The oral region includes the lips, cheeks, oral cavity (mouth), gingivae (gums), teeth, tongue, palate, and oral fauces (the area connecting the oral cavity to the pharynx). It is the gateway to the digestive tract. This region is often delegated to dental colleagues. However, there is a good deal of pathology that occurs here that is common to medicine and dentistry. This may be the only time that medical students focus on the anatomy of this specialized area that accounts for many patient complaints.
Functions of the oral region
The mastication apparatus (muscles, jaws, and teeth) breaks down ingested food. It is mixed with saliva in the oral cavity creating a pasty mass called a bolus.
Mechanical and chemical processes occurring in the mouth are the first stages of digestion. The oral region is also important in producing speech and facial expressions.
Lips and cheeks
Figure 35.1.
Lips
Cheeks
The lips contain the orbicularis oris muscle and the superior and inferior labial arteries. The muscle acts as a sphincter regulating the size and shape of the space between the lips, the oral fissure. The portion of the lips where transition occurs between face and oral cavity has a dark appearance due to its thin skin and many underlying capillaries.This is the vermillion border, often erroneously referred to as the lips themselves. The extent of the lips is actually much greater, spanning from nostrils to chin. This can easily be demonstrated by sliding your tongue behind the upper and lower lips in the midline of your mouth. Here the lips are tethered to the upper and lower gums by folds of mucosa called labial frenula. Check these out in the mirror!
The cheeks form the lateral borders of the oral cavity. They are covered externally by skin and internally by a mucous membrane. Between these layers are the buccal fat pad and the buccinator muscle. Although a muscle of facial expression, the functions of the buccinator are critical to mastication (discussed earlier).
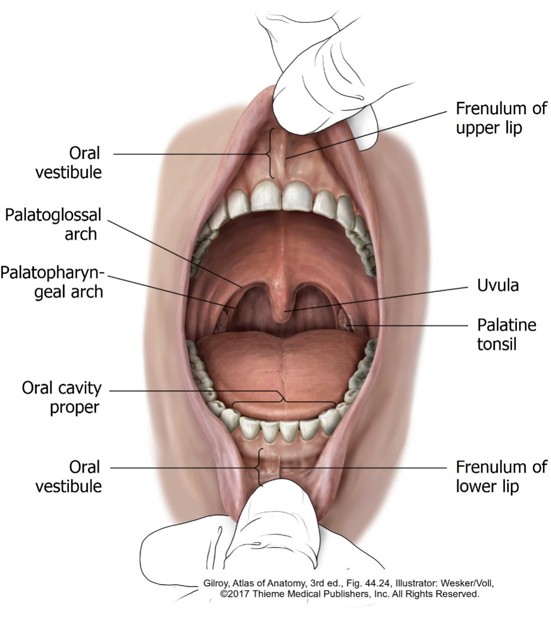
Oral cavity
Two parts = oral vestibule and oral cavity proper. These are separated by the teeth and gums.
Oral vestibule
The oral vestibule is the narrow space between teeth and lips and teeth and cheeks. Within the vestibule is an upper and lower labial frenulum (described earlier). The parotid ducts open in the vestibule opposite the second upper molar teeth.
Oral cavity proper
The oral cavity proper is internal to the teeth and gums. It extends from the palate above to the floor of the mouth below the tongue. The mobile part of the tongue protrudes into the oral cavity proper. Posteriorly the oral cavity proper communicates with the pharynx via the oral fauces.
Clinical correlation
The oral cavity is a window to the body's health. Pathologic changes to the mouth can be an indicator of systemic disease. Body-wide infections, nutritional disorders, and organ disease (e.g., HIV, vitamin deficiencies, Addison's disease) may later manifest as oral conditions.
Likewise, diseases that begin in the oral cavity may later involve distant organs, such as the link between periodontal disease and cardiovascular disease.
Gingivae and teeth
Why do physicians need to know about the teeth and gums, you ask? Emergency Departments see dental problems after hours and on weekends, which is reason enough!
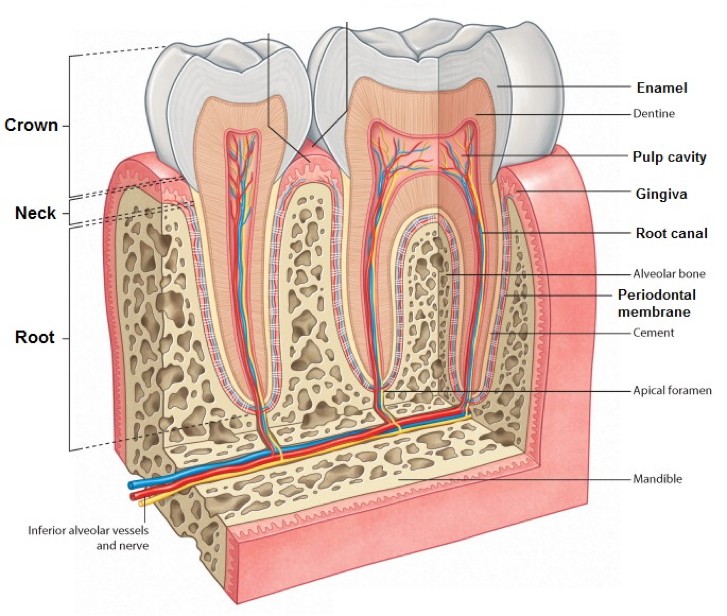
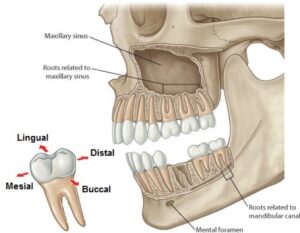
Figure 35.2. Anatomy of teeth. GRAY’S ATLAS OF ANATOMY, 2ND ED.
Here’s “Tooth Anatomy 101.”
The teeth are attached to “tooth sockets” (alveoli) by dense connective tissue called periodontal ligaments. The tooth sockets are located in the alveolar processes of the maxillae and mandible. The gums (gingivae) are layers of connective tissue and mucous membrane covering the alveolar processes. They are continuous with the periodontal ligaments in the tooth sockets.
A tooth has a crown and a root.
The crown is the part visible above the gingiva and is covered by enamel, a super-hard mineralized layer with no living cells. The top of the crown has ridges called cusps.
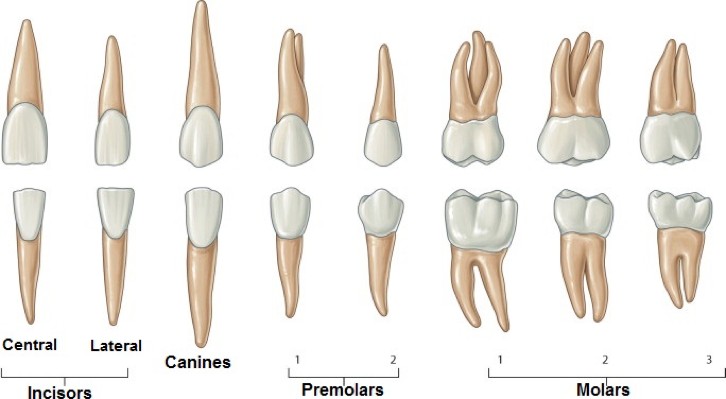
The root is fixed in the tooth socket by the periodontal membrane. Some teeth have more than one root—the upper molar, teeth for example, have three.
The roots, being embedded in bone, are examined with X-rays.
Each tooth contains a cavity that is filled with dental pulp (loose connective tissue, nerves, and blood vessels). The pulp cavity extends into the root(s) of the tooth—forming the root canal(s).
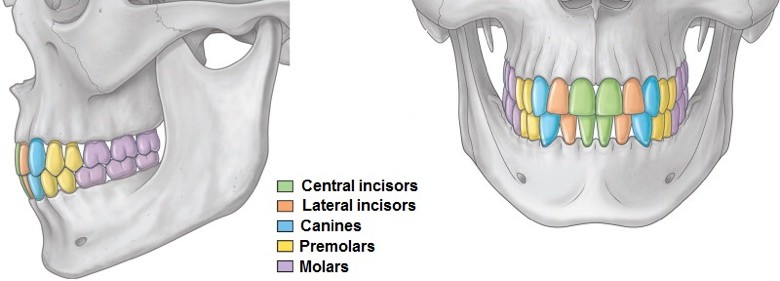
The upper and lower teeth are arranged in curved dental arches.
Primary teeth or deciduous teeth (so named because they fall out, like leaves from a tree) erupt from the gums between 6 months and 3 years of age. There are 20 primary teeth.
Figure 35.4. Adult upper and lower permanent teeth. GRAY’S ATLAS OF ANATOMY, 2ND ED.
Primary teeth are replaced by permanent teeth. These appear at various times during childhood and early adulthood. Adults with full dentition have 32 permanent teeth. Each quadrant of a dental arch as 2 incisors, 1 canine, 2 premolars, and 3 molars (8 teeth). The third (most distal) molar is called a “wisdom tooth,” presumably because it erupts last, when we are older and wiser! Dentists use a numbering system to uniquely identify each tooth in both dental arches.
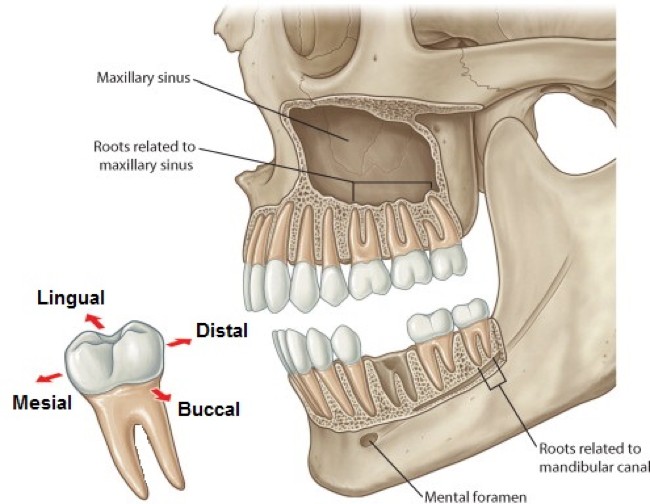
Figure 35.5. Adult permanent teeth with roots exposed, first molar extracted. GRAY’S ATLAS OF ANATOMY, 2ND ED.
Each tooth has five named surfaces:
Occlusal: Faces up or down (depending on whether the tooth is in the maxillae or mandible) and contacts the corresponding tooth above or below it. It has cusps.
Mesial: Faces toward the midline of the dental arch.
Distal: Faces away from the midline of the dental arch.
Buccal/labial (also called vestibular): Faces outward, toward the cheeks or lips
Lingual: Faces inward, toward the tongue
Clinical correlation
The alveoli of the maxillary molar teeth extend up into the nearby maxillary air sinus, forming ridges in the floor of the sinus. The roots of the molars are thus adjacent to the sinus mucosa. Tooth extraction could perforate the tooth socket, creating an opening to the sinus. Because of their proximity and overlapping nerve supply, tooth pain can be perceived as sinus pain the central face, and pain from an infected sinus could be perceived as a toothache.
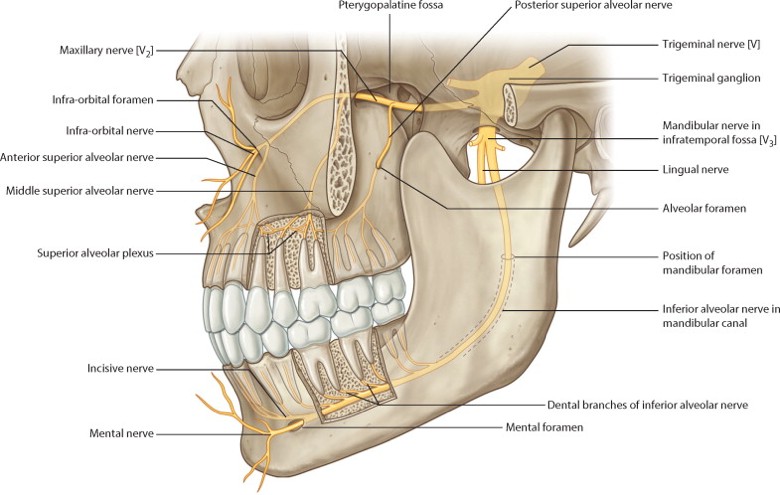
Figure 35.6. Innervation of the teeth. GRAY’S ATLAS OF ANATOMY, 2ND ED.
The upper teeth are innervated by the superior alveolar nerves (posterior, middle, and anterior), which are branches of V2. The lower teeth are supplied by inferior alveolar nerves from V3, which traverse the mandible in the mandibular canals.
Tongue
The tongue is a mobile muscular organ that can assume a variety of shapes and positions in order to fulfill its roles in chewing, taste, swallowing, and speech.
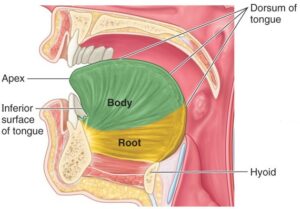
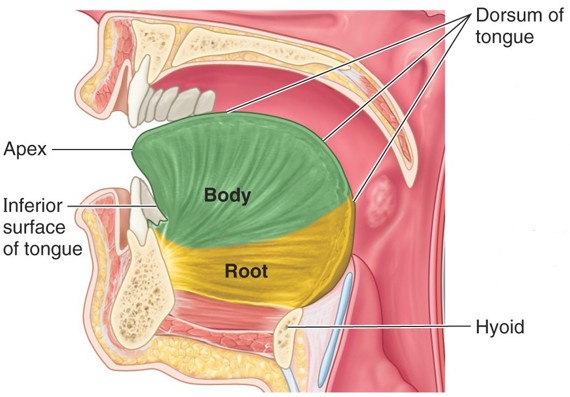
Figure 35.7. Parts of the tongue. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 7.88.Root: The fixed part of the tongue; attached to the mandible, hyoid bone, and epiglottis.
Apex (tip): The tapered anterior end that touches the incisor teeth.
Body: Central portion between root and apex. The body and apex are highly mobile.
Dorsum: Large surface area, it is sharply curved and faces up towards the palate and posterior towards the pharynx.
Inferior surface: Short, faces down toward the floor of the mouth.
Features on the dorsum
Figure 35.8. Dorsal surface of tongue. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 7.88.
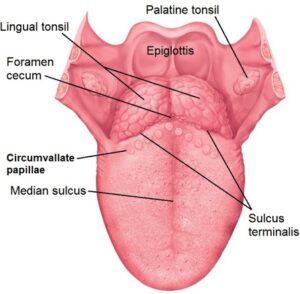
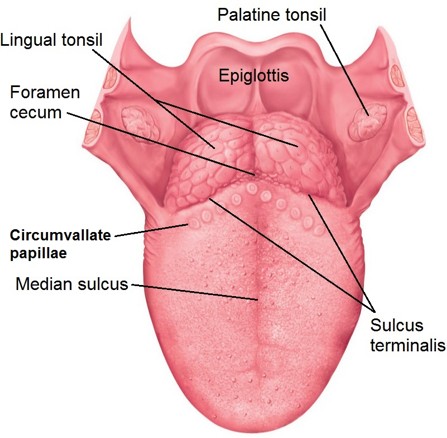
The median sulcus separates the anterior tongue into right and left portions. Deep to the sulcus, a median septum separates the two sides of the tongue. Most blood vessels don’t cross the septum. Tongue piercings are placed in the septum to avoid heavy bleeding.
The V-shaped sulcus terminalis separates the body and root of the tongue and is a useful landmark for describing the development and innervation of the tongue = 2/3 of the tongue is anterior to the sulcus terminalis, 1/3 is behind it.
At the apex of the “V” is the foramen cecum. This pit indicates the site where the primordium of the thyroid gland descended from the embryonic pharynx to its definitive location in the neck. An undescended thyroid gland presenting as a lump of tissue at the formen cecum is called a lingual thyroid.
The lingual tonsil covers the dorsum of the tongue behind the sulcus terminalis. It resembles a cobblestone street and contains lymphoid tissue.
Papillae (Latin = nipples) are found on the dorsum and sides of the anterior 2/3 of the tongue.
Filiform papillae are sharp and abundant. Like sandpaper, they give texture to the tongue, allowing it to grip food and position it on the teeth for chewing. Cats have awesome filiform papillae on their tongues!
Fungiformpapillae are scattered and shaped like mushroom caps. They contain taste buds. Taste sensations from these papillae travel in cranial nerve VII.
8–12 large circumvallate papillae are arranged in a “V” just anterior to the sulcus terminalis. They have a large mushroom cap in the center, surrounded by a round moat. They contain taste buds. Their taste information is transmitted in cranial nerve IX.
On the inferior surface/floor of the mouth
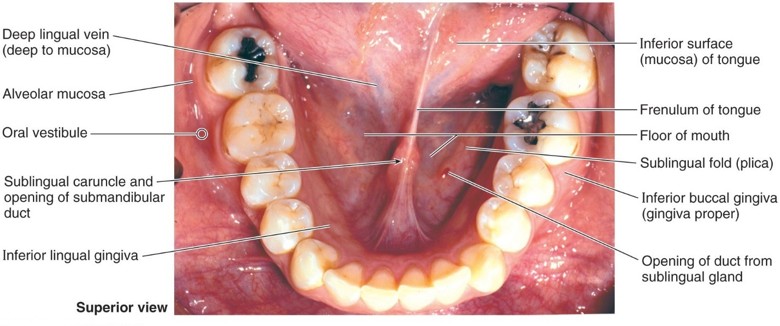
Figure 35.9. Inferior surface of tongue and floor of mouth. CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 7.89.
The frenulum of the tongue is a midline mucosal fold connecting the tongue to the floor of the mouth. Along the margins of the frenulum near its base are the sublingual caruncles, small elevations that contain the orifices of the submandibular ducts (described later). Lateral to the frenulum are bilateral ridges of mucosa called sublingual folds, raised over the underlying sublingual salivary glands. Take a look under your tongue in the mirror—these structures are easy to identify.
Clinical correlation If the frenulum extends too far forward on the interior surface of the tongue, it can affect breastfeeding and speech. This congenital condition is called ankyloglossia (tongue tie). If the condition causes problems, a surgical incision can release the tongue.
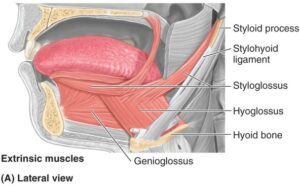
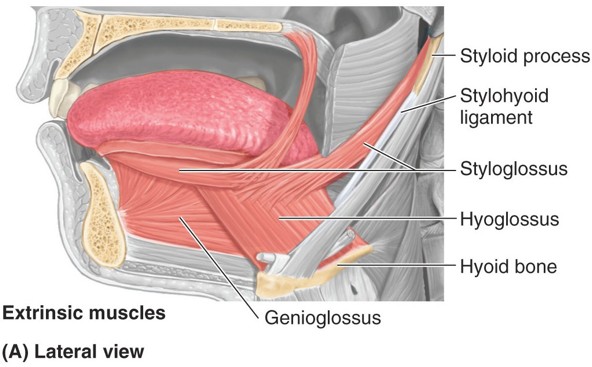
Figure 35.10. Extrinsic muscles of the tongue. CLINICALLY ORIENTED ANATOMY, FIGURE 7.90.Extrinsic tongue muscles have bony attachments outside the tongue. There are 4 paired extrinsic muscles and their names describe their attachments (glosso = Greek, tongue).
Origin
Insertion
Action
Genioglossus (genio = Greek, chin)
Inside of the mandible, opposite the chin
Fibers are arranged like a fan—insert into the body of the tongue
Protrudes tongue from mouth; pulls tongue down (depression)
Hyoglossus
Hyoid bone
Lateral part of the body of the tongue
Depresses tongue and retracts it
Styloglossus
Styloid process
Lateral part of the body of the tongue
Retracts tongue
Palatoglossus (Note: This muscle acts more on the palate than it does the tongue. It is innervated by CN X.)
Soft palate
Posterior body of tongue
Elevates tongue or depresses palate
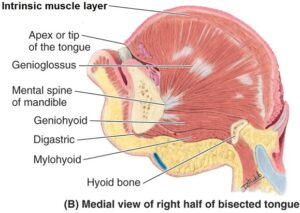
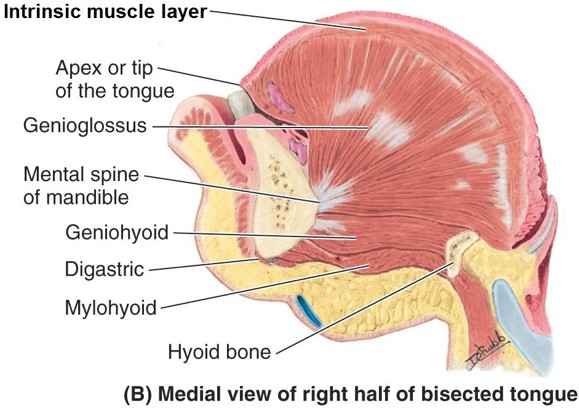
Figure 35.11. Muscles of the tongue, median section. CLINICALLY ORIENTED ANATOMY, FIGURE 7.90.Intrinsic tongue muscles have attachments completely within the tongue itself. These are arranged in layers with different patterns of organization in their fibers. In general, these alter the shape of the tongue (widen, shorten, flatten, curl) and can raise or lower (“flick”) the tip of the tongue independently.
Motor: All muscles of the tongue (extrinsic and intrinsic) aresupplied by the hypoglossal nerve (CN XII), EXCEPT one. Palatoglossus is the exception, being innervated by CN X.
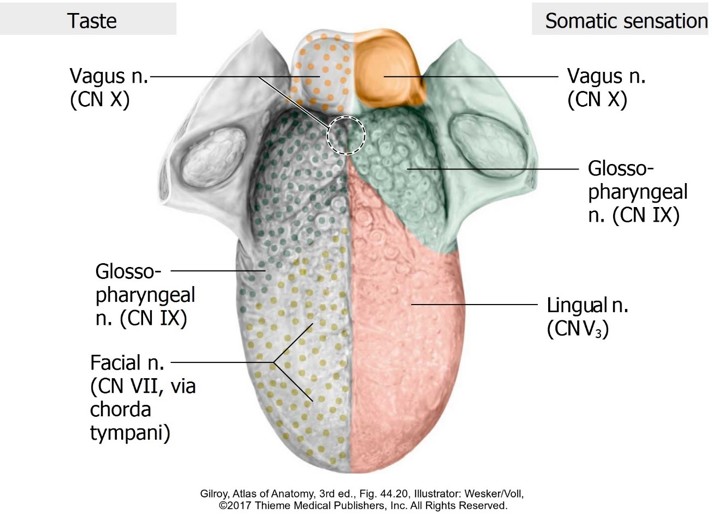
Sensory: Best described by considering the tongue in 3 parts: anterior 2/3, posterior 1/3, and root of tongue where it attaches to the epiglottis. See the table below for a summary.
Note: general sensation (touch, pressure, pain, temperature) is different from the special sensation of taste.
Cranial nerve (or branch)
Anterior 2/3 of tongue
Posterior 1/3 of tongue
Root of tongue near epiglottis
Muscles
Lingual (V3)
General sensation
Chordatympani (VII)
Taste
Glossopharyngeal(IX)
General sensation and taste
Vagus (X)
General sensation; taste buds on epiglottis
Palatoglossus
Hypoglossal (XII)
All intrinsic and extrinsic muscles except palatoglossus
Clinical correlation Having a patient protrude their tongue is a test of the function of the hypoglossal nerve. If cranial nerve XII is damaged unilaterally, the tongue will deviate toward the weakened side (side of the lesion) when protruded.
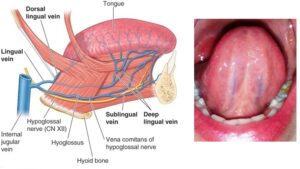
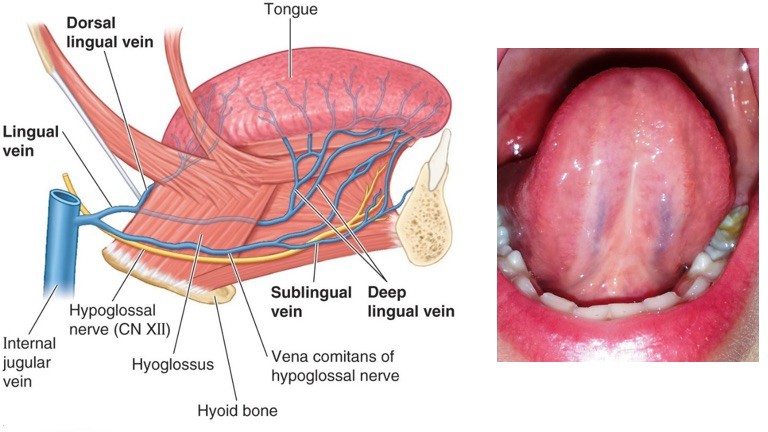
Figure 35.13. Deep lingual veins. CLINICALLY ORIENTED ANATOMY, FIGURE 7.93.Blood supply: Lingual artery, a branch of the external carotid in the neck.
Venous drainage: Dorsal and deep lingual veins. These usually merge to form a single lingual vein.
Clinical correlation Deep lingual veins are on the inferior surface of the tongue. They are easily seen since only a thin layer of mucosa separates them from the oral cavity. This is clinically useful: Sublingual administration of drugs is done by placing the medication under the tongue, where it dissolves and rapidly enters the blood stream by diffusing into the deep lingual veins. Nitroglycerine and Zofran are examples of drugs administered sublingually so they can act quickly.
Clinical correlation: Words of advice from an ENT Doc The entire tongue cannot be examined by visually inspecting the mouth. Realize that the posterior one-third of the tongue faces backward, toward the pharynx. To see it requires the use of a mirror or scope. Tumors of the tongue can be missed without this knowledge. Risk factors for tongue cancers include tobacco use and human papilloma virus (HPV) infection.
Complex and somewhat unpredictable since it does not always follow the blood vessels. Lymph from the central tongue passes directly to deep cervical nodes in the neck. Lymph from the sides of the tongue goes first to submandibular nodes. Lymph from the apex passes first to submental nodes. Ultimately all lymph from the tongue does reach the deep cervical lymph nodes.
Development of the tongue
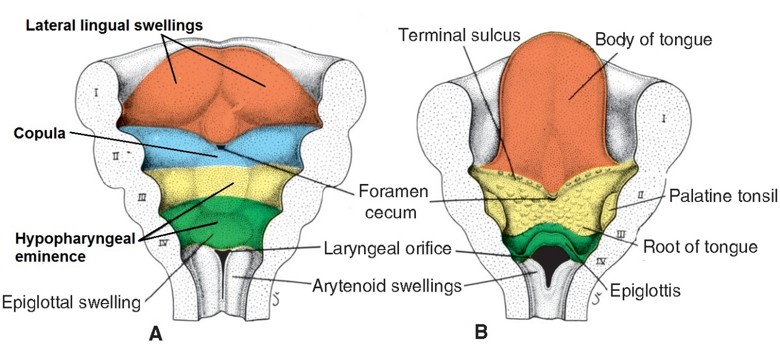
Figure 35.14. Development of the tongue. LANGMAN’S MEDICAL EMBRYOLOGY, 12TH ED., FIGURE 17.17.
The tongue develops in the floor of the primitive pharynx from four embryonic primordial masses derived from the first four pharyngeal arches. This explains the innervation pattern of the tongue.
The anterior 2/3 of the tongue develops from paired lateral lingual swellings, containing mesenchyme from the first pharyngeal arches. They merge in the midline at the median septum. The lingual branch of the mandibular nerve (V3) supplies the lateral lingual swellings.
A central mass of mesenchyme (the copula) from the second pharyngeal arches grows caudal to the lateral lingual swellings. It is a temporary structure. The chorda tympani branch of the facial nerve supplies the copula.
Although the copula contributes nothing to the definitive mucosa of the tongue, chorda tympani nerve fibers do persist and innervate taste buds in the anterior 2/3 of the tongue.
Mesenchyme contributed by the third and fourth pharyngeal arches forms the hypopharyngeal eminence. This overgrows the copula and fuses with the lateral lingual swellings at the sulcus terminalis. The eminence forms the posterior 1/3 of the tongue and the tissues of the epiglottic region. The glossopharyngeal and vagus nerves innervate the hypopharyngeal eminence.
The muscles of the tongue are derived from paraxial mesoderm that migrates into the tongue at the base of the head. Nerve fibers from the hypoglossal nerve associate with the mesoderm before it migrates.
Salivary glands
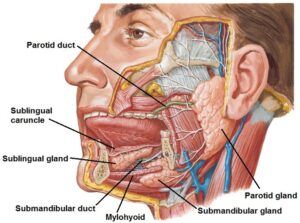
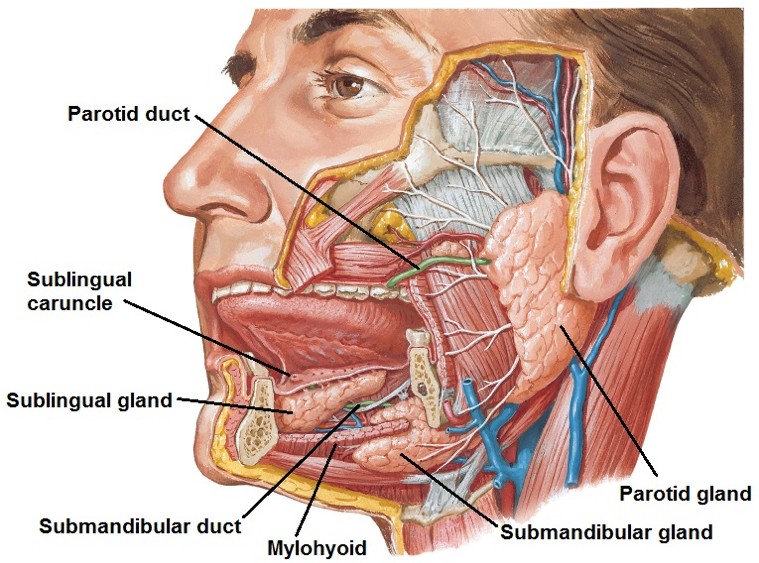
Figure 35.15. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 46.
Salivary glands produce and secrete saliva, a viscous fluid that moistens and lubricates the food bolus, contains amylase, which initiates digestion of starches, flushes the mouth to keep it clean, and contains antimicrobial agents to protect the teeth from bacteria.
Parasympathetic innervation stimulates salivary glands to secrete saliva. Sympathetic innervation inhibits them, producing a dry mouth when frightened or fearful.
Minor salivary glands are small and scattered in the mucosa of the lips, cheeks, palate, and tongue. They secrete saliva into the oral cavity continuously to keep it moist.
Major salivary glands, three in number, are paired and produce saliva when food is present or anticipated. They are connected to the oral cavity via ducts.
Parotid gland: The largest of the salivary glands, it is located subcutaneously on the lateral face and was discussed previously. The parotid duct (Stensen’s duct) penetrates the buccinator muscle to empty in the oral vestibule opposite the upper second molar teeth. The parotid gland is innervated by the glossopharyngeal nerve. The pathway is summarized by the flow chart below.
Glossopharyngeal nerve pathway
Pre-G Neurons:
Inferior salivatory nucleus (brainstem)
CN IX
Tympanic branch of CN IX
[Tympanic cavity]
Lesser petrosal nerve
[Middle cranial fossa]
[Foramen ovale]
Otic ganglion
[POST-G neurons]: Secretomotor fibers join the auriculotemporal nerve of V3
Parotid gland
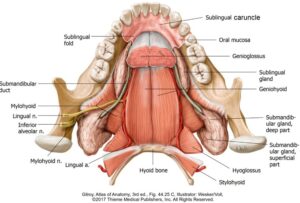
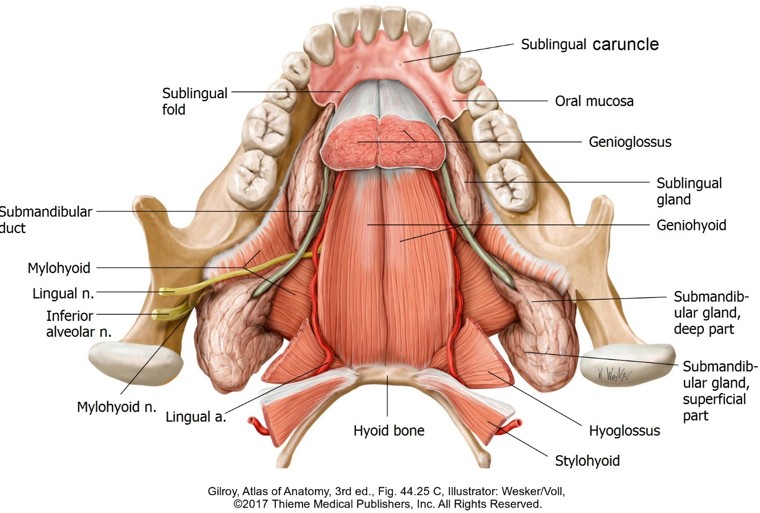
Figure 35.16. Course of submandibular duct in the floor of the mouth, superior view. The tongue has been removed. The duct is sandwiched between the tongue and sublingual gland and is crossed by the lingual nerve.Submandibular gland: Located inferior to the mandible, it curls around the posterior free margin of the mylohyoid muscle. The superficial part of the gland is external to the mylohyoid while the deep part is above it. The submandibular duct (Wharton’s duct), about 2 inches long, leaves the deep part of the gland above the mylohyoid and squeezes between the sublingual gland and genioglossus muscle to reach the floor of the mouth. As it does so, it spirals around the lingual nerve (V3), crossing it twice. Wharton’s duct opens on the sublingual caruncle below the tongue.
Sublingual gland: Smallest of the major salivary glands, it is long from front to back and has a thin profile side-to-side since it is lodged between the mandible and genioglossus muscle, below the floor of the mouth. The glands create the sublingual folds just lateral to the lingual frenulum in the floor of the mouth. There are numerous sublingual ducts: some join Wharton’s duct, but most open directly into the floor of the mouth atop the sublingual folds.
The submandibular and sublingual glands are innervated by the facial nerve. The pathway is summarized below.
Facial nerve pathway
Pre-G Neurons:
Superior salivatory nucleus (brainstem)
CN VII
[Facial canal]
Chorda tympani nerve
[Tympanic cavity]
[Petrotympanic fissure]
Joins lingual nerve (V3) in the infratemporal fossa
Submandibular ganglion (attached to the lingual nerve)
[POST-G neurons]: Secretomoto fibers pass directly to the SUBMANDIBULAR GLAND or rejoin the lingual nerve to reach the SUBLINGUAL GLAND
Clinical correlation
Mumps is a contagious disease caused by a virus. It affects the parotid gland, causing it to swell. The dense capsule of the parotid gland limits swelling, evoking pain. Swelling of the gland also makes it difficult and painful to open the mouth since the gland is wedged behind the mandible.
Clinical correlation
Sialoliths are calcified masses or stones that form in salivary ducts. They are the most common disease of salivary glands, with the majority of them occurring in the submandibular ducts, probably because the saliva produced by the submandibular gland has the highest viscosity. They are managed conservatively or removed surgically by incision and drainage.
Surgeons need to be aware of the relationship between Wharton’s duct and the lingual nerve in order to avoid injury. What would be the symptoms in a patient with a damaged lingual nerve near Wharton’s duct?
Palate
Figure 35.17.
The palate forms the roof of the oral cavity and separates it from the nasal cavities and nasopharynx above. It is composed of the hard palate (anterior two-thirds) and soft palate (posterior one-third).
Hard palate
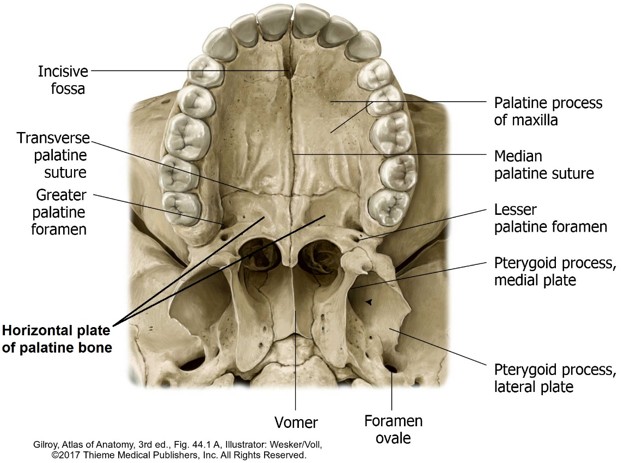
Has a bony skeleton formed by the palatine processes of the maxillae and the horizontal plates of the palatine bones.
The incisive fossa is a small cavity in the midline, just posterior to the central incisors.
Just medial to the 3rd molars the greater palatine foramina open on the palate and just posterior to these are the small lesser palatine foramina.
The bones of the hard palate are covered by a dense mucosa with many mucous glands that adheres firmly to the bone, with little loose connective tissue present. Because of this, injections to anesthetize the palate in preparation for dental procedures are painful! The palate has these surface features visible in the mouth:
Transverse palatine folds (rugae) are ridges in the anterior part of the palate, just behind the incisors. These behave like the filiform papillae to provide traction so that the slippery bolus of food can be manipulated by the tongue.
The palatine raphé is a faint ridge down the midline of the palate. It indicates the site of fusion of the palatine primordia during development.
Soft palate
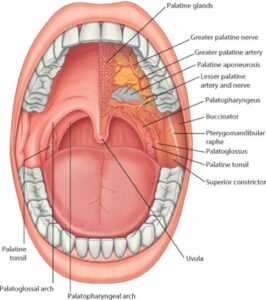
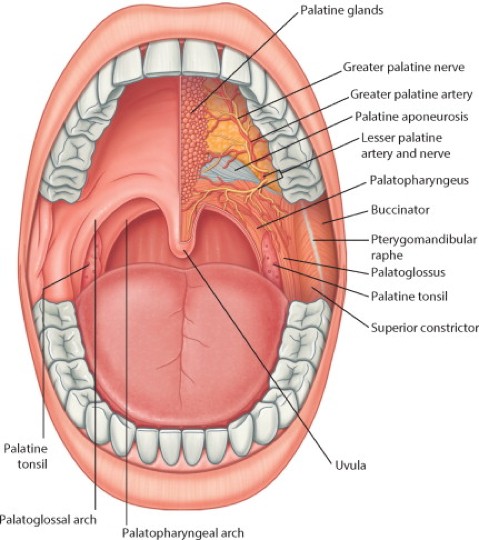
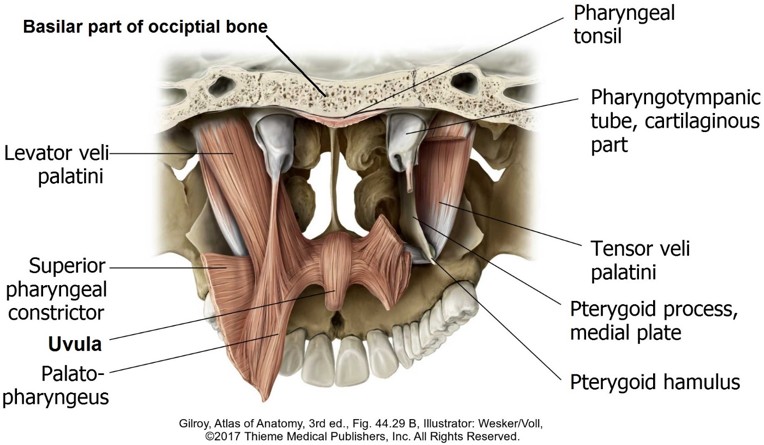
Figure 35.18. Roof of oral cavity. GRAY’S ATLAS OF ANATOMY, 2ND ED.The soft palate is muscular and mobile with no skeletal framework. It is reinforced by a core of dense connective tissue called the palatine aponeurosis.
The soft palate elevates to form a seal that blocks the nasopharynx, preventing food and liquid from entering the nasal cavities during swallowing. The most posterior part of the soft palate dangles in the midline. This is the uvula (Latin = grape). It may be important in preventing eversion of the soft palate during swallowing, speech production, and in eliciting a gag reflex to prevent large objects from entering the pharynx.
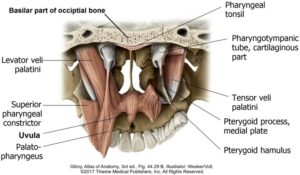
Attachments: Arises above from the sphenoid bone and cartilage of the pharyngotympanic (Eustachian) tube; inserts below into the palatine aponeurosis, in a horizontal direction.
Actions: Tenses the soft palate by stretching the palatine aponeurosis laterally. In order to do this, the tendon of TVP loops around the hamulus of the sphenoid bone, using it as a pulley to change the direction of pull from vertical to horizontal. When swallowing or yawning, the TVP pulls open the normally collapsed Eustachian tube, allowing air to enter it and reach the tympanic cavity. This sudden pressure equalization produces an “ear popping” sensation.
Innervation: Mandibular division of trigeminal (V3)
Figure 35.19. Muscles of the soft palate, posterior view. Levator veli palatini has been removed on the right to show the tensor veli palatini tendon looping around the pterygoid hamulus.Levator veli palatini (LVP)
Attachments: Arises above from the petrous temporal bone and cartilage of pharyngotympanic tube; inserts below into the palatine aponeurosis, in a vertical direction.
Action: Elevates soft palate.
Innervation: Vagus nerve
Palatoglossus
Attachments: Arises from the palatine aponeurosis; inserts into the side of the tongue.
Action: Approximates tongue and palate—this narrows the oral fauces after food has passed through it into the pharynx, to prevent regurgitation.
Innervation: Vagus
Palatopharyngeus
Attachments: Arises from palatine aponeurosis; inserts into the wall of the pharynx.
Action: Pulls pharynx superiorly when a bolus of food has entered it during swallowing.
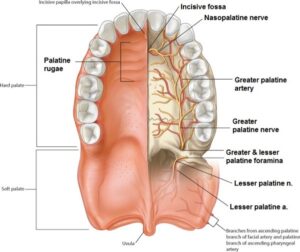
Nasopalatine nerve: Reaches the palate from the nasal cavity via the incisive canal and fossa. It supplies the mucosa directly behind the upper incisor teeth.
Greater and lesser palatine nerves: Supply the hard palate and soft palate, respectively. They reach the palate from the pterygopalatine fossa via the palatine canal. The palatine canal splits below to open on the palate via two openings = greater and lesser palatine foramina.
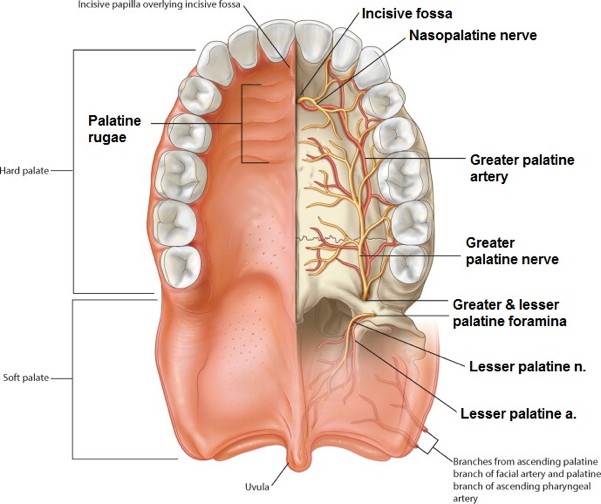
Figure 35.20. Palatine arteries and nerves. GRAY’S ATLAS OF ANATOMY, 2ND ED.
The descending palatine artery arises from the maxillary artery in the pterygopalatine fossa. It reaches the palate via the palatine canal, splitting below into greater and lesser palatine arteries that supply the hard and soft palates, respectively.
Clinical correlation
Many functions of cranial nerve X (Vagus) are difficult to observe directly. Its function in the head can be tested by having the patient open their mouth and say, "Ahh." The soft palate should rise symmetrically. If it moves to one side, the other side may be weak, suggesting a possible lesion of CN X.
Development of the palate
Figure 35.21. LANGMAN’S MEDICAL EMBRYOLOGY, 12TH ED., FIGURES 17.25, 17.26, AND 17.24.
The palate develops from the fusion of two primordia: primary and secondary palates.
Primary palate
The primary palate forms the portion of the hard palate anterior to the incisive fossa, as well as the upper incisors and their gums. The primary palate is the posterior part of the intermaxillary segment, which developed from the fused medial nasal prominences (subparts of the frontonasal prominence = discussed with the development of the face).
Secondary palate
The secondary palate gives rise to the hard palate posterior to the incisive fossa and to the soft palate. It is formed from two palatal shelves, mesenchymal projections that grow medially from the maxillary prominences. The palatal shelves fuse:
with each other in the midline behind the incisive fossa, and
to the primary palate.
Their anterior part ossifies, the posterior part does not. The palatine raphé indicates the line of fusion of the palatine shelves.
Clinical correlation
Cleft palate is fairly common, occurring in 1/2500 births and more often in females (67%). (Compare this to cleft lip: occurring in 1/1000 births, and 80% affected are males.) They occur posterior to the incisive fossa, when the left and right palatal shelves fail to fuse.
Cleft palate can impair feeding and speech. It can also be associated with other congenital anomalies and maternal use of anticonvulsant medications. A variant of palatal clefting with little or no consequences is bifid uvula.
Clefts of the soft palate disable the function of the tensor veli palatini muscles on the palate, preventing them from tensing it. Without a tense stable platform below, the tensor veli palatini can’t tug down on the pharyngotympanic tube to open it, so the tympanic cavity doesn’t get properly aerated. This may explain why children with complete cleft palates are more likely to get middle ear infections.
Oral fauces
Figure 35.22.
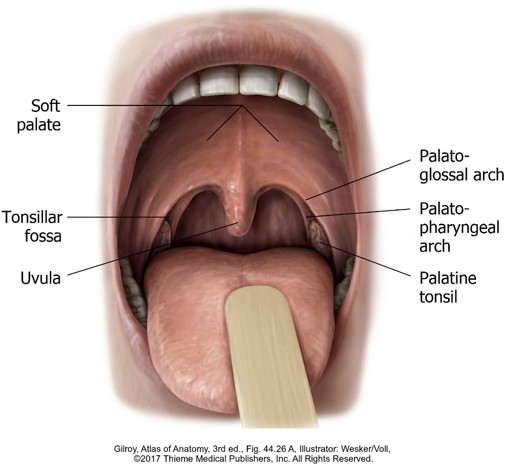
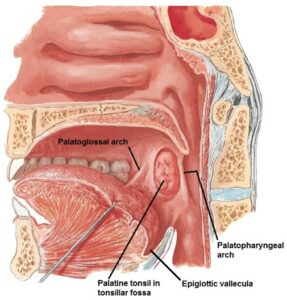
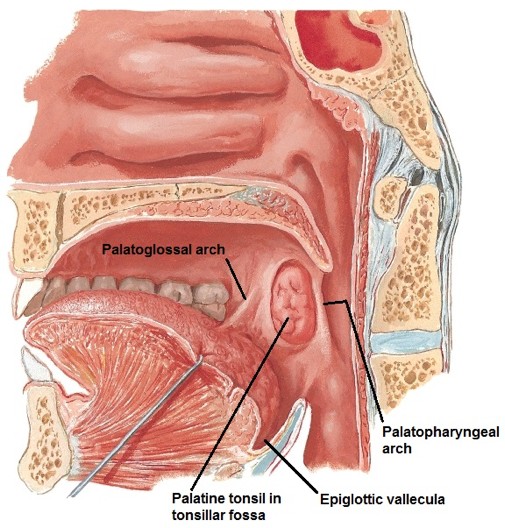
The fauces (Latin = throat) is the area that links the oral cavity and pharynx, where the bolus of food passes when swallowing. Many sources include it as part of the pharynx, so it is a bit in “no-man’s land.” We will consider it as an extension of the oral cavity. It is bounded superiorly by the soft palate, inferiorly by the root of the tongue, and laterally by the tonsillar fossa, palatine tonsils, and the arches (pillars) of the fauces.
Tonsillar fossa
Figure 35.23. NETTER, ATLAS OF HUMAN ANATOMY, 6TH ED., PLATE 68.
Two vertical mucosal folds are present on each side of the fauces. The anterior fold is the palatoglossal arch, curving downward from the soft palate to the tongue. The posterior fold is the palatopharyngeal arch, extending down from the soft palate to blend with the lateral wall of the pharynx. Each arch contains a similarly named muscle: the palatoglossusand palatopharyngeus muscles. The arches are commonly referred to as the “pillars of the fauces” or “tonsillar pillars.”
Between the two arches is the tonsillar fossa (also called the tonsillar sinus), a remnant of the embryonic second pharyngeal pouch. It is filled with the palatine tonsil, a structure that varies considerably in size and shape—it atrophies with age. Deep to the tonsillar fossa is the superior constrictor muscle. The surface of the tonsil is covered by an epithelium dotted with tiny pits called tonsillar crypts.
The tonsils receive a rich blood supply, mainly through the tonsillar branch of the facial artery. These vessels can bleed during tonsillectomy.
Below the tonsillar fossa, the root of the tongue connects to the epiglottis via three folds of mucosa. Between these folds are pouches called epiglottic valleculae. These are important landmarks for placing a laryngoscope during an intubation procedure. Once inserted properly, the laryngoscope depresses the tongue and epiglottis, so the airway and vocal cords and be viewed through the laryngeal inlet.
Clinical correlation
Deep to the tonsillar fossa is loose connective tissue known as the peritonsillar space. If an infection of the tonsil (tonsillitis) spreads to this potential space and progresses, it can form a peritonsillar abscess. These are most common in persons ages 20–40.
They are filled with pus and cause pain; difficulty swallowing (dysphagia); and a muffled, “hot potato” voice. Large abscesses can deviate the tonsil across the midline, obstructing the airway. Treatment consists of drainage (via incision or needle aspiration) and antibiotics.
The pharynx
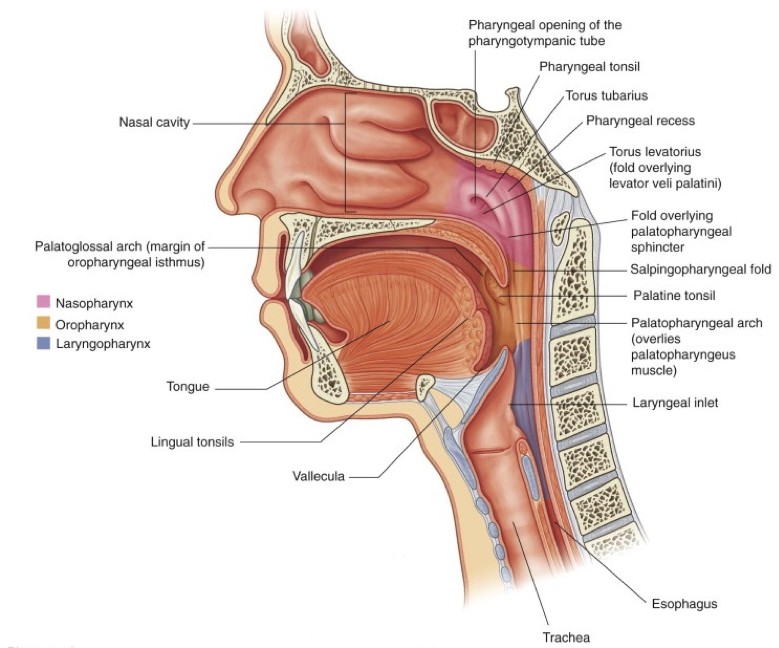
The pharynx (“throat”) is a muscular tube located against the skull base and vertebral column, posterior to the nasal and oral cavities. It is shared by the digestive and respiratory tracts, conveying both ingested food and air. It communicates below with the larynx and ends inferiorly at C-6 vertebra where it is continuous with the esophagus. The pharynx is closed posteriorly; anteriorly the open to the nasal cavities, oral cavity, and larynx.
Three divisions of the pharynx
Figure 35.24. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.201.
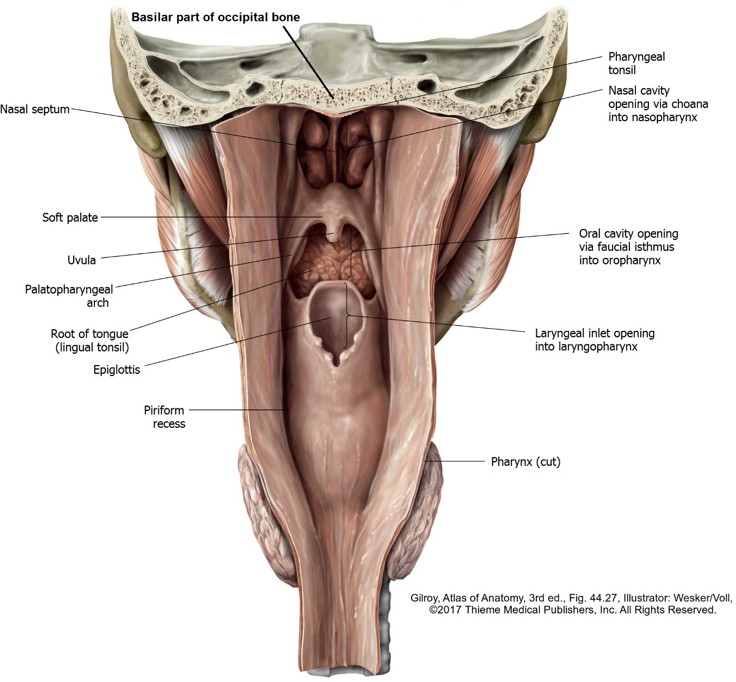
Figure 35.25. Posterior view of pharyngeal cavity. Posterior wall of pharynx has been open by a midline incision.
Communicates anteriorly with the nasal cavities via openings called choanae. Its curved roof and posterior wall contain the sphenoid and occipital bones. The soft palate forms the floor. Behind the soft palate the nasopharynx communicates below with the oropharynx. It communicates with the tympanic cavities via the pharyngotympanic (Eustachian) tubes.
Internal features of the nasopharynx
Pharyngeal tonsil: Lymphoid tissue in the roof of the nasopharynx. An enlarged pharyngeal tonsil (referred to as adenoids) can obstruct air flow and cause difficulty in nose breathing.
The orifice of the pharyngotympanic (Eustachian) tube is in the lateral wall. Because the tube passes downward and medially from the tympanic cavity, it enters the nasopharynx at an angle (not flush), producing a curved-ridge above the opening called the torus tubarius. In the mucosa of the torus is a mass of lymphoid tissue called the tubal tonsil. The tube is normally closed. To aerate the tympanic cavity and equalize pressure, the tube is briefly opened by muscles that contract when you swallow or yawn (muscles in the soft palate and pharyngeal wall).
Pharyngeal recess: Deep outpocketing posterior to the torus tubarius. Nasopharyngealcarcinomascandevelophere.
Extends from the uvula above to the epiglottis below. Communicates anteriorly with the oral cavity via the oral fauces, above with the nasopharynx, and below with the laryngopharynx. Posteriorly it relates to the upper cervical vertebrae. In the lateral wall is the palatopharyngeal fold.
Extends from the tip of the epiglottis above to the inferior border of the cricoid cartilage below, where it is continuous with the esophagus. Relates to the bodies of C4–C6 vertebrae posteriorly.
Communicates anteriorly with the cavity of the larynx via the laryngeal inlet. Above the inlet is the epiglottis. Adjacent and lateral to the inlet are depressions called piriform recesses (also called piriform sinuses). During swallowing the pharynx is elevated and the epiglottis moves down over the larynx inlet. Food and liquids usually slide around the inlet through the piriform recesses to reach the esophagus.
Clinical correlation
The epiglottic valleculae and piriform recesses are locations where foreign bodies frequently lodge. Fish bones are common culprits.
Construction of the pharyngeal wall
External to the mucosa, the construction of the pharyngeal wall resembles a meat sandwich. Two layers of fascia (a robust pharyngobasilar fascia internally; a thin buccopharyngeal fascia externally) surround the pharyngeal muscles.
The musculature of the pharynx is arranged in two distinct functional layers:
Three circular pharyngeal constrictors.
Vertically arranged pharyngeal elevators.
Pharygeal constrictors
Pharygeal elevators
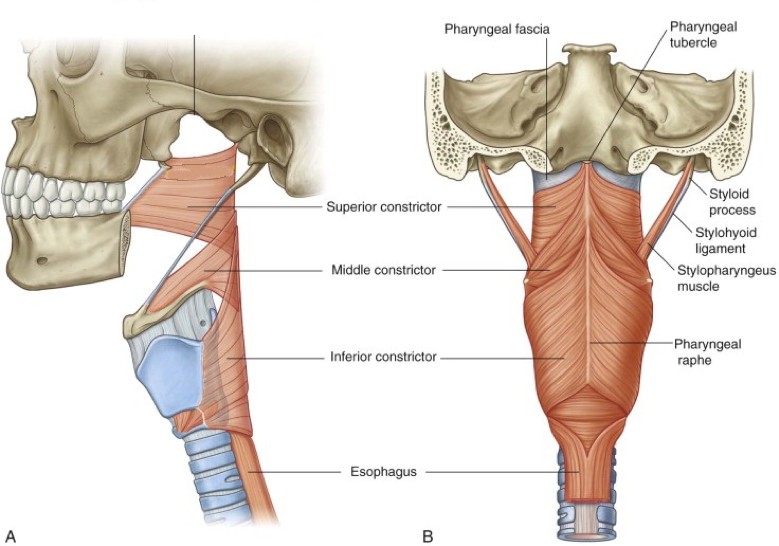
Figure 35.26. Attachments of pharyngeal constrictor muscles. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.198.
Posteriorly, in front of the vertebral column, the constrictors are joined together in the midline with their partners from the opposite side along the pharyngeal raphé (raphe = “seam”), making their boundaries hard to observe.
Anteriorly, the pharynx is open because the constrictors are not fused. Here the origins of the three constrictors are separated, making their identification easier. The three muscles overlap, a reflection of their function in constricting the walls of the pharynx in sequence, from top to bottom, during swallowing.
Superior constrictor
Posterior attachment: Base of skull and pharyngeal raphé
Anterior attachment: Inner surface of mandible, pterygoid hamulus of sphenoid bone, and between these to the pterygomandibular raphé.
Middle constrictor
Posterior attachment: Pharyngeal raphé
Anterior attachment: Greater and lesser horns of hyoid bone
Inferior constrictor
Posterior attachment: Pharyngeal raphé and esophagus below.
Anterior attachment: Thyroid and cricoid cartilages of larynx.
The lower part of the inferior constrictor muscle is said to be functionally independent and in a tonic state of contraction until swallowing ensues. This is the cricopharyngeus muscle. It acts as a sphincter to prevent regurgitation of swallowed food.
These raise and shorten the pharynx to surround the bolus of food in the early stages of swallowing. They also elevate the larynx during phonation (sound production).
Palatopharyngeus muscles were discussed in an earlier section. They are located internal to the constrictor muscles and function to raise the pharynx and narrow the fauces.
Stylopharyngeus muscles: Located external to the constrictors. They elevate the pharynx.
Superior attachment: Styloid process of temporal bone
Inferior attachment: Thyroid cartilage of larynx
Gaps in the pharyngeal musculature
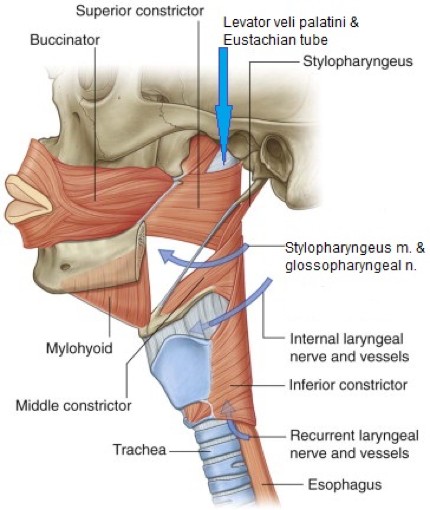
Figure 35.27. Gaps between pharyngeal constrictor muscles indicated by blue arrows. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.200.
The constrictor muscles overlap one another superior to inferior, providing four small gaps between them for passage of structures through the pharyngeal wall.
Gap 1
Above the superior constrictor, between it and the skull base.
Transmits the levator veli palatini muscle and Eustachian tube.
Gap 2
Between the superior and middle constrictors.
Transmits the stylopharyngeus muscle and the glossopharyngeal nerve (CN IX).
Gap 3
Between the middle and inferior constrictors.
Transmits the internal laryngeal nerve (from CN X) and superior laryngeal vessels.
Gap 4
Below the inferior constrictor, between it and the esophagus.
Transmits the recurrent laryngeal nerve (from X) and inferior laryngeal vessels.
Fascial spaces associated with the pharynx
As the pharynx is raised and lowered during swallowing and phonation, it glides along fascial planes created where adjacent fascias in the neck interface.
Buccopharyngeal fascia lines the external surface of the pharynx. Behind the pharynx prevertebral fascia lines the anterior surface of the vertebral column. The potential space between buccopharyngeal and prevertebral fascias is the retropharyngeal space.
The potential space between buccopharyngeal fascia on the lateral side of the pharynx and the medial pterygoid muscle in the infratemporal fossa is the parapharyngeal space. It is external to the peritonsillar space described earlier.
Clinical correlation
Surgeons use fascial spaces as planes to separate structures during surgical dissection. Abscesses and tumors can invade the fascial spaces and spread to other areas (example: from a tooth infection).
Of particular concern is the retropharyngeal space, which descends along the esophagus and could allow an infection to track down into the mediastinum. Large masses in fascial spaces can distort or displace nearby structures. For example, enlarging masses in the parapharyngeal space can obstruct the airway.
A pharyngeal plexus forms on the external wall of the pharynx in the loose connective tissue there.
It receives contributions from the glossopharyngeal (IX) and vagus (X) nerves and postganglionic sympathetic nerve fibers.
Motor supply
All muscles of the pharynx (except ONE) are innervated by the vagus. The stylopharyngeus is the exception, supplied by the glossopharyngeal nerve.
All muscles of the adjacent soft palate (except ONE) are innervated by the vagus. The exception is the tensor veli palatini, supplied by V3.
Sensory innervation
Most of the pharynx, between the levels of the opening of the Eustachian tube and laryngeal inlet, receives sensory fibers from the glossopharyngeal nerve. The oral fauces and palatine tonsils are also supplied by CN IX. Sore throat pain and pain from tonsillitis are carried in CN IX. The afferent limb of the gag reflex is carried in CN IX. Clinical testing of CN IX involves touching the arches of the fauces to elicit a gag reflex.
The upper reaches of the nasopharynx (above the opening of the Eustachian tube) is supplied by the pharyngeal branch of the maxillary nerve (V2).
The region of the laryngopharynx opposite the laryngeal inlet, including the piriformis recesses, is supplied with sensory fibers from the internal laryngeal nerve (CN X).
Mainly from the ascending pharyngeal artery (from the external carotid) and from branches of the facial, descending palatine (from the maxillary artery), and superior and inferior thyroid arteries.
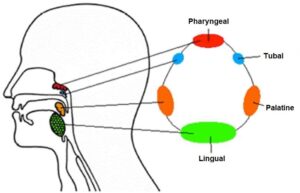
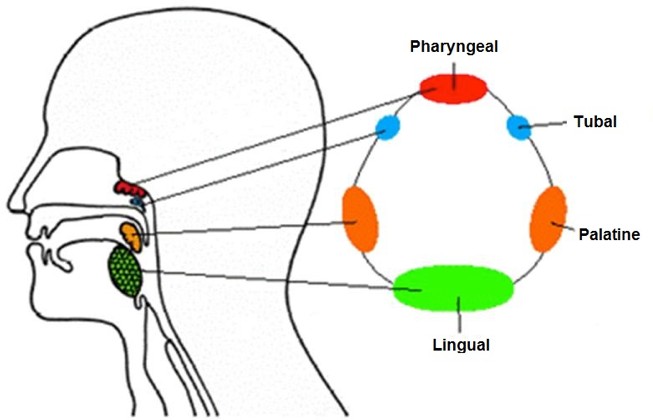
Figure 35.28.OUTLANDER ANATOMY.
Six tonsils (aggregates of lymphoid tissue) within the pharyngeal mucosa are strategically located to surround the nasopharynx and oropharynx. These are the paired palatine and tubal tonsils and the unpaired lingual and pharyngeal tonsils. Together they form an incomplete circle of lymphoid tissue known as Waldeyer’s ring. Their job is to sample inhaled and ingested materials and act as a first line of defense against pathogens. Tonsils are not lymph nodes.
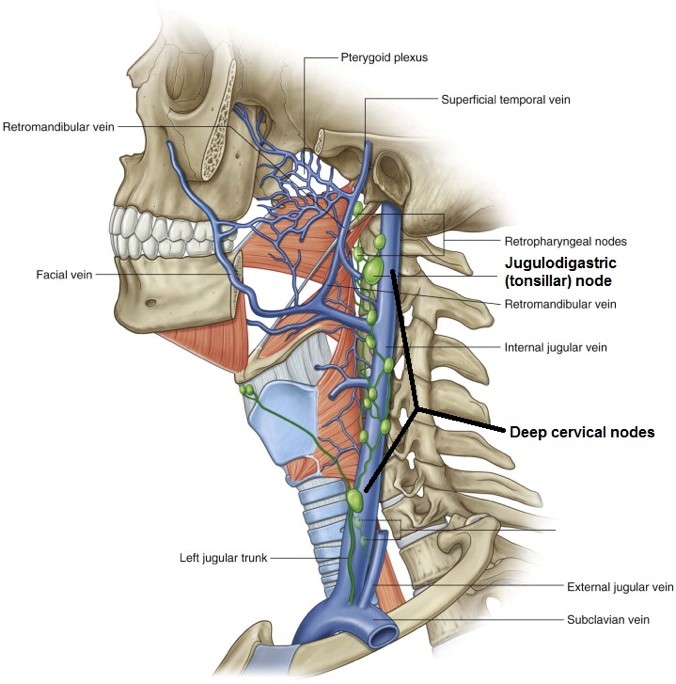
Lymph from the tonsils and the pharynx as a whole eventually drains to deep cervical lymph nodes. In particular, the largest deep cervical nodes, near the angle of the mandible = the jugulodigastric node (tonsillar node). This is why tonsillitis produces swelling and pain at this location.
Figure 35.29. Lymph from the pharynx ultimately reaches the deep cervical lymph nodes, located along the internal jugular vein. The largest of these, the jugulodigastric node, receives lymph from the palatine tonsils. GRAY’S ANATOMY FOR STUDENTS, FIGURE 8.203.
Swallowing (Deglutition)
Solid food is chewed and mixed with saliva in the oral cavity to form a soft bolus that is easier to swallow. Three stages in swallowing are recognized:
The soft palate elevates, sealing off the nasopharynx. The pharynx is elevated, widened, and shortened by contraction of the suprahyoid and pharyngeal elevator muscles.
Contraction of the constrictor muscles in sequence from top to bottom squeezes the pharynx and forces the bolus downward into the esophagus. The cricopharyngeus muscle relaxes early in swallowing, then contracts after the bolus passes by. A descending wave of contraction in the esophagus moves the bolus to the stomach.
Airway protection
The airway is protected by the positioning of the epiglottis over the laryngeal inlet when the pharynx is raised and by contraction of sphincter muscles in the larynx itself. Solids and liquids swallowed are deflected by the epiglottis, causing them to pass around the inlet and through the piriform recesses.
Any solids or liquids that do enter the airway are (hopefully) ejected by a robust cough reflex.