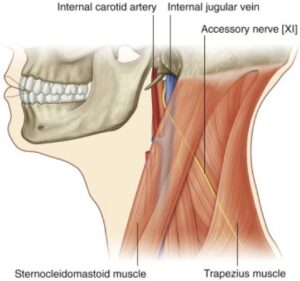
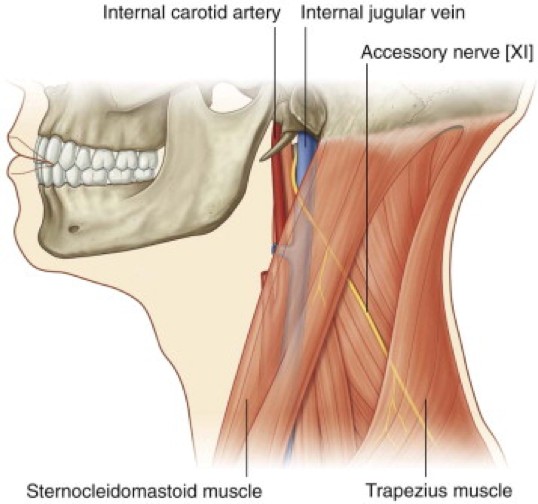
Figure 1. Gray’s Anatomy for Students, 3rd ed., Figure 8.157.
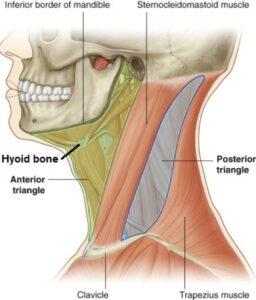
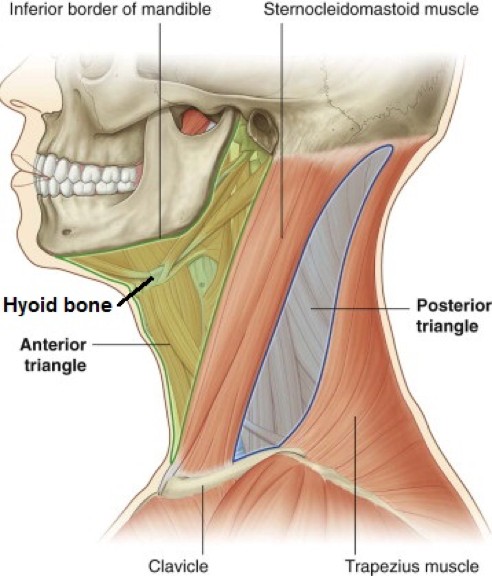
The anterior neck (“neck proper” or cervix): Extends from the inferior border of the mandible superiorly to the clavicles and sternum inferiorly.
The posterior neck (nucha or “nape”): Extends from occipital bone and mastoid processes above to C-7 vertebra and the trapezius muscles below.
Hyoid bone: In anterior midline located at ~C3; palpable floating “U shaped” bone.
Good landmark for neck structures, and several cartilages of the larynx.
Consists of a body, 2 greater horns, and 2 lesser horns.
The hyoid does not articulate with other bones; instead, it attaches to many anterior neck muscles (suprahyoid and infrahyoid), and muscles of the larynx and pharynx.
Muscles of the neck
We start with muscles because many of them are landmarks for neck structures!!
Major neck boundary, separating the anterior triangle from the posterior triangle.
Origin
Mastoid process and superior nuchal line.
Insertion
Sternal head: round tendon to manubrium; clavicular head:medial 1/3 of clavicle.
Actions
Unilateral contraction produces lateral neck flexion and head rotated, so the face is turned toward the opposite side (contraction of right SCM tilts and rotates the head to the left).
Bilateral contraction produces neck flexion (chin to thorax).
innervation
CN XI.
Clinical correlation
Torticollis ("wry neck") is dystonia of the sternocleidomastoid muscle. Dystonia is defined as an involuntary sustained or spasmodic muscle contraction. This causes the patient's head to be turned and tilted to the side away from the affected muscle. It can be painful and debilitating since the head is turned to the side and can't be returned to its normal neutral position.
Most cases of torticollis are acquired. It can be caused by injury or inflammation of the SCM or cranial nerve XI, usually by blunt trauma or simple sleeping in an awkward position. Some cases may be neurodegenerative in nature, due to problems with the basal ganglia. Torticollis in infants (congenital) can be caused by trauma to the SCM in utero or during delivery.
Elevates, retracts, and rotates the scapula superiorly (details are the limb part of the course)—it is an important muscle for shoulder shrugging.
Boundary
Posterior boundary of the posterior (neck) triangle.
innervation
CN XI.
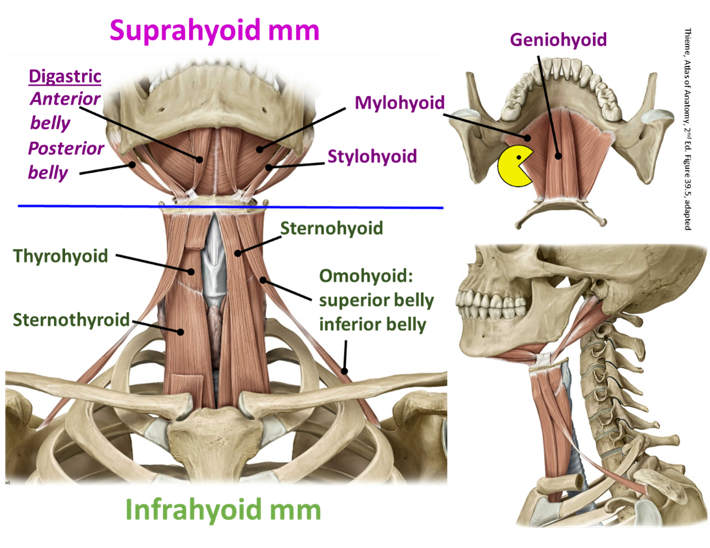
Suprahyoid muscles
Figure 2.
Attachments
Attach the hyoid bone to the mandible and temporal bones.
Boundary
Constitute the floor of the mouth.
Actions
Assist in opening the mouth.
innervation
Muscles of suprahyoid region, with innervations:
Digastric: Anterior and posterior bellies joined by a tendon that glides in a fibrous sling at the greater horn of the hyoid.
Anterior belly: Nerve to mylohyoid (from V3).
Posterior belly: Cranial nerve VII.
Mylohyoid (V3: nerve to mylohyoid).
Stylohyoid (VII): Splits around digastric tendon to attach to hyoid at the greater horn.
Geniohyoid (C1 nerve fibers, by hitching a ride on CN XII).
Infrahyoid muscles
Figure 3.
Attachments
Attach hyoid and larynx to sternum and scapula.
Actions
Are antagonists to suprahyoid muscles; depress the hyoid and larynx after having been elevated during swallowing. The infrahyoid and suprahyoid muscles work together to stabilize the hyoid so it can form a solid base for the muscles that move the tongue.
Muscles
Sternohyoid [ansa cervicalis (motor part of cervical plexus)]
Sternothyroid [ansa cervicalis (motor part of cervical plexus)]: Lies deep to the sternohyoid and attaches to the thyroid cartilage
Thyrohyoid (C1fibers, by hitching a ride on CN XII): Runs superiorly from the thyroid cartilage to the hyoid
Omohyoid [ansa cervicalis (motor part of cervical plexus)]: Two bellies (superior and inferior) connected by a tendon.
Neck lymphatic drainage
A brief intro
Figure 4. Lymph nodes of the neck. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG.8.193.
Superficial lymph nodes
Lie along the external jugular vein in superficial fascia, and drain scalp, occipital, mastoid,parotid, and superficial face regions. Drain into deep cervical lymph nodes.
Deep cervical lymph nodes
Lie deep to SCM, on the carotid sheath along the internal jugular vein.
Deep cervical nodes are grouped in two categories: Superior and inferior deep cervical nodes.
Supraclavicular nodes are the most inferior of the inferior deep cervical nodes. Lymph vessels that drain to these nodes often communicate with the thoracic duct or other large lymph trunks. Thus, lymph from other body regions may filter through supraclavicular nodes. Enlarged supraclavicular nodes are a bad sign—it may reflect metastasis of cancer from distant organs (lungs, stomach).
Deep cervical nodes are the ultimate repository for lymph from all regions of the head and neck. Lymph from the head percolates through other peripheral sets of nodes first before reaching the deep cervical nodes.
From deep cervical nodes, lymph drains into large jugular lymph trunks. These return lymph to the blood via the thoracic duct or right lymph duct, or by draining directly into the left and right venous angles.
Neck fascia
The neck has several fascial planes that contain many important structures.
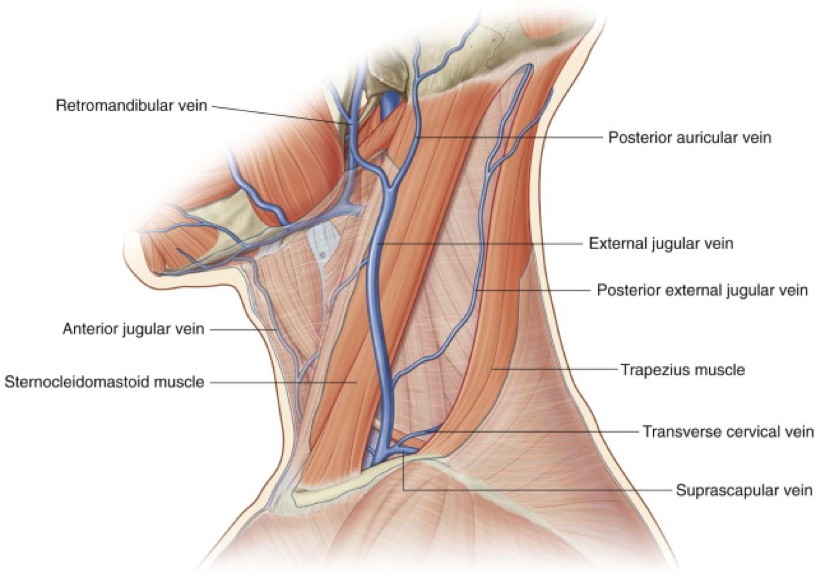
Figure 6. Superficial veins of the neck. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 8.181.
Superficial cervical fascia/subcutaneous tissue of the neck
Like all superficial fascia in the body, it contains loose connective tissue and cutaneous vessels and nerves. The superficial cervical fascia also contains the following:
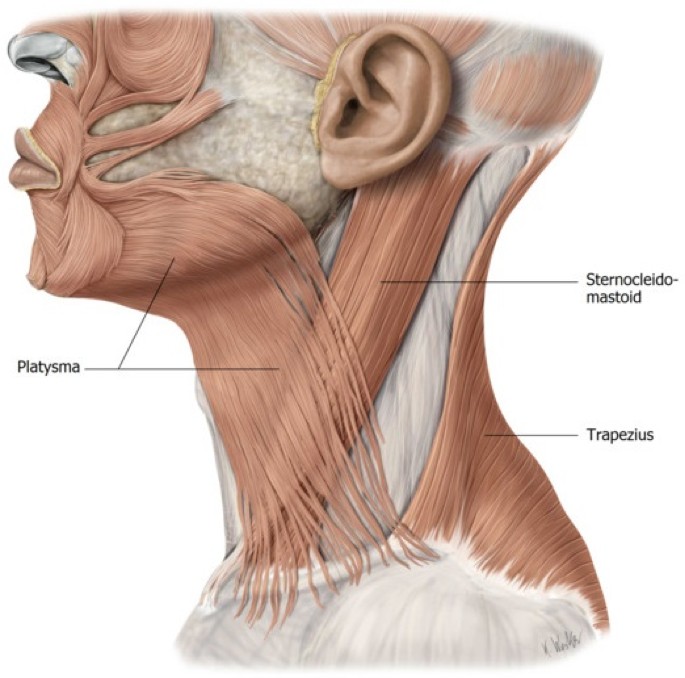
Platysma muscles: Thin grimace muscles; these are muscles of facial expression that blend with other facial muscles near the corners of the mouth.
Superficial veins
External jugular vein (EJV): Formed just below the angle of the mandible by the union of the retromandibular vein (posterior division) and posterior auricular vein.
Crosses outer surface of the SCM in the superficial fascia, just deep to the platysma.
Pierces the investing layer of deep fascia at the posterior border of the SCM, then descends to to the midpoint ofthe clavicle to join the subclavian vein.
Anterior jugular veins (usually left and right): Begin below the chin and pass inferiorly just lateral to the midline.They duck under the SCM and pass laterally to enter the EJVs.
The left and right anterior jugular veins often communicate via a venous arch that passes across the midline of the neck just above the manubrium. If present, it could cause bleeding problems during a tracheotomy procedure.
Clinical correlation
Superficial veins are clinically important in the diagnosis of impedance of venous return to the heart. In such cases, these veins become engorged and visible on the patient's neck.
Deep cervical fascia
Supports the viscera, muscles, vessels, and deep lymph nodes
Allows neck structures to move and glide past one another without difficulty (e.g. pass bolus down the pharynx, or when turning your head)
Fascial layers may be separated by pus or fluid accumulation, creating a connection where an infection may spread to another body region (e.g. to the mediastinum)
Natural cleavage planes used as guides during dissection and exposing surgical fields
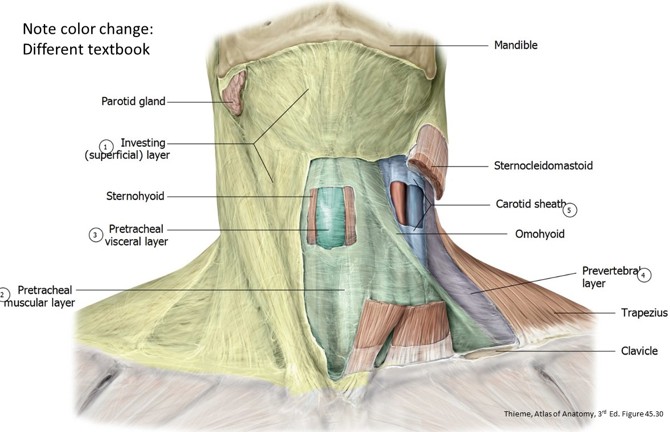
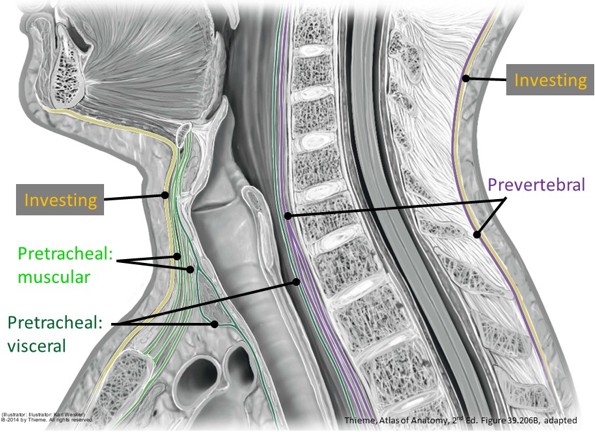
The deep cervical fascia has subparts with specific names. These enclose organs and muscle groups, forming a series of concentric rings, like those in a tree trunk. However, the layers of deep cervical fascia are connected in certain locations. The most important parts of the deep cervical fascia are:
Investing layer of deep fascia
Pretracheal fascia
Prevertebral fascia
Carotid sheath
Figure 7.
Figure 8.
Figure 9.
Investing fascia
Surroundstheentireneck just deep to the superficial fascia; forms a roof over the neck triangles
Splits to enclose the SCM and trapezius muscles
Attaches to the skull above, spines of cervical vertebrae posteriorly, and the sternum and clavicles below.
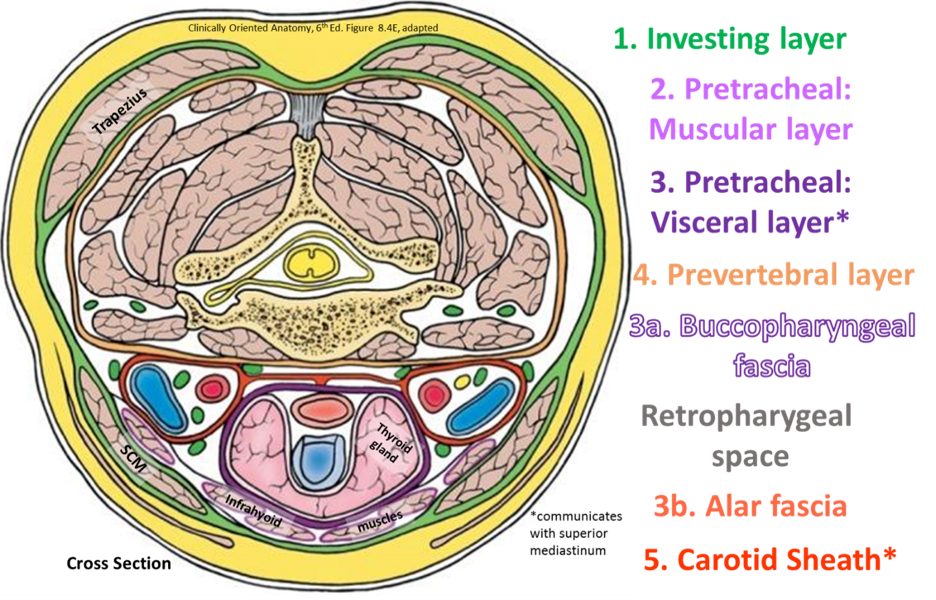
Pretracheal fascia
Limited to the anterior neck (meaning, anterior to the vertebrae)
Attaches to the hyoid bone and laryngeal cartilages superiorly and extends down into the mediastinum to blend with the fibrous pericardium in the thorax inferiorly
2 parts:
Muscular part: Thin and surrounds the infrahyoid muscles.
Visceral part: Surrounds the thyroid gland, trachea, and esophagus. This layer extends upwards to surround the pharynx, where it is called buccopharyngeal fascia.
Prevertebral fascia
Covers the prevertebral muscles anterior to the spine and the deep extensor muscles in the posterior neck.
Attaches to the base of the cranium and to the spinous processes and bodies of the cervical vertebrae
Passes along the spine into the posterior mediastinum inferiorly
Carotid Sheath
Formed by fusion of the other three layers of deep cervical fascia. Contents: Carotid arteries (common, internal, and external), internal jugular vein, vagus nerve, and nerve branches to the carotid body and sinus
Attached to the outer surface of the carotid sheath are deep cervical lymph nodes.
Fascial spaces
Potential spaces exist between the layers of deep fascia in the neck, around the pharynx, and in the floor of the mouth.
Retropharyngeal Space: between prevertebral and visceral pretracheal fasciae, this space is posterior to the pharynx and esophagus and anterior to the cervical vertebral bodies.
Allows movement of the pharynx, esophagus, trachea, and larynx during swallowing
Pretracheal space: Between infrahyoid muscles and trachea; can extend into mediastinum, where the pretracheal fascia blends with the pericardium
Lateral pharyngeal spaces (parapharyngeal spaces): adjacent to the lateral surfaces of the pharynx, between the pharynx and the muscles of the infratemporal fossa. This space communicates posteriorly with the retropharygeal space.
Clinical correlation
The take-home message with the potential spaces in the neck (between layers of deep cervical fascia) is they could provide routes for the spread of infection. The most important potential space is likely the retropharyngeal space. Infectious material in this space could track down into the mediastinum.
A good example here are peritonsillar abscesses—these occur deep to the palatine tonsils in an area adjacent to the parapharyngeal space (lateral pharyngeal space). These infections could enter the parapharyngeal space, then the retropharyngeal space.
The cervical plexus
The cervical plexus supplies motor and sensory branches to the neck, as well as giving rise to the phrenic nerves. The plexus is formed by the intermingling of nerve fibers from the ventral rami of spinal nerves C-1 to C-4. The ventral rami pierce the prevertebral fascia before joining to form the plexus.
Motor branches of the cervical plexus
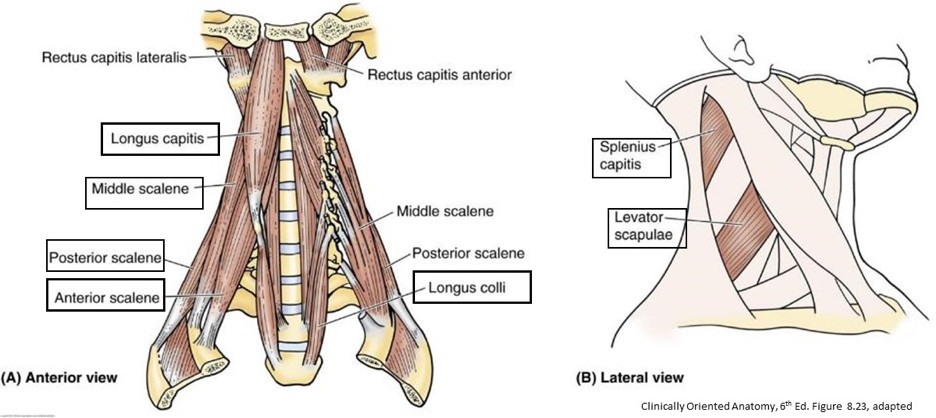
Phrenic nerves: These are old friends that we encountered previously in the thorax. They are formed by the ventral rami of C-3, C-4, and C-5, although technically only C-3 and C-4 are parts of the cervical plexus. The phrenic nerves descend on the anterior surfaces of the anterior scalene muscles at the root of the neck, then pass through the superior thoracic aperture into the thoracic cavity.
You know the rest of the story from here!
C-3, C-4, and C-5—Keep the diaphragm alive!
The phrenic nerves are motor to the diaphragm and sensory to the pericardium and parietal pleura (mediastinal and diaphragmatic portions).
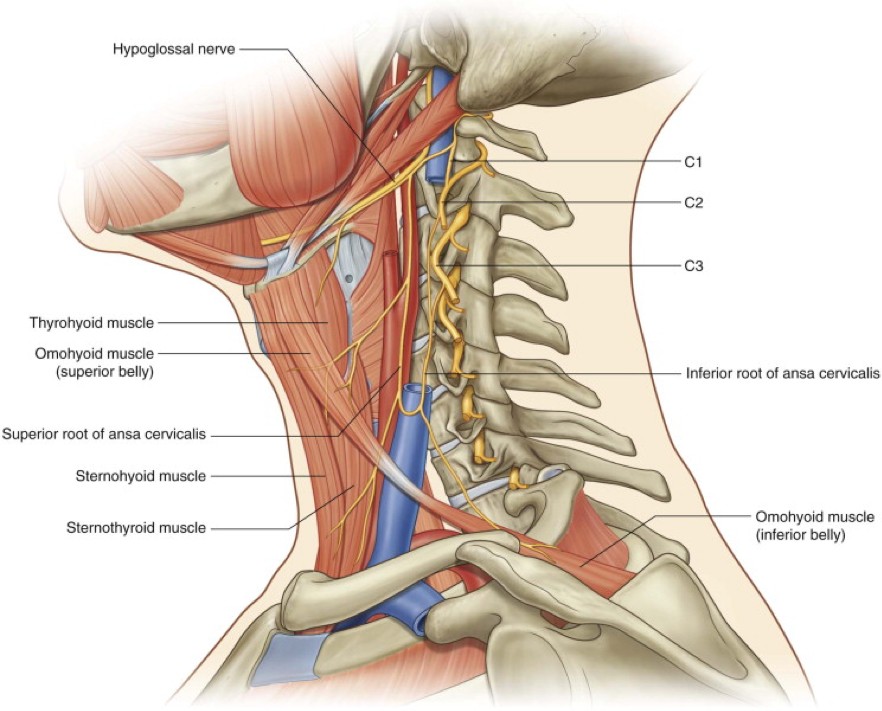
Ansa cervicalis: This nerve is formed from two roots:
A superior root derived from the ventral ramus of C-1.
An inferior root from C-2 and C-3 spinal nerves.
The superior root of the ansa “hitches a ride” with the hypoglossal nerve for a distance, before separating from it. The two roots descend along the carotid sheath and unite below to form a loop (ansa is Latin for “loop”). Motor branches from the ansa supply three of the four infrahyoid muscles:
Sternothyroid.
Sternohyoid.
Omohyoid.
Thus, the ansa supplies all infrahyoid muscles, except one = the thyrohyoid. C-1 fibers that also follow the hypoglossal nerve (but are not part of the superior root of ansa) separately innervate the thyrohyoid muscles.
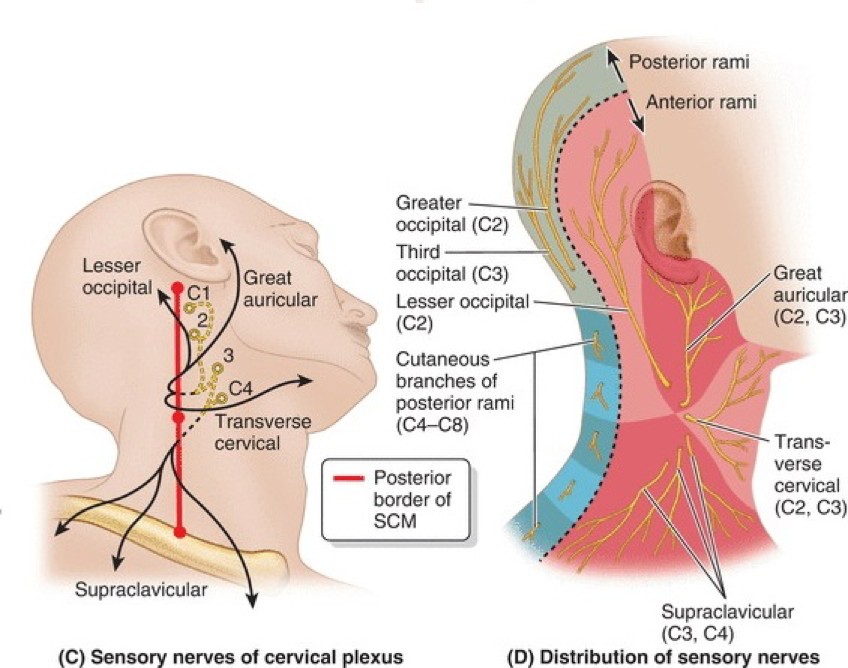
Sensory branches of the cervical plexus
Figure 11. Sensory nerves of the neck. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 8.183.
Figure 12. Cutaneous nerves of the neck. CLINICALLY ORIENTED ANATOMY, 8TH ED., FIG. 9.25A.
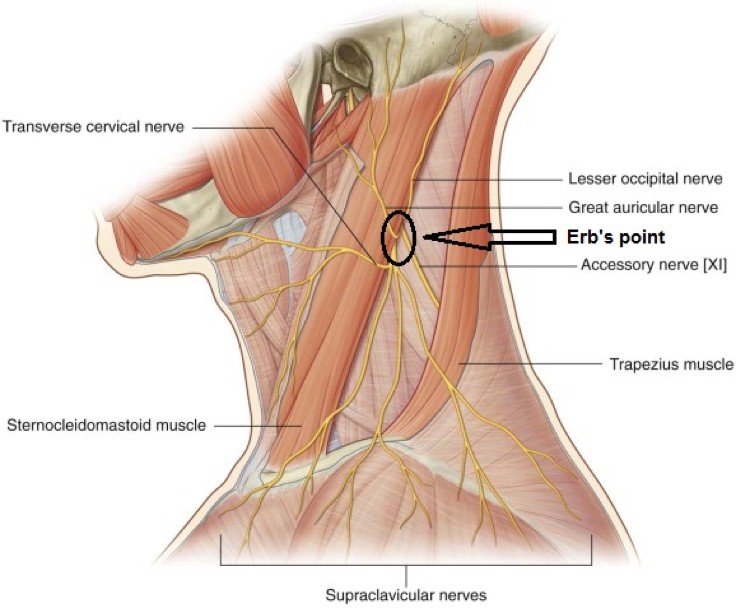
These emerge along the posterior border of the sternocleidomastoid, pierce the investing fascia, and then enter the superficial cervical fascia. Four branches:
1. Lesser occipital nerve (C-2)
Supplies the neck and scalp behind the external ear.
2. Great auricular nerve (C-2 and C-3)
Ascends vertically across the SCM, usually posterior to the external jugular vein,to skin over the parotid gland, external ear, and angle of the mandible.
3. Transverse cervical nerve (C-2 and C-3)
Crosses the SCM and penetrates the platysma, this nerve is the major sensory nerve of the anterior neck.
4. Supraclavicular nerves (C-3 and C-4)
Supply the skin at the base of the neck = over the clavicles and atop the shoulders.
Spasm of the diaphragm muscle produces pain signals that are transmitted in intercostal and phrenic nerves. Since the phrenic nerves originate in the neck, this “stich in your side” pain can also be referred to the C-3 and C-4 dermatomes (recall that these areas are supplied by the supraclavicular nerves). Indeed, runners with diaphragm spasms often complain of pain in their shoulders and neck.
Clinical correlation
All the sensory branches of the cervical plexus emerge from the deep neck and pass into the superficial fascia at a common location. This is Erb's point, located along the posterior border of the sternocleidomastoid, halfway between the mastoid process and the clavicle. Complete anaesthesia of the superficial neck can be obtained by injecting an anesthetic at Erb's point.
Triangles of the neck
The topography of certain neck muscles produces the borders of triangular spaces. These so-called neck triangles are useful for describing the locations of normal anatomical structures and pathologies in the neck.
Posterior triangle
Boundaries
Posterior: Anterior border of trapezius.
Anterior: Posterior border of SCM.
Inferior: Middle third of the clavicle.
Roof: Investing layer of deep cervical fascia.
Floor: Prevertebral fascia, covering the surfaces of prevertebral muscles.
contents
Arteries
The transverse cervical and suprascapular arteries(both from the subclavian artery) cross the triangle.
The third part of the subclavian artery is located at the base of the triangle, just posterior to the SCM, near the midclavicular point.Distal to this location, the subclavian artery becomes the axillary artery, supplying the upper limb. Downward pressure with fingers on the subclavian artery in the posterior triangle compresses the artery against the first rib. In an emergency, this is a pressure point for the control of bleeding in the upper limb.
Veins
External jugular vein: Enters the subclavian vein at the base of the triangle, just behind the SCM. It was described in the superficial fascia section
Nerves
Figure 13. CN XI in posterior triangle. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 8.170.
The Spinal Accessory nerve (Cranial nerve XI) crosses the center of the posterior triangle, after innervating the SCM.
As described earlier, Erb’s point is located halfway down the posterior border of the SCM. The supraclavicularnerves cross the posterior triangle within the superficial fascia.
Clinical correlation
The spinal accessory nerve is vulnerable within the posterior triangle. Lesions of CN XI may be caused by penetrating trauma, surgical error, or compression of the nerve by tumors or abscesses.
Hallmark sign of trapezius damage: "drooped shoulder" and inability to raise the limb above the shoulder (which requires rotation of the scapula, facilitated by the trapezius muscle).
The proximal parts of the brachial plexus (roots and trunks) pass through the base of the posterior triangle. The roots of the brachial plexus (C5–T1) exit between anterior and middle scalene muscles and descend between the 1st rib and clavicle,to enter the axilla. The roots will form trunks (upper, middle, and lower).
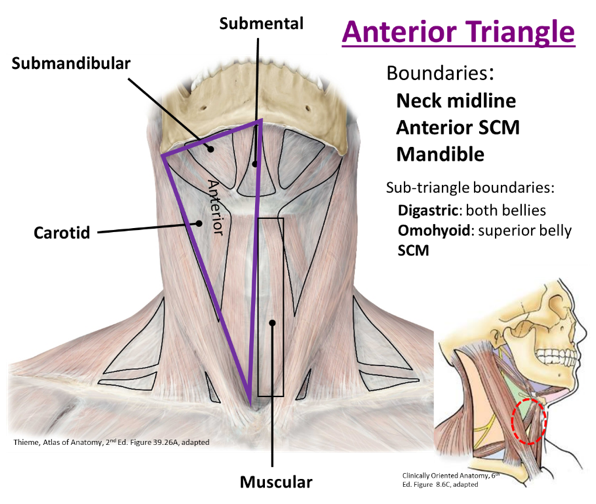
Anterior triangle
Boundaries
Medial: Anterior midline of neck
Posterior: SCM
Superior: Inferior border of the mandible
Recall the hyoid lies in the anterior triangle opposite C3. The anterior triangle above and below the hyoid bone are often called suprahyoid and infrahyoid regions, respectively.
Figure 14.
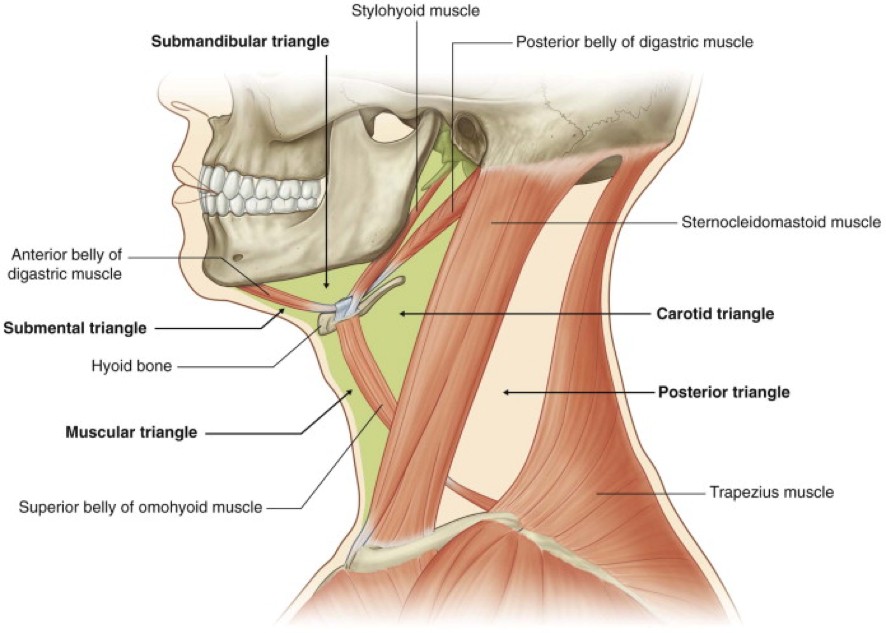
The anterior triangle is subdivided into four smaller triangles.
Figure 15. Triangles of the neck. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 8.162.
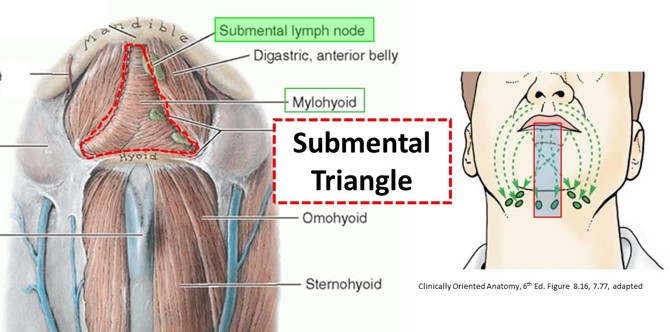
Submental triangle
This is the least important of the sub-triangles.
Figure 16.
Boundaries
Hyoid, mandible, and the right and left digastric anterior bellies. The floor is the 2 mylohyoid muscles.
contents
Submental lymph nodes and small veins that unite to form anterior jugular vein
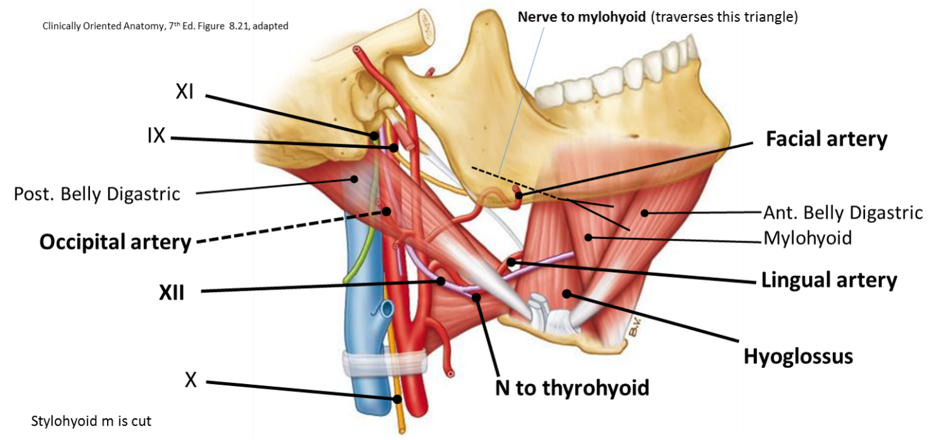
Submandibular triangle
Figure 17.
Boundaries
Anterior and posterior bellies of the digastric muscles and the mandible above. The floor is formed by the mylohyoid, hyoglossus, and middle pharyngeal constrictor muscles.
contents
Submandibular salivary gland and duct (fills most of the triangle)
Submandibular lymph nodes: receive lymph from the tongue and the oral cavity. Lesions in the mouth (like “canker” sores) can cause their inflammation (lymphadenopathy) and make them tender.
Cranial nerve XII: occipital artery twists around it; passes between mylohyoid and hyoglossus muscles
Nerve to mylohyoid (V3): innervates the digastric anterior belly and mylohyoid
Lingual artery: to the tongue
Facial artery: spirals around the submandibular gland, then crosses the mandible to reach the face.
Muscular triangle
Figure 18.
Boundaries
Neck midline, superior belly of the omohyoid, and anterior border of the SCM.
contents
Infrahyoid muscles and neck viscera
The floor muscles are reflected for surgical access to the thyroid gland, larynx, and trachea.
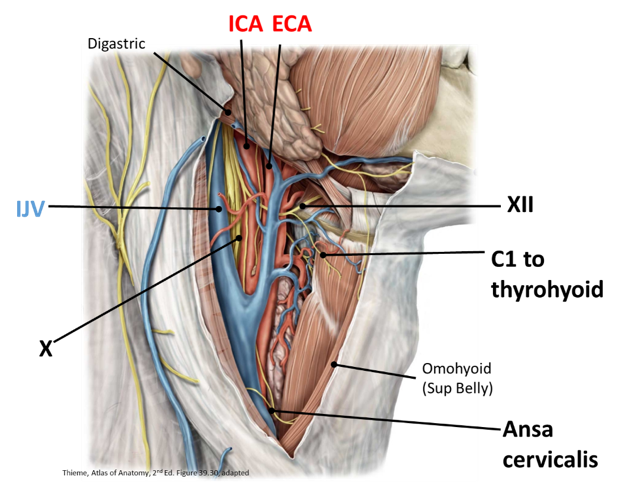
Carotid triangle
Boundaries
Digastric posterior belly, omohyoid superior belly, and anterior border of SCM. Its floor consists of the thyrohyoid, hyoglossus, and all three pharyngeal constrictor muscles.
contents
Common carotid artery, carotid bifurcation, carotid sinus and carotid body, ansa cervicalis;, deep cervical lymph nodes, internal jugular vein, vagus nerve (X), and hypoglossal nerve.
Clinical correlation
The carotid triangle is important for many reasons: taking a carotid pulse; and any surgical procedure to access the common carotid or its branches, internal jugular vein, the vagus or hypoglossal nerves. A procedure to remove atherosclerotic plaque from the carotid arteries (carotid endarterectomy) is done through the carotid triangle.
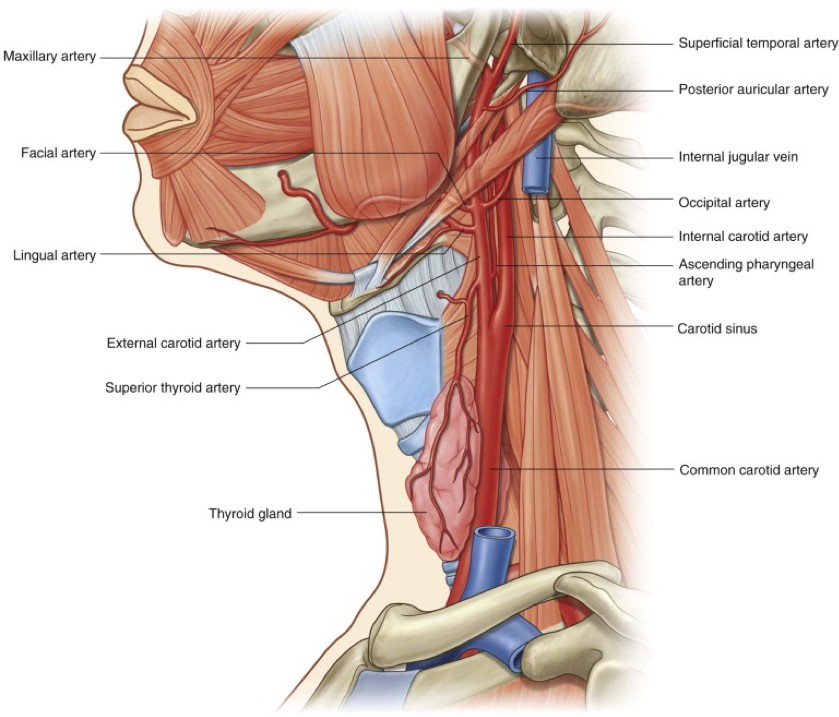
Overview of carotid arteries in the neck
Common Carotid Artery (CCA): Ascends and bifurcates at ~C-4 (superior border of the thyroid cartilage) into the internal carotid and external carotid arteries
Carotid sinus (baroreceptor): The enlarged, proximal portion of the internal carotid artery, just distal to the bifurcation; innervated by CN IX (carotid sinus nerve)
Carotid body (chemoreceptor): A small vascular structure, located outside the vessels, within the carotid bifurcation (“crotch”). Innervated by the carotid sinus nerve (CN IX).
Internal carotid (ICA): NO branches in the neck.
External carotid: Most branches originate in the carotid or submandibular triangles.
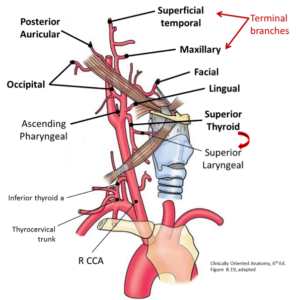
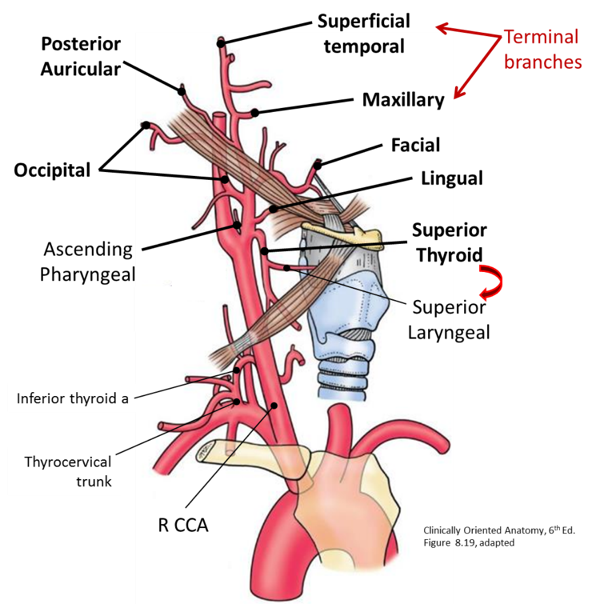
Figure 19.
Three anterior branches
Superior thyroid artery: Runs deep to the infrahyoid muscles and ends at the thyroid gland. It gives rise to the superior laryngeal artery (supplies the larynx).
Lingual artery: Passes deep to CN XII and the posterior belly of the digastric to enter the tongue deep to the hyoglossus muscle
Facial artery: Arises either in common with lingual artery or just superior to it. It passes deep to the digastric anterior belly, loops around and supplies the submandibular gland; then hooks around the middle of the inferior border of the mandible (feel pulse here) to enter the face. VERY curly Q!
Two posterior branches
Occipital artery: Passes posteriorly, immediately medial and parallel to the posterior belly of the digastric twisting around CN XII. Supplies the posterior scalp.
Posterior auricular artery: Passes behind the auricle (external ear), which it supplies, along with the posterior scalp.
One medial branch: The ascending pharyngeal artery arises from the medial side of the artery, just above the carotid bifurcation. It supplies the pharynx.
2 terminal branches: Maxillary and superficial temporal arteries. The superficial temporal artery supplies the scalp. The maxillary artery supplies cavities within the head and is discussed in later chapters.
It’s as easy as 1-2-3 to help you REMEMBER the branches of the external carotid!
1. Medial branch
2. Posterior branches
3. anterior branches
Then the terminal branches.
Figure 20. Branches of external carotid artery in the neck. GRAY’S ANATOMY FOR STUDENTS, 3RD ED., FIG. 8.167.
Overview of internal jugular vein
Receives blood from most of the head and neck, including the brain. The scalp and superficial neck are drained by the external jugular.
Begins at the jugular foramen and runs in the carotid sheath with the carotid arteries and CN X. It leaves the anterior triangle when it passes deep to the SCM.
Unites with the subclavian vein to form the brachiocephalic vein,posterior to the sternal end of the clavicle.
It is closely associated with the deep cervical lymph nodes.
Overview of vagus nerve in the neck
Pharyngeal branches: Motor to pharyngeal constrictor and soft palate muscles.
Superior laryngeal nerve, external and internal branches (internal pierces the thyrohyoid membrane with the superior laryngeal artery to enter the larynx): These supply the mucosa of the upper larynx and one muscle of the larynx. Discussed in detail on the Larynx page.
Cervical cardiac branches: Nerves to the heart arising in the neck. Why? Because of development, of course!
Recurrentlaryngealnerves: Both the left and right nerves pass through the neck, but only the right recurrent laryngeal originates from the vagus in the neck.
Ascend in the groove between trachea and esophagus to reach larynx.