Before embarking on the anatomy of the foot, let’s keep in mind how it contrasts with the hand.
The upper limb has great mobility and the hand has grasping and sensory functions.
The lower limb in general is built for stability to bear the weight of the entire body and for the purpose of locomotion. Although the hand and foot have many similarities in structure, the anatomy of the foot is adapted for weight bearing and walking.
Skeleton of the foot
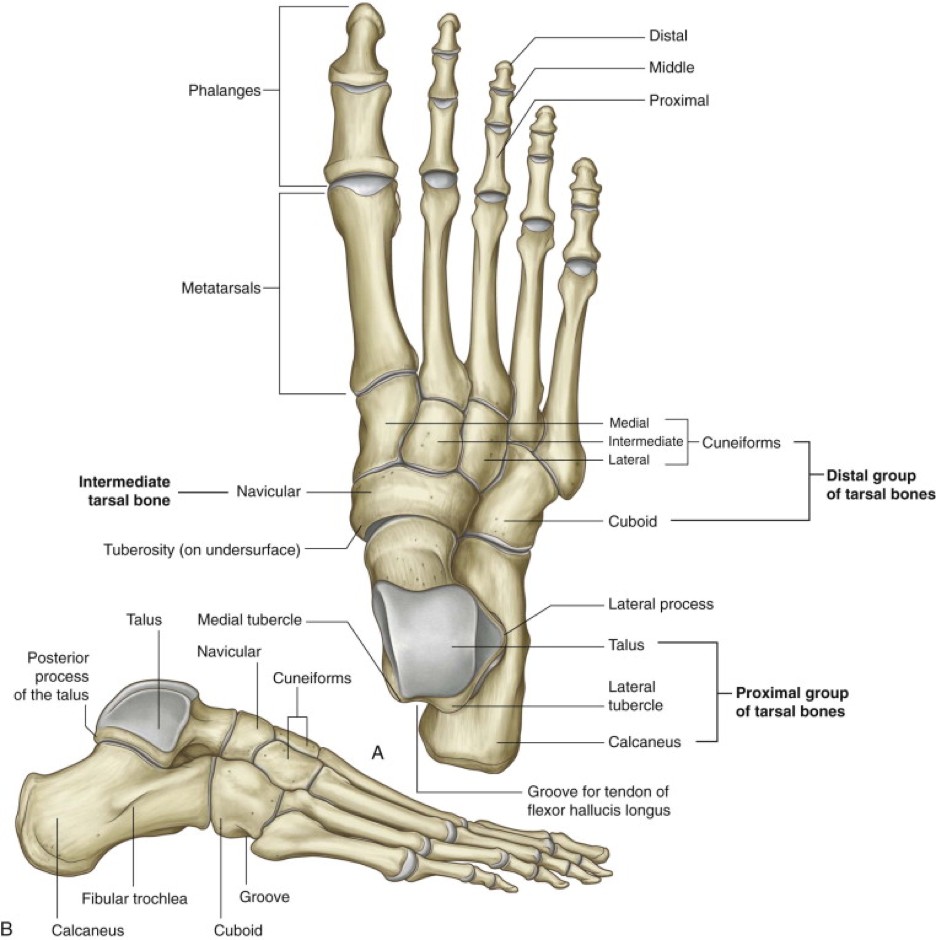
Figure 28.1 GRAY’S ANATOMY FOR STUDENTS, 3RD EDITION.
Like the hand, the skeleton of the foot consists of proximal, intermediate, and distal bones.
The proximal bones are the seven tarsal bones. Their arrangement in two rows is more difficult to appreciate as compared to the carpal bones of the hand. The talus and calcaneus are the most proximal bones of the foot and they are the counterparts of the four proximal carpal bones in the wrist. The distal tarsal bones are the navicular, cuboid, and the three cuneiform bones (medial, intermediate, and lateral). These five bones are the counterparts of the distal row of carpal bones in the hand.
Talus
The talus (Latin = ankle bone) articulates with the tibia and fibula above—it is the only tarsal bone to do so. Therefore, the talus transmits the weight of the body above it to the rest of the foot. The talus has three parts: the trochlea is the “dome” of the talus—it participates in the ankle joint and articulates with the tibia and fibula. The body of the talus articulates below with the calcaneus. The head of the talus projects forward and articulates with the navicular.
Calcaneus
The calcaneus (Latin = heel) is the largest tarsal bone. The talus rests on its upper surface. The bulky posterior surface of the calcaneus projects backwards, forming the “heel.” The calcaneal (Achilles) tendon attaches to the posterior surface of the calcaneus.
Navicular
The navicular is on the medial side of the foot, where it articulates with the head of the talus. It is so named because the ancients thought it resembled a boat. The tuberosity of the navicular is prominent and can be easily palpated on the medial foot—the tendon of the tibialis posterior muscle can be felt attaching to it.
Cuboid
The cuboid is on the lateral foot and needs no further explanation.
Cuneiform bones
The three cuneiform bones (cuneiform is Latin for wedge-shaped) line up between the cuboid laterally and the medial border of the foot. The medial cuneiform is the largest of the three bones. The cuboid and the threec uneiform bones line up in a row and articulate anteriorly with the five metatarsal bones.
The metatarsals are the intermediate bones of the foot. They are numbered I to V (roman numerals) from medial (big toe side) to lateral. The first metatarsal is the largest. Each metatarsal has a head (distal), a shaft, and a base (proximal). The bases of the metatarsals articulate with the four distal tarsal bones, discussed earlier. The base of the fifth metatarsal bone has a prominent tuberosity—which is easily palpable on the lateral foot. The tendon of the fibularis brevis muscle attaches to it.
The distal bones of the foot are the phalanges. They are arranged identical to those of the hand. The big toe (hallux) has proximal and distal phalanges. The other toes have proximal, middle, and distal phalanges.
Let’s tackle the rest of foot anatomy by considering its two surfaces (much the same way we did for the hand):
The dorsum of the foot
The plantar aspect of the foot (“sole” of the foot).
The subtalar joint
The subtalar joint is the intertarsal joint between the inferior talus and superior surface of the calcaneus. It is a plane type joint. The joint surfaces allow the foot to rock from side to side, producing inversion and eversion movements of the foot.
Dorsum of the foot (superior surface of the foot)
Fascia
There is not much superficial fascia on the dorsum of the foot. It contains superficial nerves and vessels (dorsal digital nerves and vessels) and the dorsal venous plexus of the foot. The dorsal venous plexus of the foot gives rise to both the great and small saphenous veins. Because of the paucity of superficial fascia, the tendons of the long muscles of the anterior leg are clearly visible as they pass onto the dorsum and the bones of the foot are easily palpable.
The deep fascia of the dorsum is continuous above with the superior and inferior extensor retinacula of the leg near the ankle joint.
Muscles on the dorsum
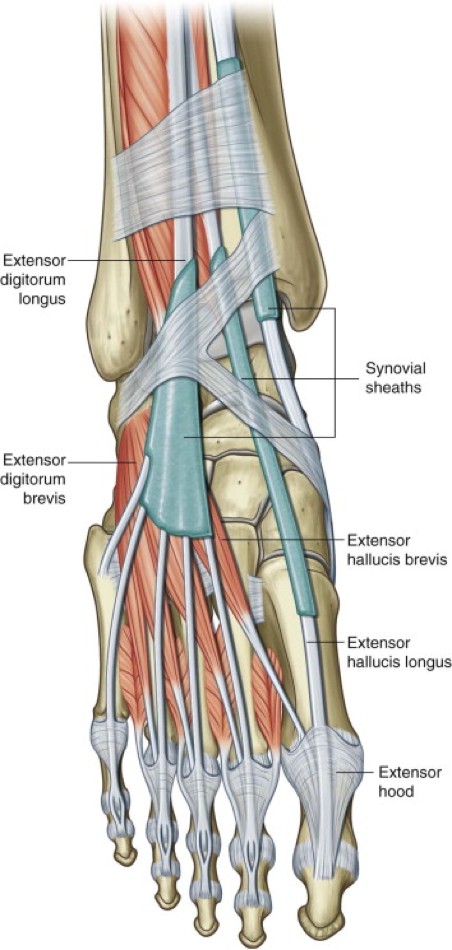
Figure 28.2 GRAY’S ANATOMY FOR STUDENTS, 3RD EDITION.
The tendons of the tibialis anterior, extensor hallucis longus, and extensor digitorum longus can be traced from the leg onto the dorsum of the foot as they emerge from the inferior extensor retinaculum. They can be followed distally to their insertions on the tarsal bones and toes.
There are two intrinsic foot muscles on the dorsum. Neither is very robust.
1
The extensor digitorum brevis arises from the superior surface of the calcaneus and from the lower extensor retinaculum. Distally, it splits into four tendons. The lateral three tendons fuse with the tendons of the extensor digitorum longus.
2
The medial tendon of the extensor digitorum brevis inserts on the distal phalanx of the big toe separate from the extensor digitorum longus tendon. Because of this, the belly and tendon of the first head of the extensor digitorum brevis is given a separate name: the extensor hallucis brevis.
Both muscles on the dorsum of the foot extend the toes. They are innervated by the deep fibular nerve.
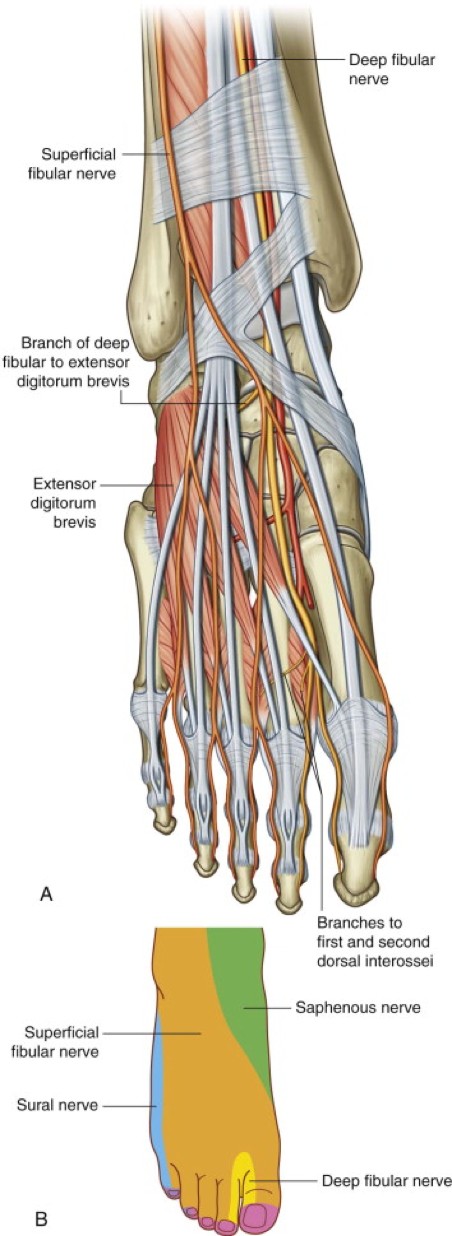
Figure 28.3 Gray’s Anatomy for Students, 3rd edition.
Sensory: Both the superficial and deep fibular nerves give rise to dorsal digital nerves that supply sensation to the dorsum of the foot. However, sensation to most of the dorsal foot is supplied by the superficial fibular nerve. The deep fibular nerve supplies sensation only to the skin between the first and second toes.
Motor: the two intrinsic muscles of the dorsal foot are innervated by the deep fibular nerve.
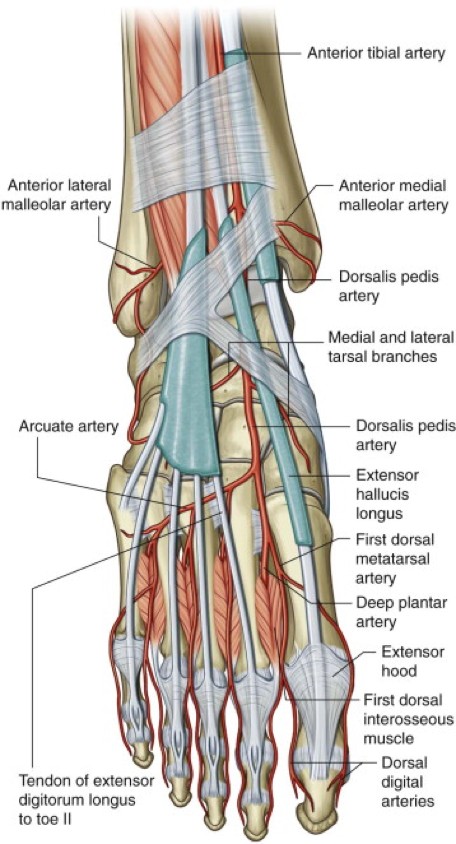
Figure 28.4 GRAY’S ANATOMY FOR STUDENTS, 3RD EDITION.
The main blood supply to the dorsum of the foot is from the dorsalis pedis artery. There is some variation to the origin and course of this artery, but it is usually the direct continuation of the anterior tibial artery from the leg on to the foot. In rare cases, the dorsal pedis artery is formed by a perforating branch from the fibular artery. The dorsalis pedis runs distally on the dorsum of the foot toward the interspace between the first and second digits. The major branches of the dorsalis pedis are the deep plantar artery and the arcuate artery of the foot. Small dorsal metatarstal arteries arise from the latter.
Clinical correlation
The pulse of the dorsalis pedis artery can usually be palpated by compressing the artery against the tarsal bones, just lateral to the extensor hallucis longus tendon. It is often palpated by clinicians to assess peripheral blood flow in the lower limb.
However, because of its variation in origin and course, the pulse of the dorsalis pedis may be absent or faint, and this should not be confused for pathological occlusion of the vessel. Also, it has been reported that up to 40% of normally palpable pulsations of the dorsalis pedis can be eliminated by active or passive plantar flexion of the foot (see Palpation of Dorsalis Pedis Pulse). Therefore, the pulsations of the dorsalis pedis artery should not be used alone to gauge peripheral blood flow—the posterior tibial artery is a more reliable indicator.
Plantar aspect of the foot (sole of the foot )
The plantar surface of the foot contacts the ground when standing upright.
Fascia
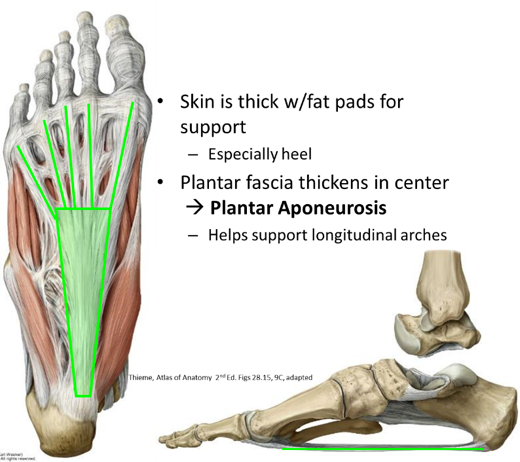
The superficial fascia on the plantar foot is odd in that it is firmly attached to the underlying deep fascia. Thus, the skin doesn’t slide along the plantar foot as it typically does in other regions of the body. It also contains localized compartments of fat adjacent to bony surfaces. These modifications of the superficial fascia provide padding over the weight bearing areas, especially in the “heel” and “ball” of the foot near the big toe.
The deep fascia is similar to that of the hand. It is thickened in the center of the plantar foot to form the plantar aponeurosis. Distally the plantar aponeurosis sends extensions (digitations) into the toes. Proximally, the plantar aponeurosis attaches to a tuberosity on the medial calcaneus. Inflammation of the plantar aponeurosis (plantar fasciitis)is especially painful here where the aponeurosis attaches to bone.
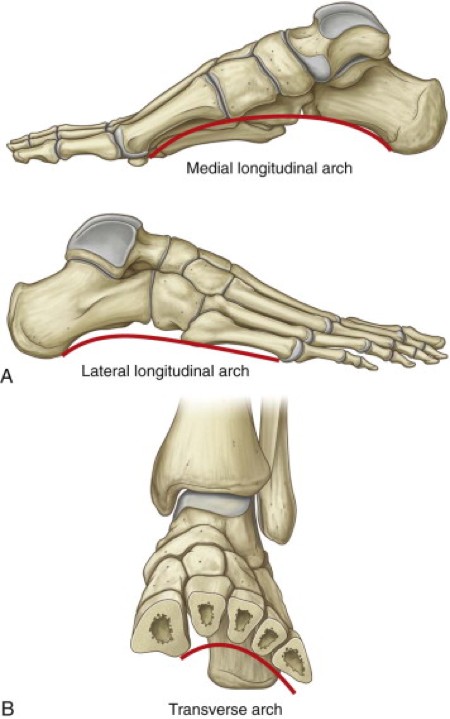
Arches of the foot
Figure 28.5 GRAY’S ANATOMY FOR STUDENTS, 3RD EDITION.
The plantar surface of the foot is not flat. Therefore, the bones of the foot do not lie in the same horizontal plane. Instead, the bones and soft tissues of the foot are arranged in arches, with concavities that face inferiorly. The purpose of the arches are to absorb and distribute the forces applied to the foot when standing and walking. If the foot were flat, this would not happen.
There are three arches: two longitudinal arches (medial and lateral) and one transverse arch. The medial longitudinal arch is the largest. The arches are maintained by ligaments and muscles.
Muscles of the foot
Extrinsic muscles
Intrinsic muscles
Extrinsic muscles act of the foot from afar—their proximal attachments are in the legs, while their long tendons insert distally on bones of the foot. These muscles were described in earlier chapters.
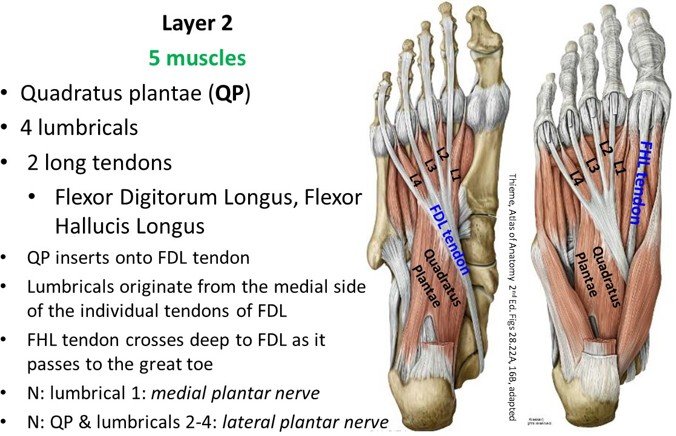
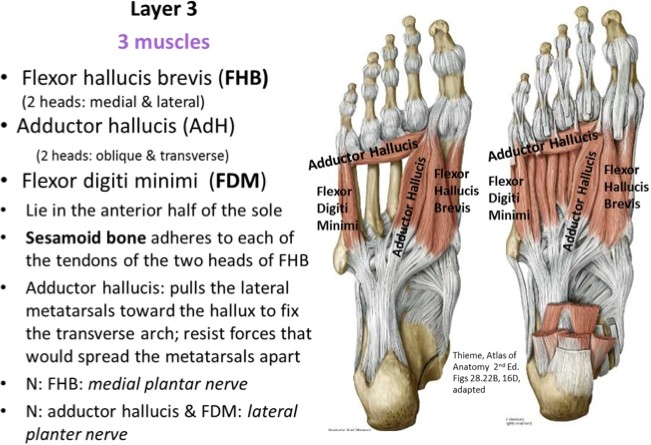
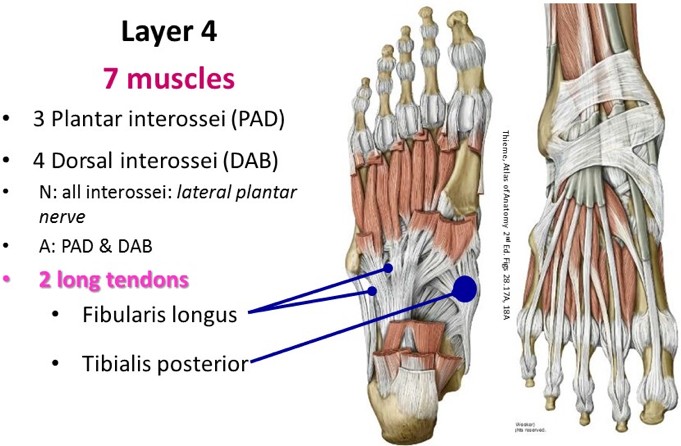
The intrinsic muscles both originate and insert within the foot. There are many of them—18 on the plantar side of the foot and 2 on the dorsal side. Gulp! The intrinsic muscles on the plantar foot are arranged in layers. It is wise to consider theactions of these muscles as a group—their overall function is to maintain the arches ofthe foot and prevent them from flattening. Most of the muscles don’t function very well in isolation—although some individuals have fine control over them, but this is not particularly important to the overall functioning of the foot. Intrinsic muscles are innervated by the medial and lateral plantar nerves—the terminal branches of the tibial nerve. Like the hand, one of the nerves is dominant in innervating muscles. In the foot, the lateral plantar nerve innervates most of the intrinsic muscles, so it is the counterpart of the ulnar nerve in the hand.
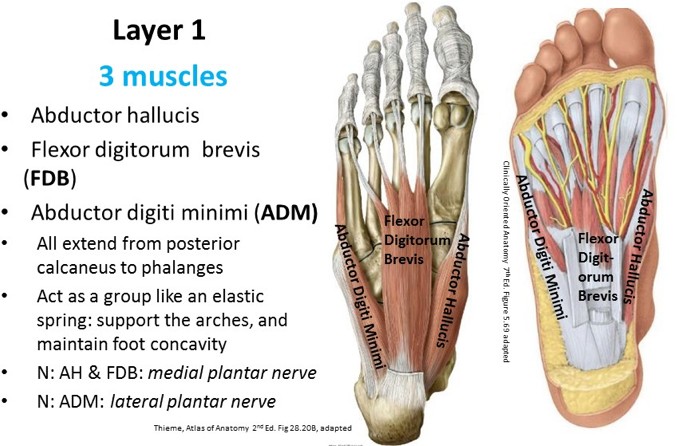
Layers of muscles on the plantar foot
The following organization by layer is useful in dissection or surgery as it is the sequence in which the muscles and other structures are encountered. The skin is very thick over the heel, lateral foot, and ball of the foot. The plantar fascia is just deep to the skin, and like the palm, it covers the first layer of muscles.
Figure 28.6
From the calcaneus, fans out over the sole, becomes broader and thinner distally
Strong, greatly thickened central part, and weaker and thinner medial and lateral portions
Longitudinally arranged dense fibrous bands help support the longitudinal arches of the foot and hold the parts of the foot together.
Divides into five bands that split to enclose the digital tendons
Attached to the margins of the fibrous digital sheaths
From the central part: vertical septae extend deeply to form the medial, lateral, and central compartments of the sole of the foot
Nerves and vessels may be described according to these compartments, but muscles are usually described (and more easily, I might add) by layers
Unstretchable; calcaneus fractures before the aponeurosis stretches. When on your tip toes: increased tension on the plantar aponeurosis, and the navicular increases its stability
Four muscular layers: specialized to maintain the arches of the foot and to enable one to stand on uneven ground. The rule of exclusion works well in innervation!
Gross actions (versus fine ones in the hand): resist forces that try to reduce the medial longitudinal arch when weight is put at the heel and transferred to the ball of the foot and the hallux during gait
Layers of Plantar Muscles
Figure 28.7Figure 28.8Figure 28.9Figure 28.10
Clinical correlation: Plantar fasciitis
Pain on plantar foot and heel with point tenderness at the aponeurosis’ attachment to the medial tubercle of the calcaneus.
Onset of pain: Just anteromedial to calcaneus, point tender
Pain most severe: When getting out of bed in the morning or getting up from resting
Pain increases with passive extension of hallux and may hurt more by dorsiflexion and/or weight bearing
Most common hindfoot problem in runners, but is also seen in high-impact aerobics, especially if wearing inappropriate shoes
Nonsurgical treatment:
Manage: Ice, orthotics, stretch calves
Biomechanics
Neurovasculature of the sole of the foot
Figure 28.11
Two neurovascular planes: Superficial between layers 1 and 2, and deep between layers 3 and 4
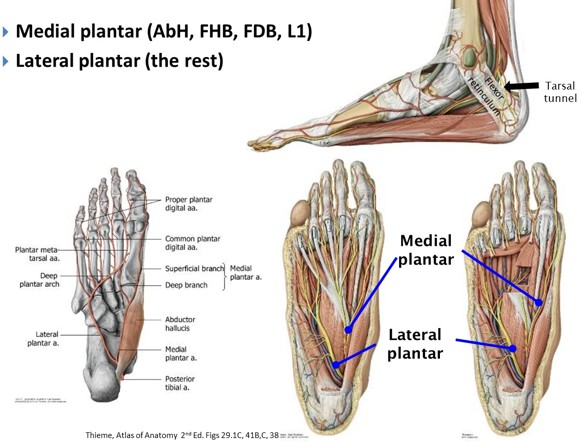
Medial plantar nerve: Arises from tibial nerve deep to flexor retinaculum
Enters the sole by passing deep to the abductor hallucis
Runs between layers 1 and 2 just lateral to the flexor digitorum brevis
Terminates near the bases of the metatarsals by dividing into three sensory branches (medial 3½ digits and sole proximal to them)
Medial plantar artery: Follows same course; gives rise to the medial 1½ plantar digital arteries
Lateral plantar nerve and artery: Course deep to abductor hallucis and run laterally between layers 1 and 2
Deep branches arch medially across the foot between layers 3 and 4
Artery forms the deep plantar arch with the deep plantar artery (from dorsalis pedis)
Arch gives off plantar metatarsal arteries, and rest of the plantar digital arteries
Cutaneous nerves on the sole of the foot
Sole: From the medial and lateral plantar nerves. See Figure 28.12.
Note that the plantar surfaces of digits one, two and three are supplied by the medial plantar nerve, plus half of digit four. The plantar surface of digit five, plus half of digit four, is supplied by the lateral plantar nerve. This sensory innervation pattern on the sole of the foot should remind you of the innervation pattern of the fingers on their palmar surfaces.
Figure 28.12 GRAY’S ANATOMY FOR STUDENTS, 3RD EDITION.
Figure 28.13 GRAY’S ANATOMY FOR STUDENTS, 3RD EDITION.
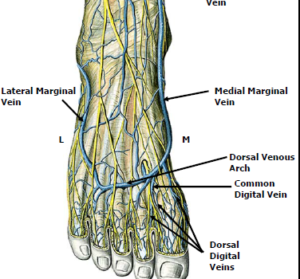
Venous and lymphatic drainage of the foot
Veins on the medial side of the foot converge and loop around as the medial marginal vein, passing anterior to the medial malleolus to become the great saphenous vein
On the lateral side the lateral marginal vein loops around posterior the lateral malleolus, and will become the small saphenous vein


 Veins on the medial side of the foot converge and loop around as the medial marginal vein, passing anterior to the medial malleolus to become the great saphenous vein
Veins on the medial side of the foot converge and loop around as the medial marginal vein, passing anterior to the medial malleolus to become the great saphenous vein