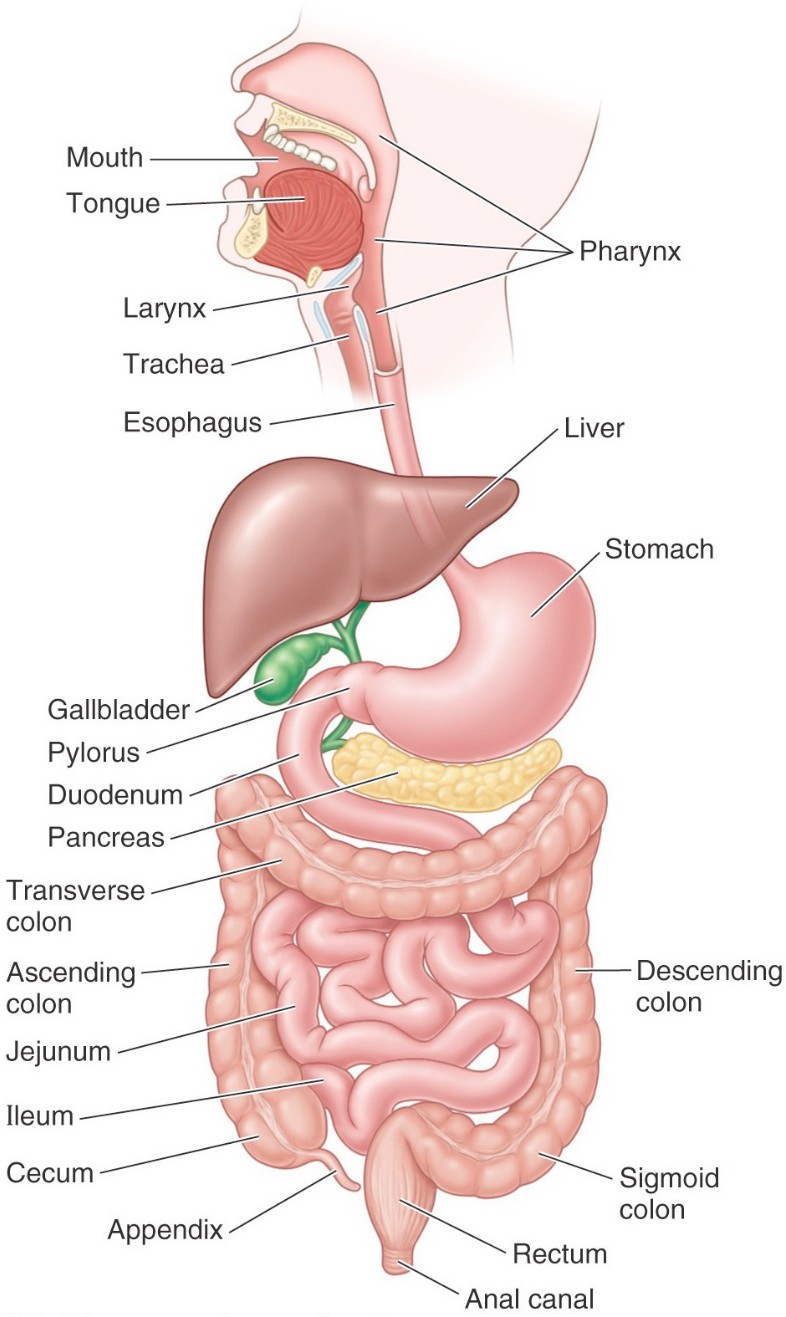
Figure 1. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, FIGURE 2.31.
As always, understanding the development of the body’s organ systems and parts illuminates their gross anatomy. The definitive anatomy of digestive organs in the abdomen is a perfect example. The embryo starts out with a simple straight tube in the 4th week, then it elongates, twists, and moves around within the abdominopelvic cavity. These processes produce the characteristics of gut topography, such as the position of the stomach with the lesser sac behind it, the location of the pancreas within the curvature of the C-shaped duodenum, the close association between liver and diaphragm, and the arrangement of the colon as an “inverted box” around the coils of small intestine.
The colon, a subpart of the large intestine, forms a square “box” around the small intestine.
Accessory organs
Salivary glands
Secrete saliva into the oral cavity.
Liver
Gall bladder
Stores bile. Connected to the liver and duodenum by bile ducts.
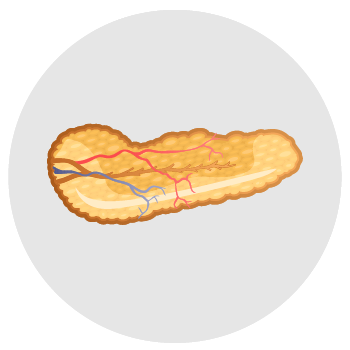
Pancreas
Has both exocrine and endocrine functions. Snuggled up within the concavity (“C”) of the duodenum and connected to it by one (or two) pancreatic duct(s).
The spleen is not a digestive organ.
It develops within the abdominal cavity in close proximity, so it shares blood supply with GI tract organs in the upper abdomen.
Review: Folding during Week 4 produces a “tube-within-a-tube” body plan
Figure 2. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 6.18.
Longitudinal and transverse folding of the trilaminar embryonic disc produces a cylindrical tadpole-shaped embryo with a body wall and body cavity. But you already knew that!
Folding internalizes the endoderm, rolling it into an elongated tube within the embryo’s body cavity.
Splanchnic mesoderm surrounds the endoderm. This endoderm-splanchnic mesoderm tube becomes the digestive tube—it is initially attached to the dorsal body wall by a broad dorsal mesentery. The gut tube ends blindly cranially and caudally, until the oropharyngeal membrane ruptures during Week 4 and the anal membrane ruptures during Week 8.
Germ layers that produce the digestive tube
Endoderm gives rise to the inner epithelium that lines the lumen of the gut tube, as well as its intrinsic glands,and to the parenchyma (functional parts) of the solid accessory organs of the gut in the abdomen (liver and pancreas).
Interestingly, there is no lumen in the primitive gut tube early on as it becomes occluded during the 6th week by rapid proliferation of endodermal cells. A few weeks later, the gut tube recanalizes to create a lumen. If this does not happen correctly, stenosis of parts of the gut tube can occur.
Splanchnic mesoderm gives rise to all the other layers of the gut tube = connective tissue and smooth muscle layers, plus the outer serosa (visceral peritoneum). The dorsal mesentery also comes from splanchnic mesoderm, as does the stroma (supporting tissue) of organs like the liver and pancreas.
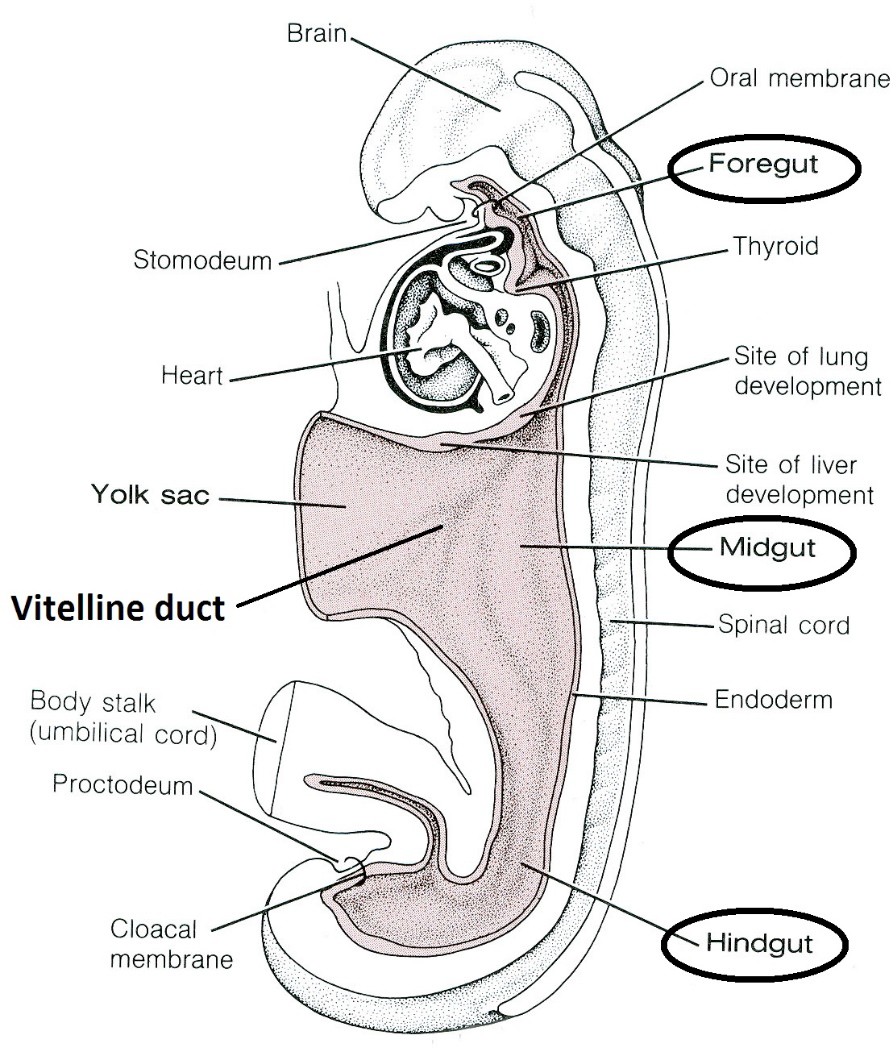
Regions of the primitive digestive tube: Foregut, midgut, and hindgut
Figure 3. Regions of primitive gut tube. LARSEN’S HUMAN EMBRYOLOGY, 5TH ED., FIGURE 14-4.
Figure 4. SPENCE, BASIC HUMAN ANATOMY, 2ND ED. (BENJAMIN-CUMMINGS PUBLISHING).
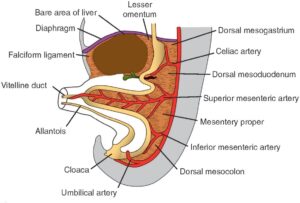
Recall that folding of the embryo extrudes the yolk sac from the embryo, where it later withers away. Within the umbilical cord, a tubular connection made of endoderm remains between the primitive gut tube within the embryo and the extruded yolk sac—this connection is the vitelline duct (some embryologists call it the yolk stalk). The vitelline duct normally obliterates after a few months. It is a useful landmark in our story of digestive tube development as we shall see. Note that after folding, the embryonic gut tube and vitelline duct produce a shape resembling the letter T.
After body folding, the cranial and caudal parts of the gut are blind-ended tubes. These are called the foregut and hindgut, respectively.
The foregut terminates cranially at the oropharyngeal membrane. Caudally it ends where the duct from the liver (bile duct) enters the halfway point of the duodenum.
The hindgut terminates caudally at the cloacal membrane.
The central part of the gut tube where the vitelline duct is attached is termed the midgut.
Understanding the three parts of the primitive gut tube and the organs and structures derived from each is useful for understanding the blood supply, lymphatic drainage, and innervation of the definitive digestive tract.
The celiac trunk supplies blood to foregut derivatives in the abdomen.
The superior mesenteric artery to structures derived from the midgut.
The inferior mesenteric artery to those parts derived from the hindgut.
Who says embryology doesn’t make sense?
Clinical correlation
Persistence of all or part of the vitelline duct can produce an Ileal (Meckel's) diverticulum in the small intestine. This anomaly can be remembered using the "Rule of Twos":
2% of infants have it
Located 2 feet proximal to the end of the ileum (ileocecal junction)
2 inches long
2 times more common in males than females.
When symptoms occur, they can include bleeding and intestinal obstruction. Symptoms can mimic appendicits. Ectopic tissue (gastric, for example) can be prsent in the diverticulum. Oh yeah, symptoms occur in about 2% of people having a Meckel’s diverticulum.
Table 1. Summary: Adult derivatives of the primitive gut
Embryonic region
Gut tube parts
Accessory organs
FOREGUT
Pharynx
Esophagus
Stomach
Proximal half of duodenum
Pharyngeal pouches and their derivatives
Thyroid gland
Lungs, bronchi, and trachea
Liver parenchyma
Gallbladder and bile ducts
Pancreas
MIDGUT
Distal half of duodenum
Jejunum
Ileum
Cecum
Appendix
Ascending colon
Proximal ⅔ of transverse colon
HINDGUT
Distal ⅓ of transverse colon
Descending colon
Sigmoid colon
Rectum
Upper ½ of anal canal
Urinary bladder
Urethra
Mesenteries suspend portions of the digestive tube within the abdominal cavity
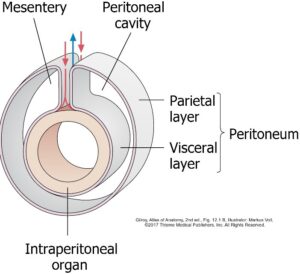
Figure 5.Peritoneum is a serous membrane.
Parietal peritoneum lines the walls of the abdominal cavity and dips down into the pelvic cavity too where it drapes over pelvic organs.
Visceral peritoneum is on the outer surface of abdominal organs—in fact, it is the outer layer of the organ itself.
The peritoneal cavity is between the two layers. It has two parts: greater and lesser sacs.
A mesentery is a double layer of peritoneum (with adipose and areolar tissue sandwiched in between) that attaches organs to the body wall. Visceral peritoneum becomes continuous with parietal peritoneum in mesenteries. Mesenteries support organs and provide a conduit for nerves and blood vessels to reach organs from the body wall. Mesenteries also allow organs to have mobility, so they can move during the activities of peristalsis.
Omenta and peritoneal ligaments are also double-layered peritoneal structures that connect organs to the abdominal wall and to one another. Omenta are associated with the stomach.
Review: Formation of dorsal and ventral mesenteries and the peritoneal cavity
Lateral folding of the embryo brings together the left and right limbs of the intraembryonic coelom that are caudal to the septum transversum (we called these coelomic ducts, remember?) and wraps them around the primitive gut tube, like two balloons pushed together with a hose in between them.Fusion of the coelomic ducts produces the peritoneal sac.
Ventral to the gut tube, in the region of the midgut and hindgut, the two coelomic ducts fuse completely. In cross-section, the peritoneal cavity in these regions is shaped like the letter U.
Dorsal to the gut tube, the coelomic ducts don’t fuse, so that the left and right sides of the peritoneal cavity are separated by a double layer of splanchnic mesoderm = the dorsal mesentery. This supports the primitive gut tube. See Figure 6.
Figure 6. Midgut and hindgut: Dorsal mesentery only. MOORE ET AL., THE DEVELOPING HUMAN, FIGURE 8.3.
Figure 7. Foregut: Dorsal and ventral mesenteries. MOORE ET AL., THE DEVELOPING HUMAN, FIGURE 8.3.
In the region of the foregut where the stomach and liver develop, the septum transversum prevents the fusion of the coelomic ducts ventral to the gut tube.
The caudal part of the septum transversum connects the abdominal foregut to the ventral body wall; so it is therefore termed the ventral mesentery. As the liver develops, it will partition the ventral mesentery into two parts:
One connecting the stomach to the liver
The other attaching the liver to the ventral body wall. See Figure 7. Remember, there is NO ventral mesentery in the region of the midgut and hindgut.
Elongation and rotation of the digestive tube in the abdomen during development destroys the simple arrangement of gut tube connected to the dorsal body wall by a dorsal mesentery. The result is that only some abdominal organs in the adult are suspended from the body wall by mesenteries. Others become secondarily fused to the dorsal body wall as their dorsal mesentery is obliterated.
Intraperitoneal organs
In the adult, organs that have mesenteries are almost completely surrounded by visceral peritoneum, except for the area where the stalk of the mesentery joins the organ. These organs are said to be intraperitoneal. Note that this doesn’t mean they are within the peritoneal cavity—they aren’t, since the peritoneal cavity is the potential space between parietal and visceral layers of peritoneum. Do you see that the entire primitive gut in the embryo was intraperitoneal to begin with?
Retroperitoneal organs
Some non-digestive organs in the AP cavity originally develop in the posterior body wall and are dorsal to the peritoneal sac. These organs are said to be retroperitoneal. The kidneys and suprarenal glands are examples. Clinicians and anatomists often say these organs are located in the “retroperitoneum.”
Parts of the gut tube that were once intraperitoneal (suspended by the dorsal mesentery) later become fused to the body wall due to elongation and rotation of the gut. Although they resemble other retroperitoneal organs, they are actually classified as secondarily retroperitoneal, since they once had a mesentery. The obliteration of the mesentery dorsal to the organ (see Figure 8) produces what is called fusion fascia, a connective tissue plane between organ and body wall. Surgeons can mobilize secondarily retroperitoneal organs by incising the peritoneum adjacent to the organ and then dissecting along the fusion fascia plane.
Figure 8. LARSEN’S HUMAN EMBRYOLOGY, FIGURE 14-3.
Development of the abdominal foregut
Stomach
During Week 5, the foregut elongates to produce a lengthy thoracic esophagus and it moves the presumptive stomach away from the lung buds. The part of the foregut just below the septum transversum becomes fusiform (spindle-shaped). This is the first indication of the stomach’s location.
The dorsal wall of the stomach grows faster than its ventral wall.
A greater curvature develops dorsally and lesser curvature ventrally.
The dorsal mesentery attaches to the greater curvature and the ventral mesentery to the lesser curvature.
The stomach has left and right surfaces at this stage.
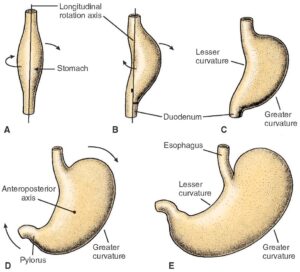
Figure 9. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 15.8.
During the 7th week, the stomach rotates 90 degrees clockwise around a longitudinal axis (as viewed from above), so that the original left side now faces anterior and its right side faces posterior. The lesser curvature now faces to the right while the greater curvature faces downward and to the left. This gives the stomach its classic J shape (when empty). This rotation explains why the left vagus nerve ends up on the stomach’s anterior surface and the right vagus nerve on the posterior surface.
The stomach also rotates around an anterior-posterior axis, such that it tips the future pylorus upwards.The stomach takes on a “steer horn” appearance, with the esophagus and pylorus forming the two horns.
Figure 10.
Structural changes in the stomach’s dorsal mesentery progressively move its attachment to the dorsal body wall from the midline toward the left side. This, along with rotation of the stomach, cause the dorsal mesentery of the stomach (= the definitive greater omentum) to connect the greater curvature to the dorsal body wall in a curved orientation (letter J), stretching from the pancreas to the left kidney and on up to the diaphragm where the esophagus enters the abdomen, rather than a vertical attachment in the midline, as it was in Week 4. See Figure 10. Development of the greater omentum will be discussed in more detail later.
Rotation of the stomach also influences the ventral mesentery that attaches from its lesser curvature to the developing liver. After rotation, the lesser omentum, like the stomach, is oriented vertically in the coronal plane.
Rotation of the stomach and development of its curvatures bends the presumptive duodenum into its classic C shape and moves it to the right side and posterior until most of it fuses to the dorsal body wall to become secondarily retroperitoneal. Only the first part of the duodenum is intraperitoneal (attached to the lesser and greater omenta).
Figure 11.
Rotation of the stomach and duodenum produces a cul-de-sac of the peritoneal cavity dorsal to the stomach and lesser omentum. This is the lesser sac (a.k.a. omental bursa). The rest of the peritoneal cavity is called the greater sac. The two sacs communicate through a small aperture that is posterior to the vertical edge of the lesser omentum = the omental foramen (foramen of Winslow). Do you see that the omental foramen is oriented so that it opens to the right? The omental foramen is the only window to the lesser sac.
Liver and gallbladder
The liver develops from the distal part of the foregut, growing out of the middle of the future duodenum. It forms initially as an outpocketing of endoderm cells called the hepatic diverticulum. Stomach rotation positions the primordial liver on the right side.
Figure 12. LARSEN’S HUMAN EMBRYOLOGY, FIGURE 14-9.
The hepatic diverticulum grows into the septum transversum, which you will recall is a mass of mesenchyme inferior to the developing heart. The hepatic diverticulum remains connected to the distal foregut by the hepatic duct. Cells of the hepatic diverticulum give rise to the functional cells of the liver (= the hepatocytes) as well the small bile carrying ducts within the liver (= bile canaliculi).
As the liver grows cranially, mesenchymal cells of the septum transversum infiltrate the cords of cells in the hepatic diverticulum to produce the connective tissues supporting the liver (= the liver stroma). Mesenchyme of the septum transversum also surrounds the developing liver to form its visceral peritoneum. Recall that the septum transversum also forms the central tendon of the diaphragm which is just cranial to the liver. When the liver makes contact with the developing central tendon, it fails to acquire a layer of visceral peritoneum here, thus this region of the liver is known as the bare area. The reflections of visceral peritoneum from the liver onto the inferior surface of the diaphragm encircle the bare area like a “crown” = thus they are known as coronary ligaments.
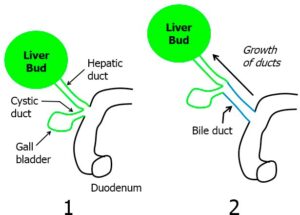
Figure 13. HAND-DRAWN CONLEY-GRAM.
Meanwhile, back at the duodenum, another outgrowth of endoderm called the cystic diverticulum develops just adjacent to the hepatic duct. The cystic diverticulum and surrounding splanchnic mesoderm give rise to the gall bladder and the cystic duct. Afterwards, cells at the junction of the cystic duct and hepatic duct proliferate and grow producing another duct = the common bile duct. Growth of the common bile duct moves the gallbladder and cystic duct cranially away from their attachment to the duodenum. These processes produce the definitive branched arrangement of major bile ducts. See Figure 13.
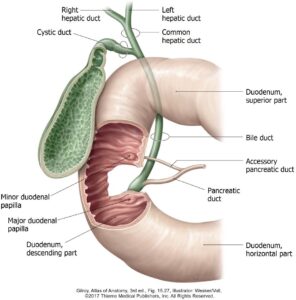
Figure 14.
The hepatic duct and cystic diverticulum originally sprouted from the ventral side of the duodenum. Rotation of the stomach and movement of the duodenum and liver to the right twisted these structures and displaced them, so that in the adult the common bile duct passes posterior to the first part of the duodenum and then connects to its second part (called the descending duodenum) on the left side, joining the main pancreatic duct as it does so. Thus, the major duodenal papilla opens internally on the medial wall of the 2nd part of the duodenum. This is where bile and pancreatic juice enters the gut.
Pancreas
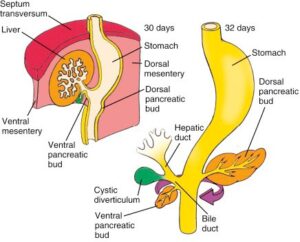
The pancreas begins its development in Week 4 from the distal foregut as two glands, but ends up in the adult as one.
The dorsal pancreatic bud is an endodermal diverticulum that grows dorsally from the future duodenum into the dorsal mesenteryopposite the hepatic diverticulum.
Figure 15. MOORE ET AL., THE DEVELOPING HUMAN, FIGURE 11-10.
A second endodermal diverticulum, the smaller ventral pancreatic bud, sprouts ventrally from the foregut just caudal to the location of the cystic diverticulum.
Pancreatic exocrine cells that produce digestive enzymes, as well as pancreatic endocrine cells (islet cells) that produce hormones (such as insulin and glucagon) all develop from endoderm.
The dorsal pancreatic bud is fixed within the dorsal mesentery. Rotation of the stomach and duodenum moves the ventral pancreatic bud and bile duct from the ventral side of the duodenum to a dorsal location, and then finally to the left. The two buds fuse to form the definitive pancreas within the concavity of the duodenum. The dorsal pancreatic bud gives rise to the head, body, and tail of the pancreas, while the ventral pancreatic bud gives rise to the hook-shaped uncinate process.
Figure 16. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 15-20.
Within each bud, a system of branched exocrine ducts and a main duct develop. The two main ducts connect to the duodenum independently. Within the pancreas, fusion of the dorsal and ventral ducts produces a single S-shaped main pancreatic duct, emptying with the bile duct in the duodenum on the major duodenal papilla. In some cases the proximal part of the dorsal duct persists and remains connected independently to the duodenum. If present, this is called the accessory pancreatic duct.
Clinical correlation
In rare cases, an anular pancreas encircling the descending duodenum (second part) may develop.
This is caused by the formation of a bifid ventral pancreatic bud. These buds rotate in opposite directions around the duodenum, forming a ring of pancreatic tissue that fuses with the dorsal bud. An anular pancreas can cause duodenal obstruction.
Figure 17. LARSEN’S HUMAN EMBRYOLOGY, ED., FIG. 4-11.
Fate of the ventral mesentery of the foregut
Figure 18. LARSEN’S HUMAN EMBRYOLOGY, FIGURE 14-13.
The caudal-most part of the septum transversum is known as the ventral mesentery of the foregut. It connects the lesser curvature of the stomach and first part of the duodenum to the ventral body wall. Recall that the cranial part of the septum transversum gives rise to the central tendon of the diaphragm. Recall also that the hepatic diverticulum grows into the center of the ventral mesentery, where the liver develops.
The part of the ventral mesentery between the developing liver and the ventral body wall thins out to become the falciform ligament. As the ventral body wall elongates vertically, the falciform ligament elongates too, producing its characteristic “sickle” shape. The caudal margin of the falciform ligament transmits the umbilical vein from the body wall to the liver.
The portion of the ventral mesentery between the liver and foregut thins out to form the lesser omentum. The portion of the lesser omentum between the liver and first part of the duodenum is the hepatoduodenal ligament. It contains the portal vein, hepatic artery proper, and the common bile duct (= the portal triad). The portion of the lesser omentum connecting liver and stomach is the hepatogastric ligament. Rotation of the stomach and duodenum cause the lesser omentum to move from its original orientation in a sagittal plane, to its definitive orientation in a coronal plane.
Development of the midgut
Figure 19. CLEMENTE, REGIONAL ATLAS OF THE HUMAN BODY, FIGURE 234.
Recall that the midgut region of the primitive gut tube is recognized by its attachment to the vitelline duct, which leaves the body cavity via the umbilicus to enter the umbilical cord and attach to the yolk sac.
Figure 20. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 15.4.
During the 5th week, the midgut grows extensively and elongates such that it produces a hairpin loop (the primary intestinal loop) with the vitelline duct situated at the apex of the loop. The dorsal mesentery tethers the loop to the dorsal body wall and the superior mesenteric artery runs through the dorsal mesentery along the axis of the loop to its apex.
The cranial part of the primary intestinal loop will give rise to the distal part of the duodenum, the jejunum, and most of the ileum = essentially the “coils” of the small intestine.
The caudal part of the loop gives rise to the cecum, ascending colon, and most of the transverse colon. A swelling or “bump” in the caudal loop (called the cecal primordium), just distal to the attachment of the vitelline duct, locates the future cecum and appendix, and this is a useful landmark for us for locating the junction of small intestine and large intestine.
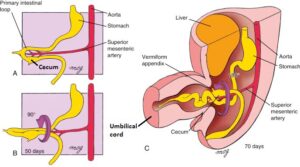
Figure 21. “Physiological herniation” of midgut as it rotates 90 degrees counter clockwise; then 180 degree rotation as the midgut loop “retracts” from the umbilical cord. LARSEN’S HUMAN EMBRYOLOGY, FIGURE 14-14.
The primary intestinal loop becomes too large to fit in the peritoneal cavity and pressure put on the loop by the developing liver forces it to herniate through the umbilicus into the umbilical cord. Yikes! This so-called “physiological herniation” is normal development, however. Whew!
As the loop herniates, it also rotates about 90 degrees counterclockwise (as viewed from the anterior) around the axis of the superior mesenteric artery. The cranial limb of the loop thus moves caudally and to the embryo’s right side while the caudal limb moves cranially and to the embryo’s left side. At this time, we also note that the cranial limb begins to grow and expand to form the many loops and coils of the future jejunum and ileum.
During Week 10, the herniated midgut retracts from the umbilical cord and returns to the abdominal cavity, which has now grown large enough to accommodate the gut tube. As the twisted primary intestinal loop returns, it undergoes an additional 180 degree counter clockwise rotation. Now we see the original caudal limb of the primary intestinal loop (future large intestine) moving to the embryo’s right side, while the original cranial limb (future small intestine) moves to the embryo’s left.
For reference, keep an eye on the cecal primordium = that bump just distal to the apex of the original primary intestinal loop. Note how it moves to the right and into the lower quadrant of the abdomen after the midgut loop has retracted and rotated. That, of course, is the location of the definitive cecum and appendix in the adult. Hurray! How many total degrees has it rotated? The answer is = 270 degrees counter clockwise as viewed from thefront of the embryo. Do you see this?
Rotation of the primary intestinal loop and descent of the cecum to the lower right quadrant explains why the transverse colon is located superior to the loops of the small intestine and passes anterior to the duodenum, and why the large intestine forms a “box” around most of the jejunum and ileum. Cool, huh? Figure 22 shows the definitive orientation of the midgut following rotation.
Figure 22. LARSEN’ S HUMAN EMBRYOLOGY, FIG. 14.14.
Omphalocele is a congenital anomaly in which abdominal organs (surrounded by a bag made of serous membrane) are outside the body cavity, having been herniated through the ring of the umbilicus. This could be due to failure of the midgut loop to retract into the body cavity during rotation or subsequent herniation of organs later in development.
Omphaloceles can be large, including the entire bowel and liver. They are often associated with chromosomal abnormalities.
Clinical correlation
Malrotation describes any defect caused by abnormal rotation of the midgut or abnormal fixation of the midgut to the posterior body wall during rotation.
Figure 23. MOORE ET AL., THE DEVELOPING HUMAN, FIGURE 11-20.
Non-rotation means that the primary intestinal loop undergoes normal initial 90 degree rotation, but fails to undergo the remaining 180 degree counterclockwise rotation as it is retracted into the abdominal cavity.
Abnormal or incomplete rotation can pin the midgut to the body wall, causing coils of the small intestine to hang down and twist. This torsion could produce a volvulus, which can lead to obstruction of the intestine and/or compression of blood supply. If the arterial supply is cut off, intestinal ischemia can occur, and could result in a segment of necrotic bowel.This requires emergent operative intervention! Volvulus isalways a consideration in cases of malrotation!
In reversed rotation, the primary intestinal loop undergoes normal initial 90 degree rotation counterclockwise. However, the second 180 degree rotation occurs clockwise, so the net rotation of the midgut is 90 degrees clockwise. This brings the midgut and hindgut into normal spatial arrangement, except that the duodenum lies ventral to the transverse colon, instead of dorsal to it. The duodenum therefore does not become secondarily retroperitoneal, whereas the transverse colon does! Note that the superior mesenteric artery courses above the transverse colon, instead of the duodenum, as it normally does.
Development of the hindgut
The topographic orientation of the hindgut in the adult is mostly due to the development we described for the midgut = the growth, expansion, rotation, and displacement of the primary intestinal loop. This produces the box-shaped colon and puts the sigmoid colon into the lower left quadrant of the abdomen. Given this fact, we are not left with too much to discuss regarding hindgut development. For now, here is a quick rundown of the special development associated with the distal part of the hindgut that gives rise to the elements at the “tail end” of the digestive tube = the rectum and anal canal.
Figure 17.24. LANGMAN'S MEDICAL EMBRYOLOGY, FIGURE 15.36.
The part of the hindgut just superior to the cloacal membrane expands to form a pouch called the cloaca. This structure is the embryo’s “sewer” since it will develop into organs that store both urine and feces in the adult!
A diverticulum of the cloaca called the allantois extends into the umbilical cord. Normally the allantois regresses into a ligament-like band of connective tissue called the urachus, which has no function in humans but to connect the apex of the bladder to the anterior abdominal wall.
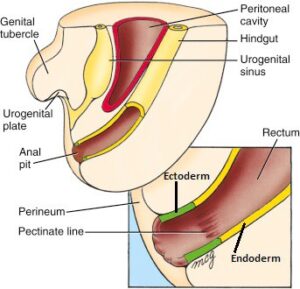
The cloaca is partitioned into a dorsal anorectal canal and a ventral urogenital sinus by the growth of a wall of mesoderm called the urorectal septum. The urogenital sinus will produce structures such as the urinary bladder and urethra. The anorectal canal gives rise to the rectum and anal canal. The development of urinary organs is discussed in another session.
Growth of the urorectal septum also partitions the cloacal membrane in half. The dorsal part closing the anorectal canal is the anal membrane.
Ectoderm around the anal membrane proliferates to form a raised circular border around the future anus. This process moves the anal membrane internally, so it is now placed at the bottom of a “pit”lined by ectoderm (called the proctodeum). As a result, external to the anal membrane is a short canal lined by ectoderm, while internal to the membrane is the distal end of the hindgut lined by endoderm.
Figure 25. LARSEN’S HUMAN EMBRYOLOGY, FIGURE 14-33.
The anal membrane breaks down during the 7th or 8th week. The location of the anal membrane is marked in the adult anal canal by a serrated fold of mucosa called the pectinate line. This is an important landmark and will be discussed in more detail with the perineum.
The proximal anal canal above the pectinate line is derived from the anorectal canal and is lined by epithelium derived from endoderm.
The distal anal canal below the pectinate line is derived from the proctodeum and is lined by epithelium derived from ectoderm.
The arterial supply, venous drainage, lymphatic drainage, and innervation of the two parts of the anal canal (as well as their sensitivities to touch and pain) are also different. So, get to know your pectinate line.
Clinical correlation
Failure of the anal membrane to break down properly can lead to a narrowed anal canal (anal stenosis) or an imperforate anus.
Failure of the urorectal septum to partition the cloaca correctly can cause abnormal communication between anal canal and urinary organs (fistulas).
Figure 26. MOORE ET AL., THE DEVELOPING HUMAN, FIGURE 11-29.
Summary: Fate of the dorsal mesentery
Secondarily retroperitoneal organs
Intraperitoneal organs
Rotational changes and movements of the developing gut cause some parts ofthe digestive tract to become fused to the posterior wall of the abdominal cavity, obliterating their dorsal mesentery. These organs are said to be secondarily peritoneal:
Second, third, and fourth parts of duodenum
Pancreas
Ascending and descending colon
Rectum
Thought question Why do some organs become secondarily retroperitoneal? No one knows for sure, but fixing some organs stoutly to the body wall may prevent excessive twisting and kinking in the gut tube as foodstuffs move through it during digestion.
Retain mesenteric attachments to the dorsal body wall.
Stomach
First part of duodenum
Jejunum and ileum
Appendix
Transversecolon
Sigmoid colon
Greater omentum
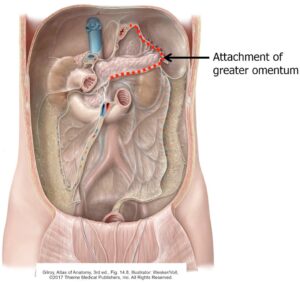
Figure 27.
The embryonic dorsal mesentery of the stomach becomes an adult structure called the greater omentum. The greater omentum has three major parts:
Gastrocolic ligament
Connects the proximal duodenum and greater curvature of the stomach to the posterior body wall = it drapes over the transverse colon like an apron or bib in doing so.
Gastrosplenic ligament
Between stomach and spleen.
Splenorenal ligament
Between spleen and posterior body wall, over the left kidney.
Stomach rotation stretches the dorsal mesentery anteriorly and to the left. Continued growth of the greater omentum after stomach rotation produces the redundant loop of mesentery that hangs down from the greater curvature of the stomach like a bib, an apron, or an empty pocket (take your pick of visual analogies!) = this part is technically the gastrocolic ligament. Rotation of the stomach also explains why the gastrocolic ligament has moved from an orientation in the sagittal plane in the embryo to a definitive orientation in a coronal plane. Remember also that rotation of the stomach forms the lesser sac of the peritoneal cavity behind the stomach and lesser omentum.
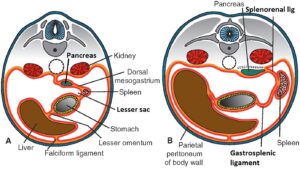
Figure 28. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 15.11.
The spleen develops from a lump of splanchnic mesoderm within the dorsal mesentery of the stomach during Week 5. The spleen is not a digestive organ, and it is not derived from endoderm. Instead, it is a vascular lymphoid organ derived from mesoderm. As the greater omentum forms and buckles to the left side of the body (see discussion earlier) it carries the spleen with it to the left. Formation of the spleen partitions the greater omentum that connects the fundus of the stomach to the posterior body wall into two parts: gastrosplenic ligament (fundus of stomach to spleen) and splenorenal ligament (spleen to posterior body wall—attaching anterior to the retroperitoneal left kidney). The spleen is thus an intraperitoneal organ. Note that the pancreas also develops within the dorsal mesentery of the stomach, but later becomes retroperitoneal.
Rotation of the stomach accomplishes a lot of things:
Turns the stomach on its side, such that it has anterior and posterior surfaces.
Aligns the stomach, lesser omentum, and gastrocolic ligament in the coronal plane.
Produces the lesser sac.
Kinks the duodenum into its C shape.
Moves the liver to the right side of the abdomen.
Causes the pancreas to become retroperitoneal, as the dorsal mesentery behind it collapses.
Mesentery (mesentery proper)
Figure 29. WIKIMEDIA COMMONS.
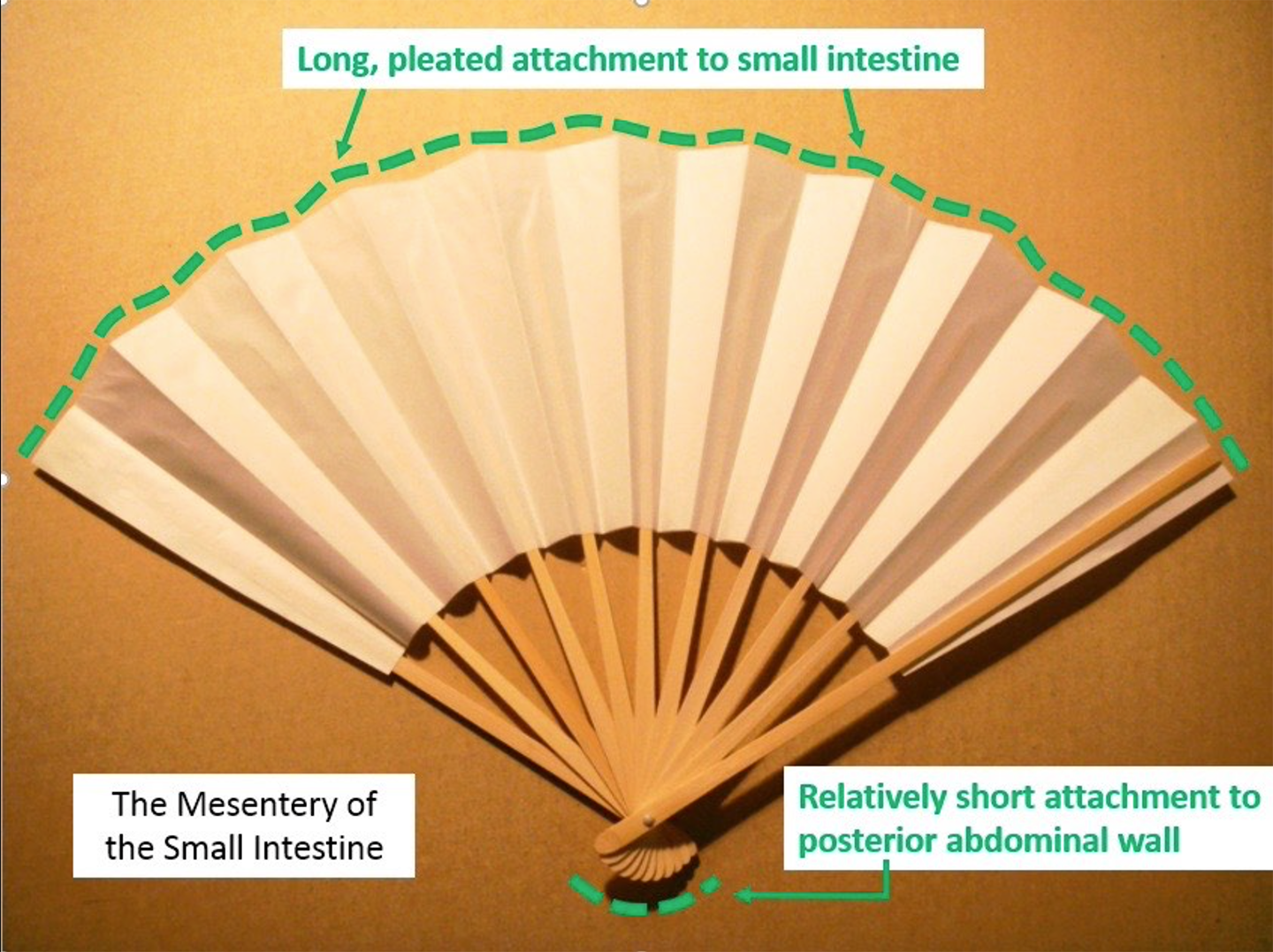
The dorsal mesentery of the jejunum and ileum is simply called the mesentery or the mesentery proper. Rotation of the midgut and movement of the cecum to the right lower quadrant explains why it attaches obliquely across the posterior abdominal wall and toward the right, from the distal duodenum to the cecum, and why it contains the superior mesenteric artery. Because the small intestine grows so rapidly in comparison to the body wall, it forms many loops, increasing the absorptive area internally. The attachment of the mesentery to the small intestine is therefore much larger in size than its attachment to the posterior abdominal wall—this causes the mesentery to be folded upon itself, like a hand fan, or the pleats in an accordion (for you accordion enthusiasts!).
Transverse mesocolon
Figure 30. LANGMAN’S MEDICAL EMBRYOLOGY, FIGURE 15.13.
The mesentery of the transverse colon is the transverse mesocolon. The complex movements and rotations of the stomach and midgut bring the dorsal mesenteries of the stomach and transverse colon in close proximity—this is why the superior surface of the transverse mesocolon is fused to the posterior fold (posterior side of the “empty pocket”) of the gastrocolic ligament in the adult. See Figure 30 to convince yourself of this.
Sigmoid mesocolon
The dorsal mesentery of the sigmoid colon is the sigmoid mesocolon. It attaches to the body wall in an inverted V fashion (which ancient anatomists believed looked like the Greek sigma Ʃ) along the leftiliac fossa and left side of the pelvic cavity.