Functional subdivisions of the nervous system are classified not on topography, but according to the organs and tissues they supply:
Somatic nervous system
Supplies structures that we are consciously aware of and have conscious control of: body wall and limbs = “the outer shell of the body.”
Autonomic nervous system (ANS)
Supplies structures we have little or no conscious perception of or control: viscera, smooth muscle, and glands = “the inner guts of the body.”
The somatic and autonomic nervous systems have components in both the CNS and PNS. We focus on the somatic division here. The ANS is covered later.
The somatic nervous system and spinal nerves
Figure 3.1 CORNELIUS ROSSE, M. D., D. SC., STUDY GUIDE FOR GROSS ANATOMY AND EMBRYOLOGY, UNIVERSITY OF WASHINGTON. USED WITH PERMISSION.
Development
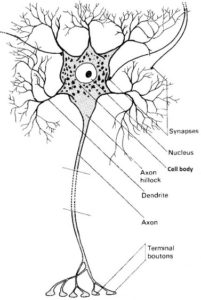
Figure 3.2 The neuron.
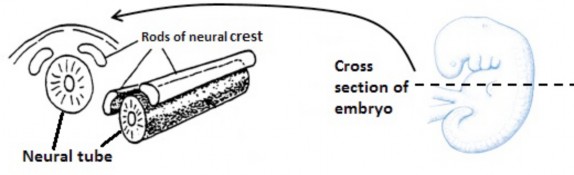
In Week 3 of development the neural plate folded inward to form a neural groove and two neural folds. The tips of the neural folds are made up of specialized nervous tissue called neural crest. Neural folds fuse and detach from the surface, forming a hollow neural tube. As the neural tube is forming, the two clumps of neural crest become detached, forming discrete bars of nervous tissue along the dorsolateral aspect of the neural tube. See Figure 3.1.
The cranial two-thirds of the neural tube becomes the brain; the caudal one- third develops into the spinal cord. The brain and spinal cord comprise the central nervous system.
Cells in the neural tube develop into neuroblasts of the brain and spinal cord. Neuroblasts also arise in the neural crest, but they are located outside the CNS. Neuroblasts develop into neurons (nerve cells) of the CNS and PNS.
The neuron is the functional unit of the nervous system.
Figure 3.3
Neurons possess a cell body (contains the nucleus and cytoplasm) and a variable number of processes that project away from the cell body. Processes are of two types: dendrites and axons. By definition, the axon transmits impulses away from the cell body.
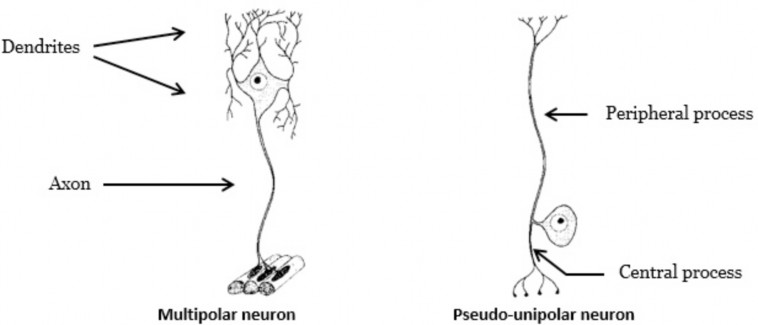
Structurally, neurons are classified by the number of processes they possess. Neurons that have more than two processes (e.g., many dendrites and one axon) are called multipolar neurons (Figure 3.3). Most neurons within the CNS are multipolar neurons as are the neurons in the PNS that supply skeletal muscles (motor neurons) (Figure 3.3).
Neurons in the PNS that carry sensory information (touch, pain, etc.) to the CNS have a single short process that subsequently divides into two longer branches—the peripheral process and the central process. Since they appear to have only one process, but really have two, they are known as pseudo-unipolar neurons.
Functionally, motor neurons carry information away from the CNS to an effector (e.g., a muscle or gland). Motor neurons are multipolar neurons.
Sensory neurons carry information from the periphery (e.g., skin) to the CNS. Sensory neurons are pseudo-unipolar neurons.
Terminology
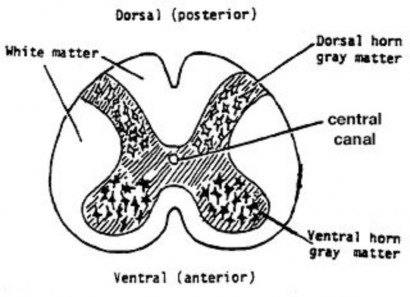
The cell bodies of neurons in the CNS form the gray matter of the spinal cord and brain. Clusters of neuron cell bodies in the CNS that are functionally related are called nuclei (NOT to be confused with the cell’s nucleus). Nuclei are part of the overall gray matter of the CNS.
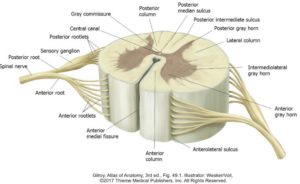
The white matter in the CNS contains axons of neurons wrapped by myelin (a lipoprotein that insulates axons and speeds up the propagation of impulses). Myelin is a fatty substance so it appears white in unstained tissue. A cross-section of the spinal cord shows the gray matter core arranged like the letter “H,” surrounded by white matter. The gray matter is organized into two posterior (dorsal) horns and two anterior (ventral) horns. See Figure 3.4.
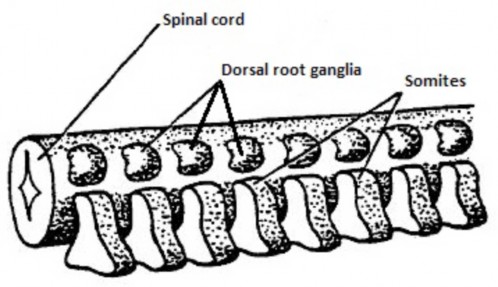
A ganglion is a collection of nerve cell bodies in theperipheral nervous system (outside the CNS). Nearly all ganglia in the body are derived from neural crest. Some neural crest cells remain in their original location, dorsolateral to the neural tube. These neural crest cells close to the spinal cord form segmented clusters of cell bodies called spinal ganglia (dorsal root ganglia). See Figure 3.5. These contain cell bodies of sensory neurons (remember that sensory neurons are structurally pseudo-unipolar neurons).
Figure 3.4 CORNELIUS ROSSE, M.D.,D.SC., STUDY GUIDE FOR GROSS ANATOMY AND EMBRYOLOGY, UNIVERSITY OF WASHINGTON. USED WITH PERMISSION.
Figure 3.5 CORNELIUS ROSSE, M.D., D.SC., STUDY GUIDE FOR GROSS ANATOMY AND EMBRYOLOGY, UNIVERSITY OF WASHINGTON. USED WITH PERMISSION.
Other cells of the neural crest migrate away from the spinal cord, forming such diverse structures as autonomic ganglia (part of the ANS), melanocytes of the skin, enamel of teeth, bones of the middle ear, the medulla of the suprarenal glands, and Schwann cells that insulate neurons in the PNS!
Neuroblasts in the spinal cord form motor neurons. Neuroblasts in dorsal root ganglia become sensory (pseudo-unipolar) neurons. In pseudounipolar neurons, the peripheral process carries impulses toward the cell body, while the central process carries impulses from the cell body to the spinal cord.
Recall that somites are segmented blocks of paraxial mesoderm. Somites are located adjacent to the developing neural tube. As somites are formed, the neural crest also segments into a row of dorsal root ganglia (Figure 3.6). 31 ganglia are formed and they become associated with 31 of the somites.
Figure 3.6 CORNELIUS ROSSE, M.D., D. SC., STUDY GUIDE FOR GROSS ANATOMY AND EMBRYOLOGY, UNIVERSITY OF WASHINGTON. USED WITH PERMISSION.
Figure 3.7 CORNELIUS ROSSE, M.D., D.SC., STUDY GUIDE FOR GROSS ANATOMY AND EMBRYOLOGY, UNIVERSITY OF WASHINGTON. USED WITH PERMISSION.
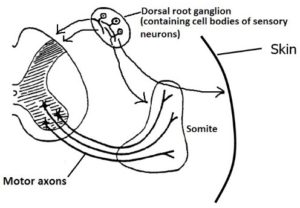
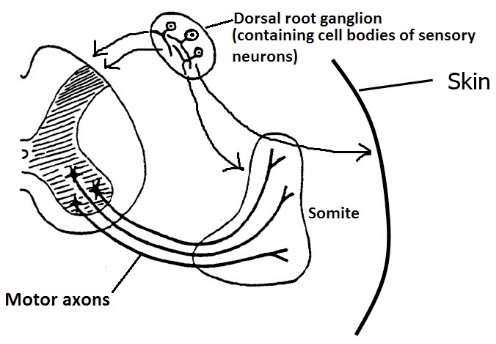
Groups of axons of motor neurons grow out from the ventral horns of gray in the spinal cord and invade the somite closest to their origin. Similarly, the cell bodies of sensory neurons in the dorsal root ganglia sprout processes: the peripheral process grows into the somite as well as the overlying skin. The central processes of sensory neurons grow into the spinal cord where they will synapse with neurons in the dorsal horns of gray in the cord. See Figure 3.7.
Nerve fiber is a term used to describe a long process of a neuron = a peripheral process of a pseudounipolar neuron or an axon of a multipolar neuron.
A nerve is a bundle of nerve fibers (held together by a connective tissue) in the PNS. A nerve contains thousandsof microscopic nerve fibers. Most nerves are mixed, containing both sensory and motor fibers. Nerves are macroscopic structures composed of many nerve fibers. Nerves are found only in the peripheral nervous system—there are NO nerves in the central nervous system.
The spinal nerve
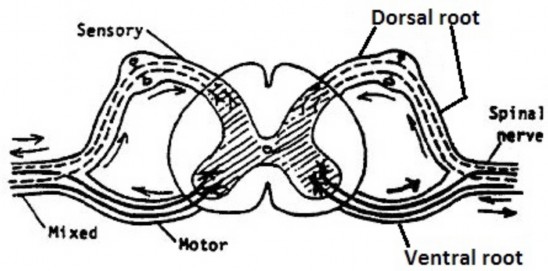
Bundles of central processes of pseudo-unipolar neurons enter the posterior spinal cord at regular intervals as dorsal (posterior) rootlets—these are arranged in two rows (left and right). Likewise, bundles of axons of motor neurons leave the anterior spinal cord at regular intervals as ventral (anterior) rootlets, arranged in two rows (left and right). Rootlets contain many nerve fibers.
At each spinal cord level, dorsal rootlets are gathered together in a single dorsal (posterior) root. The spinal ganglion is associated with the dorsal root, so it is also called a dorsal root ganglion. Likewise, at each level of the spinal cord, ventral rootlets are gathered together into a single ventral (anterior) root. Rootlets and roots are physically located within the vertebral canal of the vertebral column.
The ventral and dorsal roots at each spinal cord level merge, forming a spinal nerve. Spinal nerves are very short. They leave the vertebral column through intervertebral foramina. Dorsal root ganglia are also wedged within the intervertebral foramina.
Figure 3.8 CORNELIUS ROSSE, M.D., D.SC., STUDY GUIDE FOR GROSS ANATOMY AND EMBRYOLOGY, UNIVERSITY OF WASHINGTON. USED WITH PERMISSION.
The ventral root conducts impulses away from the spinal cord—it is entirely motor in function. The dorsal root conducts impulses toward the spinal cord—it is entirelysensory. The spinal nerve contains both sensory AND motor fibers—it is mixed.
Impulses that travel toward the CNS are called afferent (affect = “feeling”); they are conducted along afferent nerve fibers (“afferents” for short). Those that relay information from the body wall and limbs are called somatic afferents.
Impulses that travel away from the CNS are called efferent (“effectors”= muscles, glands, etc. = structures that perform an action); they are conducted by efferent nerve fibers (“efferents”). Those that relay information to the body wall and limbs are called somatic efferents.
Once outside of the vertebral column the spinal nerve divides into a smaller dorsal (posterior) ramus and a larger ventral (anterior) ramus. Dorsal and ventral rami are mixed nerves. See Figure 3.9.
Dorsal rami supply skin on the dorsal side of our bodies (posterior scalp and neck, back, and buttocks) and paravertebral muscles adjacent to the spine.
Ventral rami supply skin on the ventrolateral aspect of our trunk and on our limbs, as well as prevertebral, body wall, and limb muscles.
Figure 3.9 DR. JON MALLATT, UNIVERSITY OF IDAHO WWAMI MEDICAL PROGRAM. USED WITH PERMISSION.
Segmental anatomy of the trunk and spinal nerves
Figure 3.10 Anatomy of a spinal cord segment.
Associated with the spinal cord are 31 pairs of spinal nerves and 31 pairs of dorsal root ganglia.
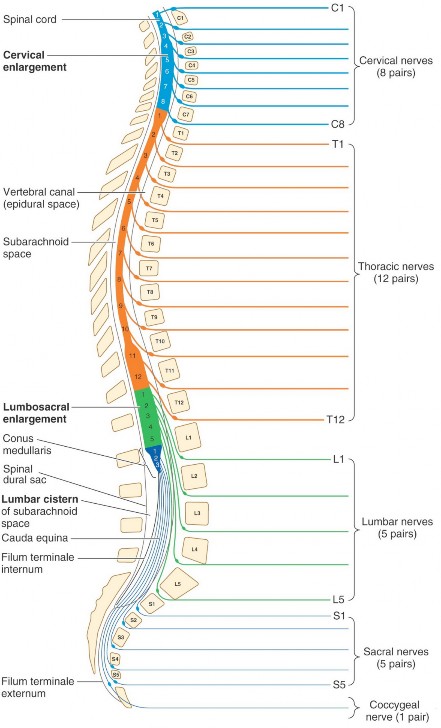
A region of the spinal cord that gives rise to all the ventral rootlets of one spinal nerve and receives all the dorsal rootlets of the same spinal nerve is called a spinal cord segment. Thespinal cord has 31 segments. Spinal nerves and spinal cord segments are identified with a name and number. There are 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal spinal nerves and spinal cord segments.
Spinal nerves exit the vertebral column through an intervertebral foramen directly belowthe corresponding vertebra. Example: Spinal nerve L-1 passes through the intervertebral foramen below L-1 vertebra. This is not true, however, in the cervical region. Why?
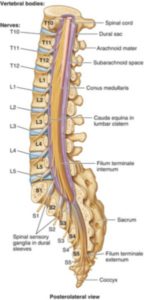
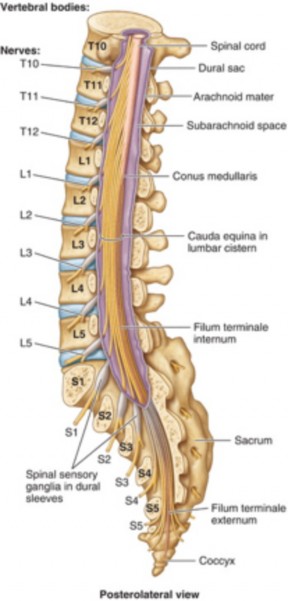
The spinal cord is shorter than the vertebral column. Theinferior tip of the spinal cord ends opposite theintervertebral disc between L-1 and L-2 vertebrae. Therefore, the spinal cord segments do not correspond topographically one-for-one with the vertebrae.
Figure 3.11 MOORE ET AL., CLINICALLY ORIENTED ANATOMY, 7TH ED., FIGURE 4.39.
Have a look at Figures 3.11 and 3.12. Note that a crushing injury of the vertebral column at the level of L-1 vertebra would most likely NOT damage the L-1 segment of the spinal cord—instead L-1 vertebra is roughly at the level of the L-5 spinal cord segment. The sacral segments in the spinal cord are contained within the tapered inferior part of the cord (the conus medullaris).
Realize however, that lumbar, sacral, and coccygeal spinal nerves DO exit the vertebral column through an opening below their corresponding vertebrae. This means that the dorsal and ventral rootsthat form these spinal nerves are LONG—in order to reach their appropriate vertebral level below. See Figure 3.11.
Figure 3.12 Note that the lower spinal cord segments DO NOT correspond one-to-one with the vertebrae.
The long dorsal and ventral roots of lumbar, sacral, and coccygeal spinal nerves are gathered together in a bushy structure within the vertebral canal (below vertebra L-1) that resembles a “horse’s tail”—thus it is given the name cauda equina. Below vertebra L-1, there is NO spinal cord—instead, there is a cauda equina.
Like the spinal cord and spinal nerves, all structures derived from the somites are segmentally arranged. Examples: vertebrae and ribs (from sclerotomes), trunk muscles (from myotomes), and dermis of skin. The distribution of spinal nerves to all of these elements is segmental.
Recite this mantra
There’s a spinal nerve for every body “segment.”
The spinal meninges and meningeal spaces
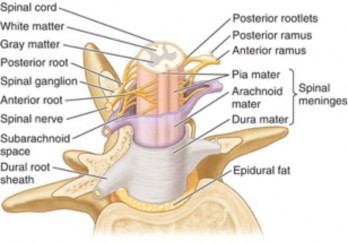
The meninges (Greek = “membranes”) are three layers of protective tissue that surround both the brain (cranial meninges) and spinal cord (spinal meninges). From external to internal the layers are the dura mater, arachnoid mater, and pia mater.
The dura mater (Latin = “hard mother”) contains dense connective tissue. The spinal dura is connected above to the skull along the rim of the foramen magnum. Above this it is continuous with the cranial dura mater around the brain. Below, it extends down into the sacral canal, as far inferiorly as S-3 vertebra. Laterally, the dura encloses the spinal nerves and extends into the intervertebral foramina where it blends with the outer layer of the nerves (epineurium).
The arachnoid mater (Latin = “cobweb mother”) is the middle layer of meninges. It is a thin layer of loose connective tissue that clings to the internal surface of the dura mater. Thin strands of arachnoid (trabeculae) extend inward (like cobwebs!) to attach to the pia mater on the spinal cord.
There is no space between the dura and arachnoid—only a thin layer of lubricating fluid. Thus, the so-called subdural space is a potential space.
The dura and arachnoid cling together and loosely surround the spinal cord and roots (unlike the pia mater, which is closely adherent), producing a double-layered sheath called the thecal sac. Sleeves of the thecal sac extend laterally to surround the spinal nerves as they exit the intervertebral foramina. The thecal sac contains the spinal cord and the cauda equina.
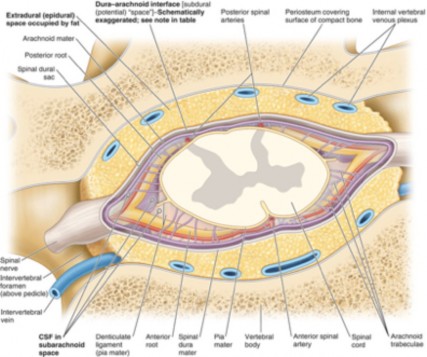
The thecal sac is separated from the bony walls of the vertebral canal by the epidural space. This space extends from the skull base above to the sacral hiatus below. The epidural space contains loose connective tissue, fat, and a large plexus of veins, the internal vertebral venous plexus.
Clinical correlation
Epidural nerve blocks are delivered by injecting an anesthetic or analgesic into the epidural space outside the thecal sac, near the sleeves that surround the spinal nerves. This affects selective spinal nerves (and their dermatomes) without affecting the spinal cord itself and profoundly blocking entire body regions. Epidural anesthesia can numb an area prior to surgery. Epidural analgesia helps manage pain, such as that due to labor during childbirth.
The pia mater (Latin = “tender mother”) is a delicate layer of loose connective tissue that snuggly invests the spinal cord, rootlets, and roots. Small blood vessels that supply the spinal cord and spinal nerve roots course within the pia.
Along the sides of the spinal cord, tent-shaped extensions of the pia project laterally through the arachnoid to attach to the dura. These denticulate ligaments anchor the spinal cord within the dura and provide it with some stability.
At the inferior tip of the spinal cord (conus medullaris), the pia continues as a long strand called the filum terminale. This extends through the thecal sac at S-3. Below this, the filum terminale is invested by the thecal sac (dura + arachnoid) and extends downward to attach to the coccyx.
Figure 3.15 MOORE, CLINICALLY ORIENTED ANATOMY, 8TH ED., FIGURE 2.41.
Between the pia and arachnoid layers is the subarachnoid space. This space contains cerebrospinal fluid (CSF). Thin extensions of the arachnoid mater (trabeculae) criss-cross the subarachnoid space like cobwebs. The spinal subarachnoid space communicates with the cranial subarachnoid space through the foramen magnum. CSF is manufactured in the brain’s ventricles and circulates around the brain and spinal cord in the subarachnoid space. CSF has several functions:
Protection: It acts as a shock absorber around the central nervous system
Provides nutrients
Removes wastes.
The subarachnoid space is especially wide around the cauda equina—this part of the space is known as the lumbar cistern.
Clinical correlation
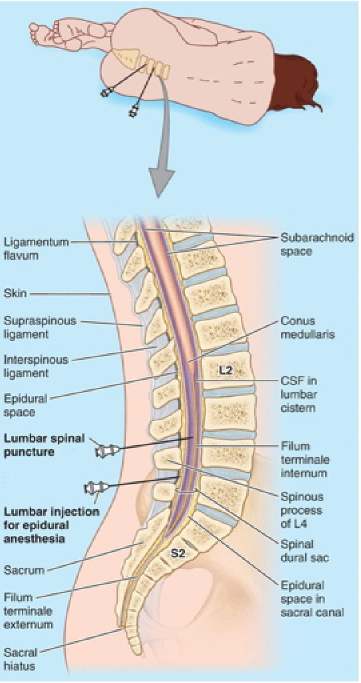
For diagnostic purposes, the composition of CSF may need to be determined or its pressure measured. To obtain CSF, a lumbar puncture procedure is done. Knowledge of spinal anatomy is critical here. A lumbar puncture is performed by placing a hollow needle between vertebrae, through the thecal sac, and into the subarachnoid space. It is usually done between L-3 and L-4 or L-4 and L-5. These are preferred locations because:
they are below the termination of the spinal cord, thus avoiding its injury
the subarachnoid space is larger in this region (lumbar cistern)
the spaces between adjacent vertebral laminae/arches are wide in the lumbar region.
To make the spaces between vertebrae even wider, the patient is asked to bend forward while sitting down or lying on their side. The needle is placed in the back between vertebrae typically in the midline. The resistance offered by ligaments (such as the interspinous ligament or ligamentum flavum) and the subsequent “giving way” when the needle penetrates them informs the clinician that the needle tip has passed into the epidural space. From here the needle is advanced through the thecal sac into the subarachnoid space.
The embryonic terms “myotome” and “dermatome” should not be confused with the clinical concepts of myotome and dermatome.
Larger muscles (as in the limbs) are usually made up of more than one myotome, and thus are innervated by more than one spinal nerve. Knowledge of myotome maps can be useful when trying to diagnose injury to spinal nerves. For example, weakness in elbow flexion could be due to damage of C-5 or C-6 spinal nerves, since C-5 and C-6 are the myotomes corresponding to the prime movers of elbow flexion.
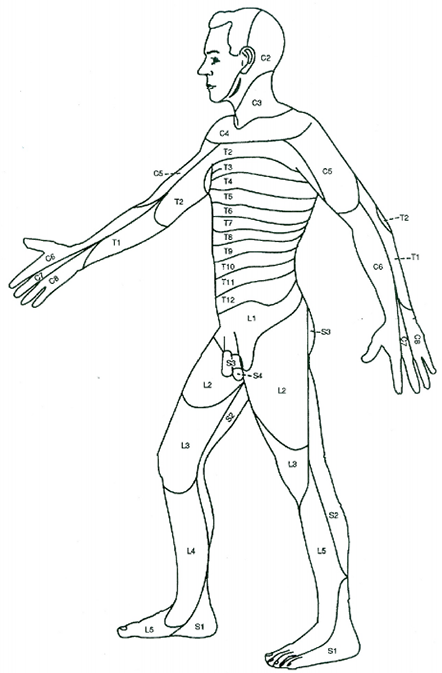
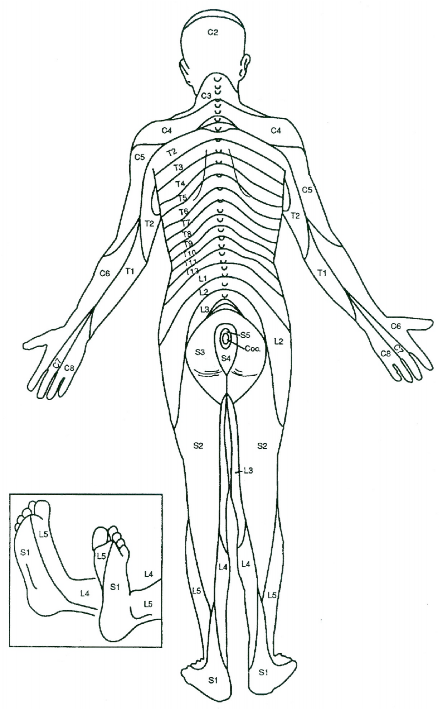
For example, the T-10 dermatome is a patch of skin supplied by the T-10 spinal nerves. This strip of skin is located at the level of the umbilicus (“belly button”). You should understand the dermatome “map” of the trunk—because it can give you clues to certain pains experienced by patients. For example, a case of appendicitis “refers” its pain to the dermatome that crosses the umbilicus = the T-10 dermatome. Referred pain is pain perceived at a location in the body other than the site where the painful stimulus originates.
Two classical dermatome maps were developed by Foerster (1933) and by Keegan and Garrett (1948). The Foerster maps are preferred by neurologists. We will use the Foerster maps in our anatomy course—they are printed for your perusal in Figure 3.17 and Figure 3.18.
Figure 3.17 INTERNATIONAL STANDARDS FOR NEUROLOGICAL CLASSIFICATION OF SPINAL CORD INJURY (AMERICAN SPINAL INJURY ASSOCIATION, 2011).
Figure 3.17 INTERNATIONAL STANDARDS FOR NEUROLOGICAL CLASSIFICATION OF SPINAL CORD INJURY (AMERICAN SPINAL INJURY ASSOCIATION, 2011).