PhD · Clinical Assistant Professor, Department of Translational Medicine & Physiology
Office: PBS 41C
Table of Contents
Optional reading
Clinically Oriented Anatomy, 9th ed., Head chapter, Internal surface of cranial base section through Posterior cranial fossa; Face and scalp section through Lymphatic drainage of face and scalp; Cranial meninges section through Arachnoid mater and pia mater; Cerebral arterial circle section and Venous drainage of brain section.
Scalp
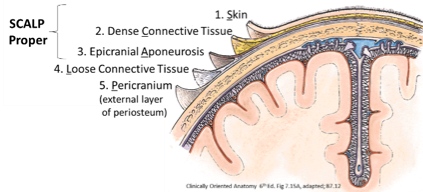
Figure 1.
The scalp covers the skull and extends from the supraorbital margins anteriorly to the nuchal lines posteriorly, and laterally to the zygomatic arches. The skin, connective tissue, and aponeurosis (SCA, layers 1–3 below) make up the scalp proper and are clinically considered one layer that are reflected together during a craniotomy, or when part of the scalp is torn off in an injury. From superficial to deep, the layers of the scalp are:
1. Skin
2. Connective tissue
Binds skin to the epicranial aponeurosis, ensheaths most of the blood vessels, and contains the nerves supplying the scalp.
3. Aponeurosis
Epicranial aponeurosis: 2 flat skeletal muscles attached to its anterior and posterior ends (the frontal and occipital parts of the occipitofrontalis muscle) move the scalp forward and backward. These muscles are innervated by the facial nerve (cranial nerve VII).
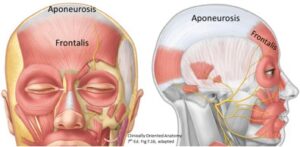
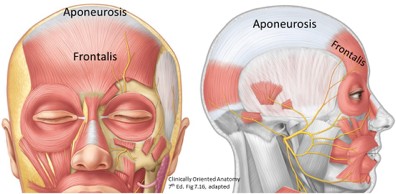
Figure 2.
Aponeurosis: When it is cut, the occipitofrontalis holds the wound open so lacerated arteries can’t retract. This is one of the reasons that scalp wounds bleed profusely. Superficial lacerations that do not extend to the aponeurosis are easily closed.
4. Loose connective tissue
Creates a potential space that allows movement of the scalp proper on the calvaria, and also can fill with fluid from injury or infection.
5. Pericranium (external layer of periosteum)
Clinical correlation
The epicranial aponeurosis is attached to bone posteriorly (via the occipitalis muscle) and laterally via temporal fascia. This seals the loose connective tissue layer of the scalp in these directions.
Anteriorly, however, the space is not sealed since the frontalis muscle inserts into skin and not bone. Blood in the loose connective layer could leak into the eyelids scalp injuries therefore can produce “black eyes.”
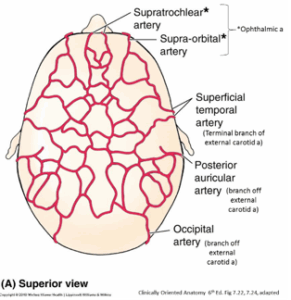
Arterial supply to scalp
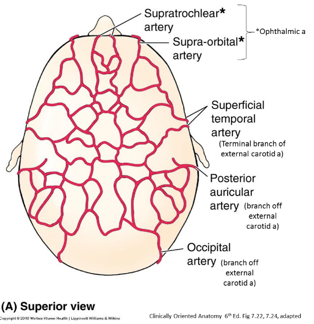
Figure 3.
Highly vascularized from vessels derived from both external and internal carotid arteries. From external carotid:
Superficial temporal
Posteriorauricular
Occipital
From internal carotid via the ophthalmic artery:
Supraorbital
Supratrochlear
Venous drainage of scalp
The scalp proper is drained by veins that accompany scalp arteries.
The deep scalp also drains into venous sinuses within the cranial cavity via small emissary veins. These pass through tiny holes in the calvaria. It is possible for scalp infections to enter the cranial cavity!
Innervation of the scalp
Figure 4.
Figure 5.
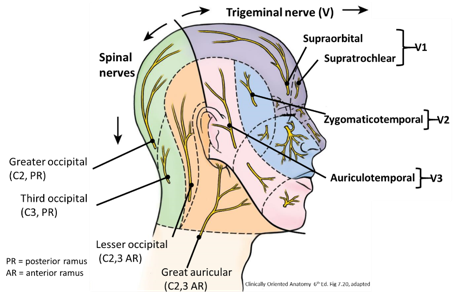
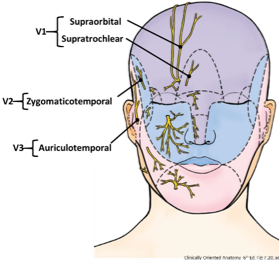
The skin is very sensitive. The cutaneous innervation is supplied by:
Supraorbital (V1), Supratrochlear (V1), Zygomaticotemporal (V2), and Auriculotemporal (V3)
Cervical plexus nerves, anterior rami: Lesser occipital and Great auricular (both C2,3)
Posterior rami cutaneous branches of C2 (Greater occipital) and C3 (Third occipital)
Occipitofrontalis muscle receives innervation via the facial nerve (cranial nerve VIII)
Lymph drainage of scalp
There are no lymph nodes in the scalp. Lymph drains into nodes at the junction between the head and neck. Most of the scalp drains into parotid, mastoid, and occipital nodes and then into the deep cervical lymph nodes located along the internal jugular vein (IJV).
Cranial cavity
Figure 6.
The cranial cavity is within the skull bones of the neurocranium and houses and protects components of the central nervous system. Theneurocranium is a box around the brain (including the meninges and some nerves and vessels) and is made of single frontal, sphenoid, ethmoid, and occipital bones; and paired parietal and temporal bones.
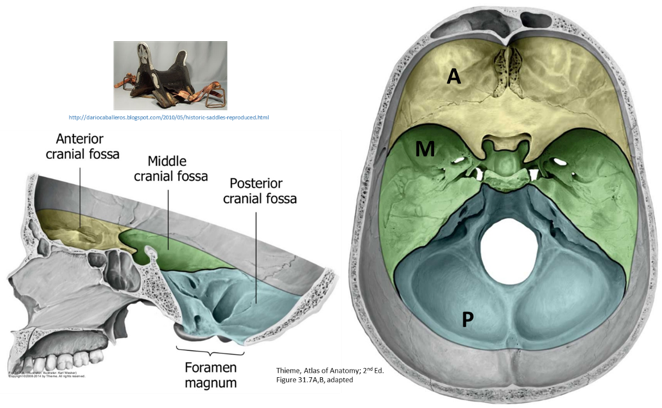
The cranial cavity contains three cranial fossae:
Anterior
Middle
Posterior
Anterior cranial fossa (ACF)
Shelf lying superior to the orbits and nasal cavity
Frontal bone: Orbital plates; ethmoid bone: cribriform plates, crista galli; sphenoid bone: lesser wings (posterior boundary of the ACF)
contents
The temporal fossa is occupied by the temporalis muscle and its fascia, nerves, and vessels.
Frontal lobe of the cerebrum
Olfactory bulbs lie on either side of the crista galli
Cranial nerve I axons pass through the cribriform plate. Fracture of the cribriform plate may result in anosmia, inability to smell, due to damage of the olfactory nerve fibers.
Middle cranial fossa (MCF)
Central portion of the cranial cavity
Sphenoid bone: Greater wings and body; temporal bone: petrous and squamous parts
contents
Temporal lobe of the cerebrum (between greater wing and petrous part)
Sella turcica (L=Turkish saddle): Central portion of the MCF
Boundaries: Anterior and posterior clinoid processes.
Parts: tuberculum sellae, hypophysial fossa, and dorsum sellae.
Content: Hypophysis (pituitary gland).
Posterior cranial fossa (PCF)
Largest and deepest fossa, mainly in the occipital bone
Dorsum sellae: separates the PCF from the hypophysial fossa
Clivus is the bony plate that slides down to the foramen magnum
contents
Occipital lobes of brain; cerebellum, pons, and medulla; tranverse and sigmoid dural sinus.
Meninges and dural venous sinuses
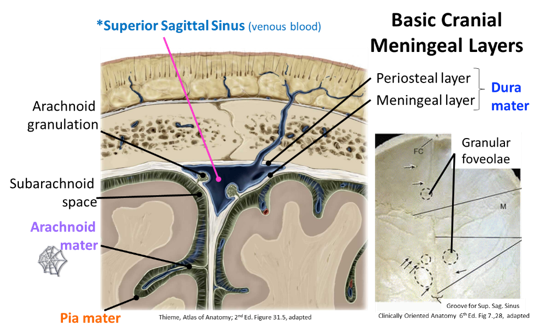
Figure 7.
Cranial meninges
The meninges are the coverings of the central nervous system. In the cranial cavity, the cranial meninges cover the brain and brainstem. The cranial dura mater is firmly attached to the bones of the cranial cavity.
Functions
Protection; blood vessel scaffolding; formation of venous sinuses; and formation of the continuous sac called the subarachnoid space (located between the arachnoid mater and pia mater), for the flow of cerebrospinal fluid.
Layers in the cranial cavity, from superficial to deep:
Dura mater
The tough outer fibrous layer
Arachnoid mater
The middle thin layer
Pia mater
The delicate inner layer, directly adherent to the brain
Dura mater
Two layers:
Periosteal (aka endosteal): The inner periosteum of the skull bones.
Meningeal: Same as that surrounding the spinal cord. It reflects away from the periosteal layer, forming partitions that separate the cranial cavity into compartments. The partitions include:
Falx cerebri: Between the two cerebral hemispheres, and attaches from the crista galli anteriorly to the occipital bone posteriorly
Falx cerebelli: In the posterior cranial fossa, separates the cerebellar hemispheres
Tentorium cerebelli: Forms a roof over the cerebellar hemispheres separating them from the occipital lobes. It attaches to the clinoid processes, petrous ridge of the temporal bone, and the occipital bone.
Tentorialnotch: Large gap anteromedially; allows the passage of the brainstem
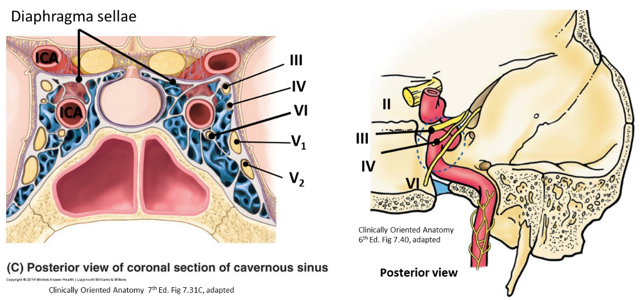
Diaphragma sellae: Doughnut-shaped meningeal dura forming the roof over the pituitary gland and has a small gap for the stalk/infundibulum of the pituitary gland
Figure 9. GILROY ET AL., ATLAS OF HUMAN ANATOMY, 2ND ED., THIEME PUBLISHERS, FIGURE 17.372A.
Dural sinuses: Endothelial lined spaces between periosteal and meningeal layers. They receive venous blood from the brain and skull.
Often you can see indentations of the sinuses on the skull itself (e.g., “groove for sigmoid sinus”).
Note again: Some venous sinuses receive emissary veins from the deep scalp.
Cerebral veins: Drain blood from the brain into the dural sinuses
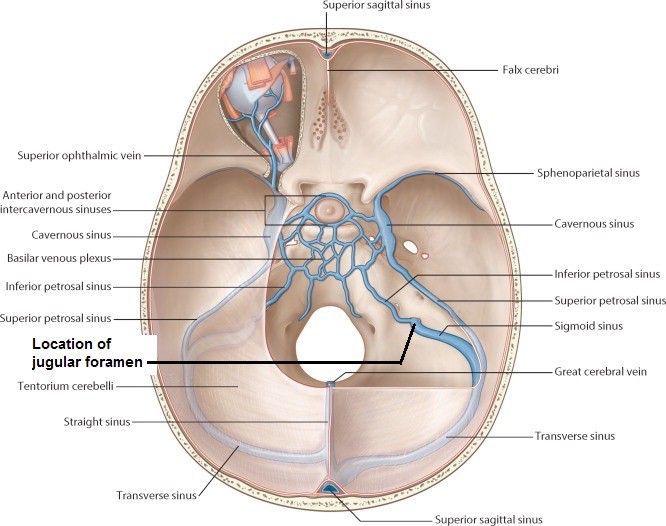
Jugular foramina: All dural venous sinuses drain here, where the internal jugular veins begin
Specific dural venous sinuses
Superior sagittal: Located in the superior margin of the falx cerebri
Arachnoid granulations: These are macroscopic collections of microscopic structures called arachnoid villi (see Figure 7). The villi are mushroom-cap shaped extensions of the arachnoid mater that protrude through the dura and into the superior sagittal venous sinus. They act as one-way valves that allow the cerebrospinal fluid in the subarachnoid space on top of the brain to enter the venous blood in the superior sagittal sinus. This returns CSF to the blood stream. CSF is a filtrate of the blood, formed when blood plasma leaves tufts of capillaries called the choroid plexus that are within the ventricles of the brain.
Inferior sagittal: Inferior margin of falx cerebri
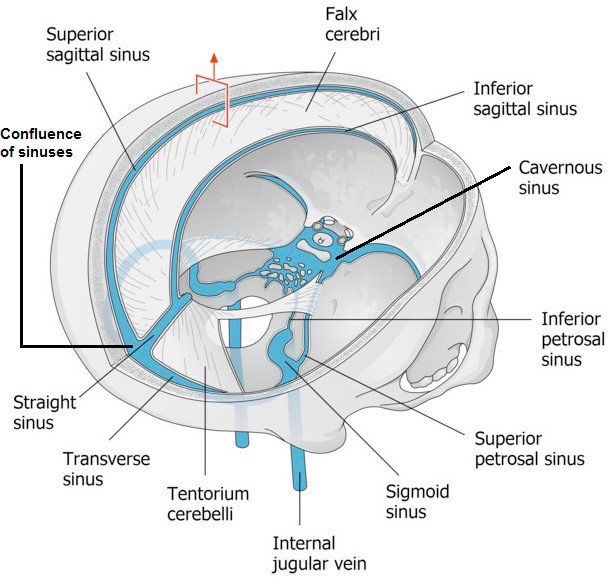
Straight: Superior margin of tentorium cerebelli at attachment of falx cerebri; ends posteriorly in the confluence of sinuses
Confluence of Sinuses: Convergence of straight, superior sagittal, and inferior sagittal, and occipital sinuses
Transverse: Runs forward from confluence of sinuses along occipital bone
Sigmoid: In posterior cranial fossa on temporal and occipital bones; continues inferiorly into internal jugular vein at jugular foramen
Occipital: In falx cerebelli; connects to internal vertebral plexus and confluence of sinuses
Superior petrosal: Along the upper ridge of petrous part of temporal bone; joins with the tranverse sinus to form the sigmoid sinus
Inferior petrosal: Runs inferiorly along the base of the petrous temporal bone—connects the cavernous sinus to the internal jugular vein within the jugular foramen
Cavernous: 2, located on either side of the sella turcica, posterior to the orbits
Interconnected cavities formed by connective tissue trabeculae that crisscross the sinuses, making blood flow sluggish
Connects to veins on the face via ophthalmic veins in the orbits
Cavernous sinus neurovascular relationships
Internal carotid arteries: pass through the sinuses and turn anteriorly. Note that venous blood is surrounding arterial blood in the cavernous sinuses. Odd!
Cranial nerves III, IV, V1, and V2are the lateral wall of the cavernous sinus. Cranial nerve VI is in the center of the cavernous sinus, bathed by venous blood!
FIgure 10.
Dura arterial supply
Middle meningeal artery: A branch of the maxillary artery. The middle meningeal artery is the primary blood supply to the calvaria and an important source to the dura mater associated with it.
Dural sensory innervation
Branches of all three divisions of trigeminal nerve
Branches from the upper cervical spinal nerves
Vagus nerves
Referred pain arising from the dura is one cause of headaches.
Clinical correlation
Under pathological conditions (usually due to trauma), an epidural or subdural space may be created and filled with blood.
A hematoma is a collection of blood outside of a blood vessel. An epidural hematoma occurs when an artery is ruptured by violent force (usually the middle meningeal artery), causing blood to collect between the dura mater and skull. When seen on CT, the hematoma is biconcave lens-shaped, since the blood tears the dura off the inside of the skull, but usually does not cross skull bone sutures (the joints between bones), since the dura is firmly attached here. A subdural hematoma occurs when “bridging veins” (cerebral veins that pass from the brain, penetrate the arachnoid and dura, and enter the venous sinuses) are lacerated. Bridging veins are so named since they cross (“bridge”) the subarachnoid and subdural spaces. Tearing of the veins occurs where they penetrate the fixed dura mater around the venous sinuses. This allows blood to pour into the subdural space. When seen on CT, a subdural hematoma is crescent-shaped, since it is not constrained by dural attachments to the inside of the skull.
Arterial supply to the brain
Figure 11.
The brain is highly sensitive to glucose and oxygen levels in the blood. To guarantee adequate blood supply to the brain, an anastomosis of two major arteries occurs at the base of the brain—this is the circle of Willis.
Internal carotid (ICA) and vertebral arteries: Two pairs of arteries supplying the brain itself.
ICA enters the cranium via the carotid canal and traverses the cavernous sinus as mentioned previously
Basilar artery: Runs along the clivus on the pons; formed by the two vertebral arteries that enter through the foramen magnum
Cerebral arterial circle (circle of Willis): Communication between the basilar and both internal carotid arteries
The Circle of Willis is composed of the anterior and posterior cerebral arteries; and the anterior and posterior communicating arteries