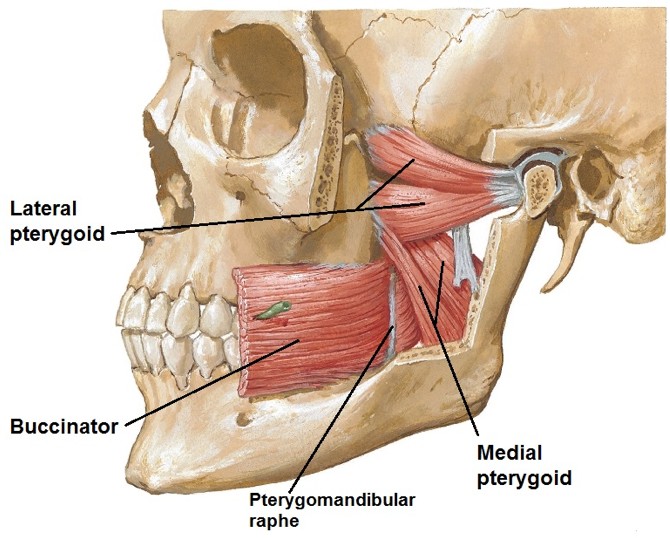
Quadrangular muscle within the ITF that slopes medial to lateral as well as anterior to posterior. It is essentially the mirror image of the masseter muscle, but on the internal surface of the mandibular ramus (the masseter is on the external surface).
Origin: Arises as two heads, one from the maxilla and one from the medial surface of the lateral pterygoid plate (sphenoid bone).
Insertion: Medial surface of ramus of mandible.
Action: Elevates the mandible and helps protrude it.
Innervation: Branch of V3.
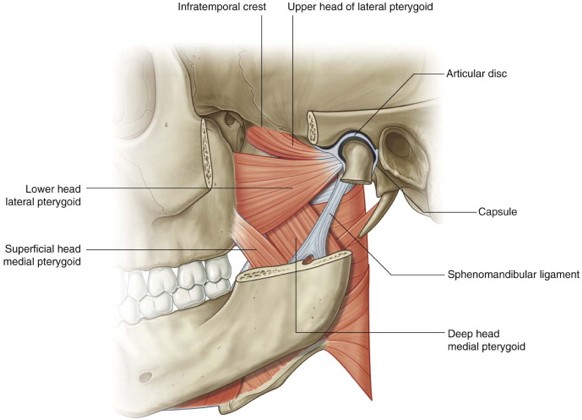
Lateral pterygoid muscle
Triangular muscle in the ITF = broad at its origin, tapers at its insertion.
Origin: Like the medial pterygoid, it has two heads. The upper head arises from the greater wing of the sphenoidbone (roof of ITF), while the lower head arises from the lateral surface of the lateral pterygoid plate.
Insertion: The two heads converge and attach to the neck of the mandible (just below the condyle) and to the capsule of the temporomandibular joint.
Action: Protrudes the mandible, an action necessary for any substantial opening of the mouth.
Innervation: Branch of V3.
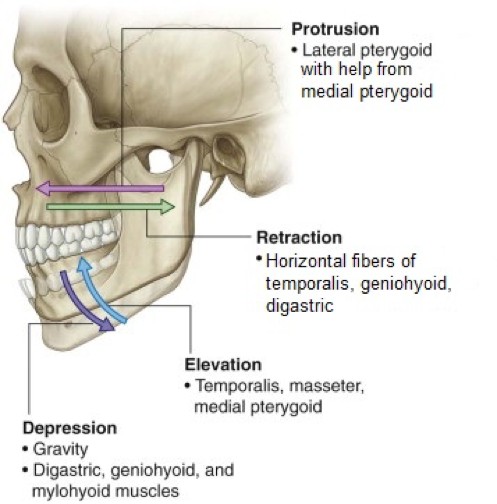
Summary: Movements of the mandible
These occur at the temporomandibular joint (TMJ).
Three muscles (temporalis, masseter, and medial pterygoid) can elevate the jaw and clench the teeth. This explains the power generated for biting.
Because of the direction in which chewing muscles attach to the mandible, the jaw can be deviated medial and lateral while being elevated and depressed. Synchronized action of the muscles can thus produce the motions needed for grinding food on the teeth.
The buccinator muscles (muscles of facial expression) assist with chewing by compressing the cheeks to keep food on the teeth.
Gravity helps with opening the mouth (depressing the mandible) when the head is upright. Suprahyoid muscles (geniohyoid, mylohyoid, digastric), located below the chin, are recruited to assist with depressing and retracting the mandible when there is resistance to such movements—i.e., when gravity can’t help.
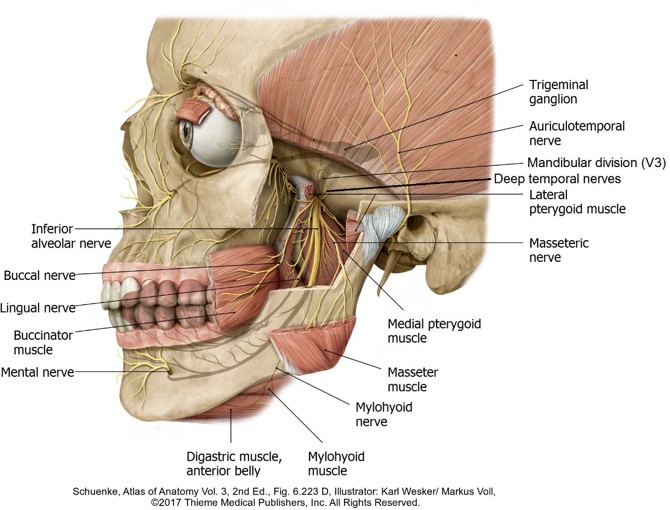
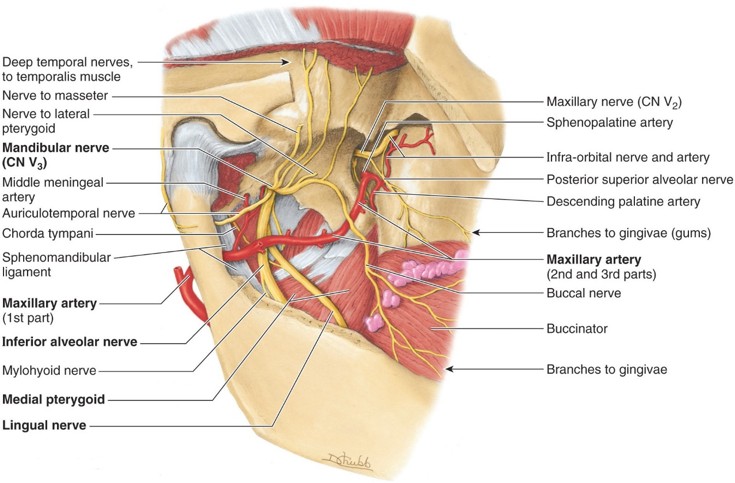
As it leaves the trigeminal ganglion in the middle cranial fossa, V3consists of a large sensory root and a smaller motor root. The roots pass separately through foramen ovale and fuse just below it. The main trunk of the nerve is deep to the lateral pterygoid muscle. Anatomy texts describe V3 as separating into anterior and posterior divisions within the ITF. This can’t be seen very well in the lab, so we will simply classify the major branches of V3 as sensory or motor. The branches leave V3 high in the ITF, just below foramen ovale. Their origins can only be seen by removing the lateral pterygoid muscle.
Sensory branches of V3
Figure 8.
Figure 9. Branches of V3 shown after removal of lateral pterygoid muscle. CLINICALLY ORIENTED ANATOMY, FIGURE 7.74.
Buccal nerve: Passes downward and forward, adjacent to and sometimes within the tendon of temporalis. It supplies the check—both the skin outside and mucous membrane inside.
Note
Don’t confuse this nerve with the motor buccal branch of the facial nerve!
Lingual nerve: Heads toward the oral cavity sandwiched between the medial pterygoid muscle and ramus of the mandible. Transmits general sensation from the anterior 2/3 of the tongue, floor of the mouth (sublingual area), and the lingual sides of the lower gums (gingivae). The chorda tympani nerve joins the lingual in the ITF. Thus the lingual nerve also carries preganglionic parasympathetic fibers (to the submandibular and sublingual glands) and taste fibers from the anterior 2/3 of tongue.
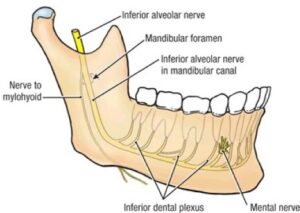
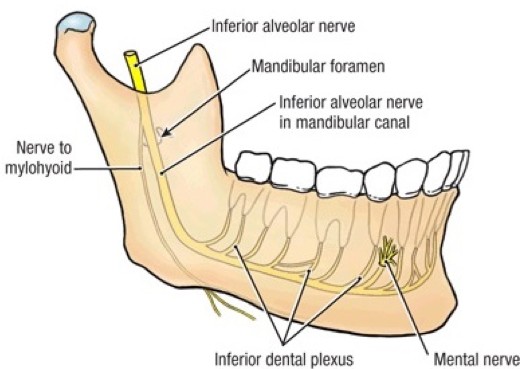
Figure 10. GRANT’S ATLAS OF ANATOMY, 13TH ED., FIGURE 7.52.Inferior alveolar nerve: Enters the mandibular foramen and traverses the body of the mandible via the mandibular canal. Transmits general sensation from the lower teeth. The mental nerve, a branch of the inferior alveolar, supplies the skin of the lower lip and chin via the mental foramen.
Auriculotemporal nerve: Leaves V3as two trunks that encircle the middle meningeal artery and fuse lateral to it. Passes deep to the condylar process of the mandible and the parotid gland, ascends on the face anterior to the auricle, and then enters the scalp. Transmits general sensations from the scalp, auricle, and temporomandibular joint. It carries postganglionic parasympathetic fibers from the otic ganglion that innervate the parotid gland.
Clinical correlation
An inferior alveolar nerve block is done by injecting an anesthetic agent into the area near the mandibular foramen, via the oral cavity. It not only anesthetizes the lower teeth and gums, it numbs the lower lip and chin (dermatome of the mental nerve), producing the strange sensation of having a "fat lip."
Motor branches of V3
Nerve to tensor veli palatini muscle (a muscle of the soft palate).
Nerve to tensor tympani muscle (in the tympanic cavity).
Nerves to medial and lateral pterygoid muscles.
Masseteric nerve.
Deep temporal nerves (anterior and posterior—to the temporalis muscle).
Nerve to mylohyoid and anterior belly of digastric: Hitches a ride with the inferior alveolar nerve, branching from it just before it enters the mandibular foramen.
Chorda tympani nerve
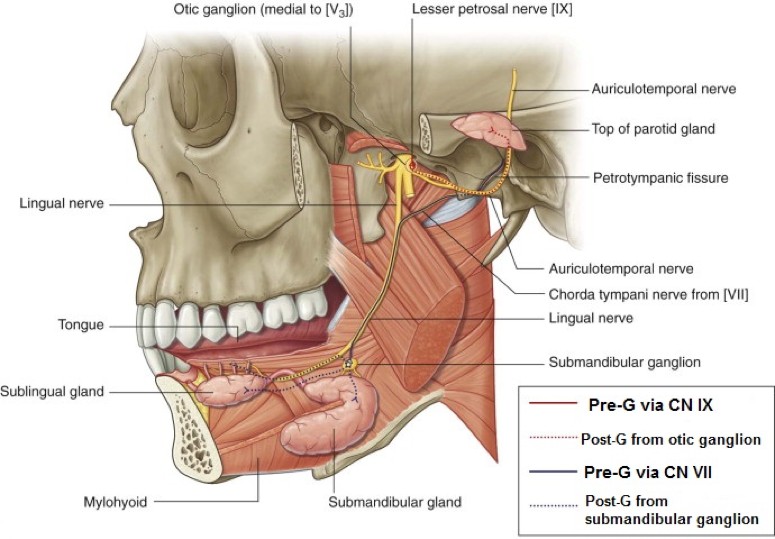
From cranial nerve VII, it carries taste fibers from the anterior 2/3 of the tongue and visceral motor (parasympathetic) fibers to the submandibular ganglion. Chorda tympani enters the ITF from the tympanic cavity through the petrotympanic fissure—a tiny crack in the temporal bone just anterior to the temporomandibular joint. It joint the lingual nerve high in the infratemporal fossa.
Otic ganglion
One of the four parasympathetic ganglia of the head, it is located in the ITF attached to the medial side of the mandibular nerve just inferior to foramen ovale. Preganglionic parasympathetic fibers from the lesser petrosal nerve (CN IX) synapse on postganglionic cell bodies in the otic ganglion. Lesser petrosal enters the ITF through foramen ovale.
Postganglionic fibers travel with the auriculotemporal nerve to their destination: the parotid gland.
Parasympathetic fibers
Figure 11. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.146.
The pathways of innervation of the three major salivary glands traverse the infratemporal fossa. They originate in cranial nerves VII (submandibular and sublingual glands) and IX (parotid gland), but finish their journeys as postganglionic parasympathetic fibers hitching rides on branches of the V3 in the ITF (lingual and auriculotemporal nerves). Synapses between pre-G and post-G neurons occur at the submandibular and otic ganglia. The pathways of innervation are sketched out in flow charts in The oral region and pharynx.
Posterior superior alveolar nerves
Branches of the maxillary nerve (V2), they pass out of the pterygopalatine fossa via the pterygomaxillary fissure. In the ITF, they pass along the posterior surface of the maxilla and enter it via tiny foramina. These nerves carry sensation from the upper molar teeth and their gingivae and from the mucosa of the maxillary air sinus.
Blood vessels of the infratemporal fossa
Maxillary artery
Figure 12. Branches of the maxillary artery. Anatomists and clinicians divide the artery into three parts. The first two (mandibular and pterygoid parts) give off branches in the infratemporal fossa. GRANT’S ATLAS OF ANATOMY, 13TH ED.,FIGURE 7.51.
One of two terminal branches of the external carotid artery (what is the other one?), it enters the ITF from the parotid gland by passing deep to the condylar process of the mandible. It is intimately associated with the lateral pterygoid muscle. In about 50% of cases it passes superficial to the muscle, while in the other 50% it passes deep to the lower head of the muscle.
This artery can be a toughie for several reasons: it is difficult to dissect(tough fascia and often hidden by the lateral pterygoid muscle), has many branches (some quite small), and it disappears from view rather quickly as it enters the pterygopalatine fossa via the pterygomaxillary fissure. A favorite textbook of your professor labels this artery as “the bane of the medical student”! Realistically, medical students have many banes, so we will simplify the maxillary artery by placing its branches into a few categories.
Keep in mind
This scheme does not organize arteries in the topographic order in which they branch. Consult your Atlas.
Deep auricular and anterior tympanic arteries supply the external acoustic meatus and tympanic cavity, respectively. Very small. We won’t see these in lab.
Middle meningeal artery: Super-important branch that enters thecranial cavity via foramen spinosum. It supplies blood to the periosteum, bones, and dura associated with the calvaria (skull cap).
Accessory meningeal artery: Not too important and often absent. Enters the cranial cavity via foramen ovale to supply dura in the floor of the middle cranial fossa.
Inferior alveolar artery: Follows the nerve of the same name into the mandibular foramen and mandibular canal where it supplies the lower teeth.
Posterior superior alveolar artery: Its small branches follow the nerves of the same name into the maxilla, supplying the posterior molar and premolar teeth and maxillary air sinus.
Infra-orbital artery: Enters the orbit via the inferior orbital fissure. It supplies a few extra-ocular muscles in the orbit and a small portion of the central face, but perhaps its most important job is to supply the upper incisor and canine teeth.
Descending palatine and sphenopalatine arteries: These arise from the maxillary artery within the pterygopalatine fossa, so we won’t describe them here. These arteries can be considered the terminal branches of the maxillary artery.
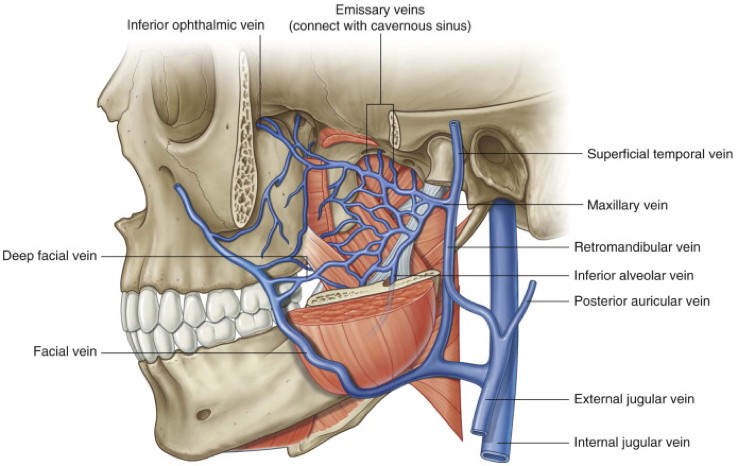
Pterygoid venous plexus
Figure 13. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.148.
This network of small veins courses through the fascia in the ITF and surrounds the lateral pterygoid muscle. A short maxillary vein drains the plexus, joining the superficial temporal vein within the parotid gland to form the retromandibular vein. Tributaries of the pterygoid plexus drain structures that are supplied by the maxillary artery. It hasclinical importance as a “go-between,” connecting veins of the face with the cavernous sinus. This route, along with a route through the orbit (ophthalmic veins—described with the face on the Face and Parotid Gland page), provides a possible way for infections to pass from face to cranial cavity.
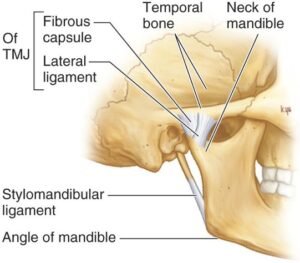
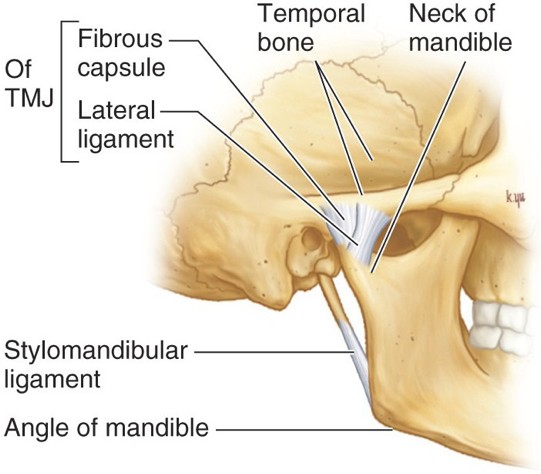
Sphenomandibular ligaments
Figure 14. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.143.
Located on each side of the head within the infratemporal fossae, they attach above to the inferior surface of the sphenoid bone near the foramen spinosum and below to the lingula of the mandible, a bony spine near the mandibular foramen. Just above this, the inferior alveolar nerve is sandwiched between the ligament and mandible. These are thought to function as supports for the lower jaw and as check ligaments to prevent excessive movements of the TMJ.
Temporomandibular joint (TMJ)
The TMJ is the largest and most clinically important synovial joint in the head. Before we consider the TMJ, let’s lay out the features all synovial joints possess, since we haven’t learned about them yet.
General features of synovial joints
Figure 15. CLINICALLY ORIENTED ANATOMY, FIGURE 7.69.Articular (joint) capsule: A tough layer of dense connective tissue that joins together the articulating bones, allowing them to move relative to one another without being pulled apart.
Articular (joint) cavity: Within the joint capsule, it contains lubricating fluid and provides the space for the bones to move.
Articular cartilage: The articular surfaces of bones within synovial joints are line by hyaline cartilage. It resists and distributes compressive forces.
Synovial membrane: Loose connective tissue lining the inside of the articular capsule and richly supplied with blood vessels. It produces synovial fluid.
Synovial fluid: “Joint oil” —a viscous fluid resembling egg white (ovia = Latin for “egg”) that lubricates the joint surfaces and provides nutrients. It is “nature’s WD-40.”
Ligaments: Located around the joint capsule, they further reinforce the joint.
A small number of synovial joints (knee and TMJ, for example) contain one or more articular discs (menisci). These are shelves of fibrocartilage within the joint cavity. They are thought to add cushioning and allow for complex joint movements, such as combinations of rotation and forward/backward gliding.
The temporomandibular joint is the articulation between the condyle of the mandible and the mandibular fossa of the temporal bone. The condyle is elliptical in shape, having its long axis oriented from medial to lateral.
Anterior to the mandibular fossa is a rounded eminence on the inferior margin of the zygomatic arch called the articular tubercle. It restricts excessive anterior movement of the mandible and possible dislocation of the joint.
The articular capsule of the TMJ is attached around the edge of the mandibular fossa, to the articular tubercle, and to the neck of the mandible just below the condyle.
The TMJ is different from most synovial joints in that the articular cartilage is fibrocartilage, not hyaline cartilage.
The TMJ has an articular disc (called the meniscus by clinicians) situated in the center of the joint space. It attaches to the entire circumference of the joint capsule, dividing the joint space into two joint cavities: upper and lower joint spaces.
The lateral pterygoid muscle inserts into the TMJ capsule and to the neck of the condylar process. When the muscle contracts, both the mandible and TMJ capsule move forward. Since the articular disc attaches to the joint capsule, it too moves forward when the mouth opens.
The auriculotemporal nerve and the superficial temporal artery supply the TMJ.
Clinical correlation: TMJ dysfunction
Trivia night in the anatomy lab!
Every time you swallow, your molar teeth come in contact (try it and see). During this contact about 25 pounds of pressure is placed on the teeth. Much of this pressure is transferred to the TMJ. It’s no wonder that TMJ dysfunction is common.
Technically known as internal derangementof the TMJ.
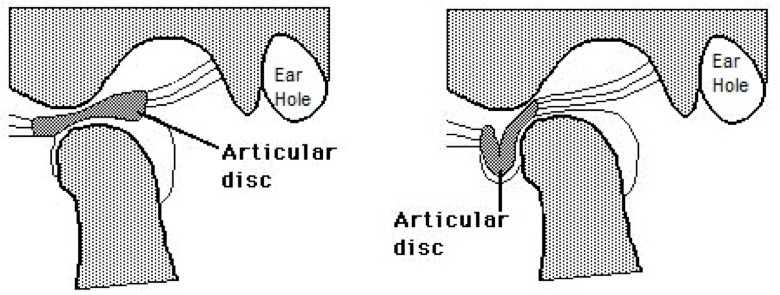
Joint clicking occurs when the articular disc becomes displaced anterior to the mandibular condyle when the mouth is opened (anterior displacement of the disc). If the displaced articular disc returns to its normal place as the mouth is opened wider, the patient will feel a “pop” and hear a “click.” This is called anterior displacement with reduction. If the articular disc remains displaced throughout the entire range of joint motion, the displacement is without reduction. These patients cannot fully open their mouths.
Displacement of the articular disc demonstrated in donor specimens: Watch this “yoint video” from Sweden.
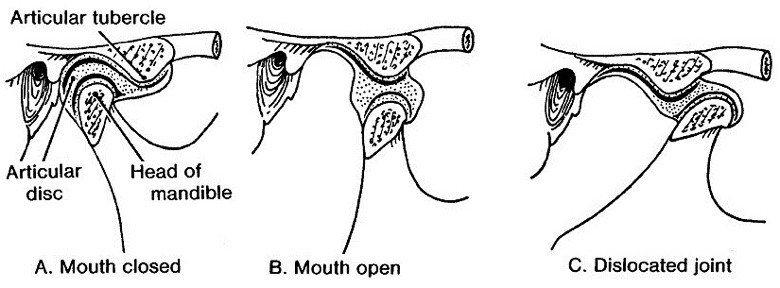
Clinical correlation: TMJ dislocation
When the mouth is widely opened (as in yawning during an anatomy lecture), the mandibular condyle and articular disc are precariously perched on the articular tubercle. A sudden contraction of the muscles that open the mouth, or a slap on the back from your classmate, could pull the articular disc and mandibular condyle over the edge of the prominence into the infratemporal fossa. Once there, the masseter and medial pterygoid muscles may spasm and clamp down on the dislocated mandible like a vise. The patient comes into the Emergency Department with his or her mouth stuck open. The dislocation is reduced by pulling the mandible downward with the thumbs (heavily wrapped in gauze) to clear the articular tubercle, then giving it a backward push to click it into place.
Figure 18. FROM LUYKNH, LARSEN PE: THE DIAGNOSIS AND TREATMENT OF THE DISLOCATED MANDIBLE. AMJ EMERG MED 1989; 7:329.