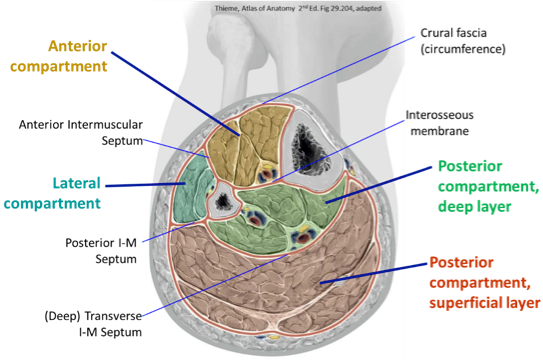
The deep fascia of the thigh (fascia lata) continues on to the leg, forming a dense, snug-fitting layer called the crural fascia
The crural fascia, intermuscular septa, bones of the leg,and interosseous membrane separate the leg into anterior, lateral, and posterior compartments
Figure 26.1
Clinical correlation: Compartment syndrome
The deep fascia in the limbs is a tough inelastic material: swelling in the leg (e.g., due to trauma, such as a tibial fracture) increases the intra-compartmental pressure, which could rise above the hydrostatic pressure in the capillaries within the compartment and prevent oxygen from reaching the tissues.
Muscles and nerves become ischemic (painful!!) compartment syndrome.
Usually affects the anterior compartment of the leg. Vigorous exercise or sudden overuse can cause the anterior leg muscles to swell, increasing the pressure within the compartment.
Pressure usually not high enough for vascular collapse. Not medical emergency.
Acute compartment syndrome: Acute trauma (fracture, kick to leg).
Since ischemia can cause muscle necrosis in as little as 6 hours, the definitive treatment for compartment syndrome is fasciotomy (incising the deep fascia = cut it open!).
Important signs and symptoms are pain and paresthesia (“pins and needles” sensation). The pain is usually described as “out of proportion” to the findings of the physical exam (more intense than what would be expected from the injury itself ). Pain is aggravated by stretching the muscles in the compartment and is not relieved with analgesia. The anterior compartment of the leg is the most common site for compartment syndrome.
Figure 26.2
Figure 26.3
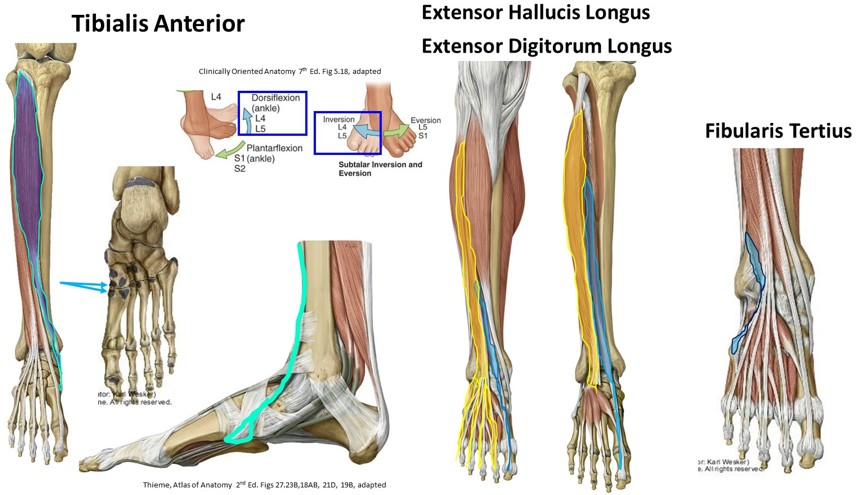
Anterior compartment of the leg
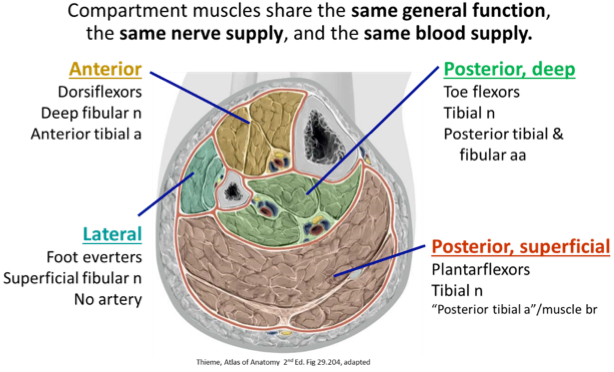
Contains four muscles, whose major action is to dorsiflex the foot at the ankle joint. Two of the muscles also extend the joints of the toes.
Small and variable, partially separated part of EDL; Absent in ~5% of population
Insertion: Dorsum, base of 5th metatarsal
Action: Proprioceptive to protect Anterior Talofibular ligament (from ankle inversions); insignificant dorsiflexion; aids in eversion
Nerve: Deep Fibular nerve
Figure 26.4
Clinical correlation: Weakness or paralysis of muscles in the anterior compartment of the leg
Weakness: May cause audible foot slap immediately after heel contact.
Injury to the common fibular nerve proximally or distally to the deep fibular nerve: Produces Foot Drop (inability to clear the foot during the swing phase of the gait cycle) and an audible foot slap immediately after the heel contacts the ground.
Clinical correlation: Shin splints
Painful compartment syndrome after vigorous and/or lengthy exercise after sudden overuse. Anterior leg muscles swell and reduce blood flow. Cramps may develop if use of the muscles is continued. Reduced dorsiflexion, and increase in pain during pain during passive plantaflexion; stretch, ice, rest.
Other causes: Microtears in periosteum from repetitive microtrauma, stress fractures.
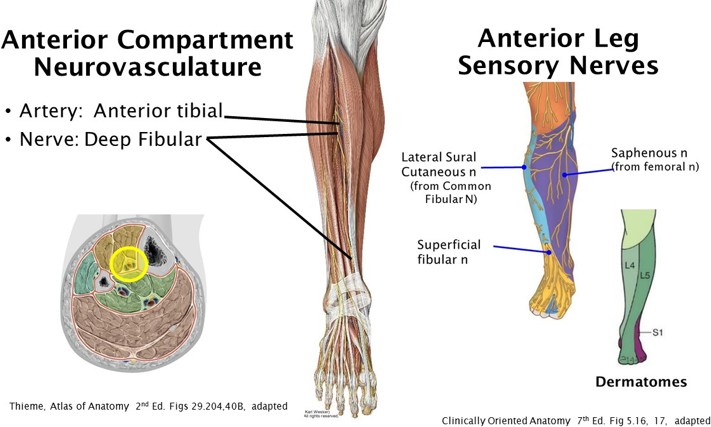
Neurovasculature of the anterior compartment
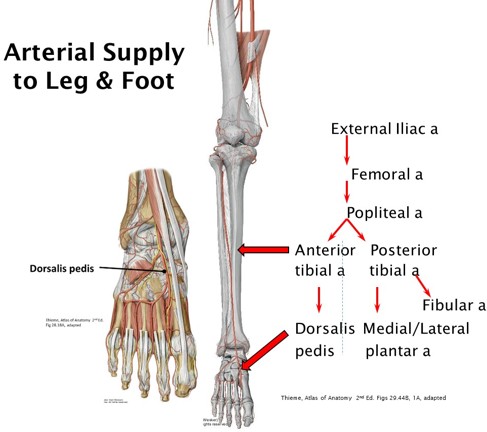
Anterior tibial artery (a branch of the popliteal artery)
Muscles: Deep fibular (peroneal) nerve, from common fibular nerve
Sensory: Saphenous, lateral sural cutaneous, and superficial fibular nerves
Figure 26.5
Figure 26.6
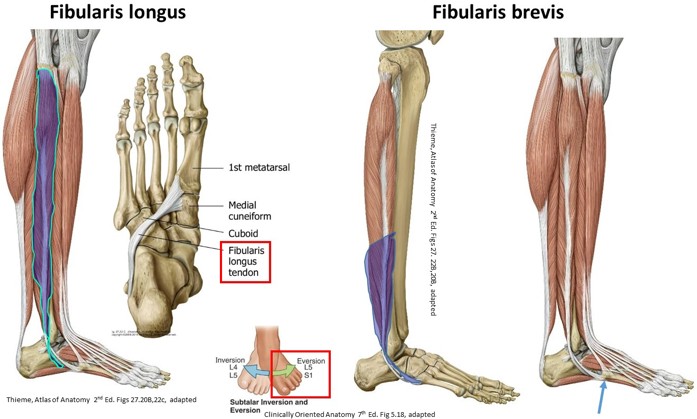
Lateral compartment of the leg
Both muscles in the lateral compartment originate from the fibula, evert the foot, and are innervated by the superficial fibular nerve.
Tendon grooves the posterior surface of the lateral malleolus, lying in common tendon sheath with the fibularis longus; easily traced to insertion
Insertion: Tuberosity of 5th metatarsal
Action: Evert foot; weakly plantarflex
Nerve: Superficial fibular nerve
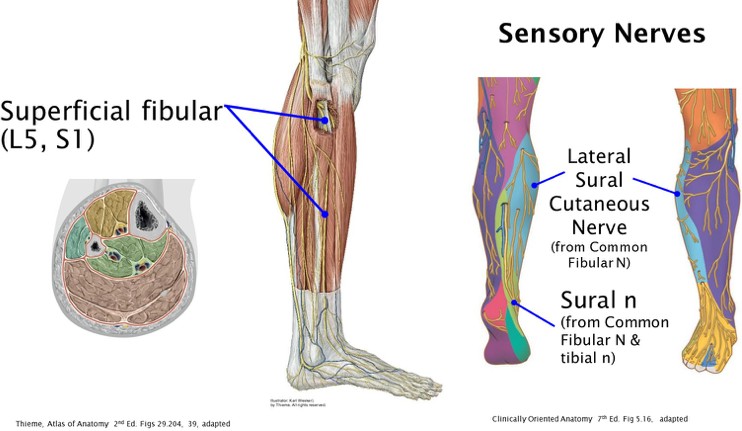
Neurovasculature of the lateral compartment
Figure 26.8
Oddly, the lateral compartment has no primary artery or vein of its own. Instead, the blood supply to the lateral compartment comes from small perforating vessels that arise from the anterior tibial and fibular arteries in the anterior and posterior compartments of the leg, respectively.
Sensory: Lateral sural cutaneous and sural nerves
Muscles: Superficial fibular nerve, a terminal branch of the common fibular nerve
Clinical correlation
When paralyzed by injury to the superficial fibular (peroneal) nerve, the unopposed action of the foot inverters causes the foot to strike the ground on the lateral side during the gait cycle, predisposing the patient to roll the ankle unless an orthosis is used.
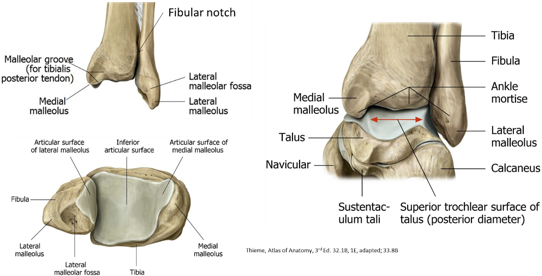
Talocrural (ankle) joint
A uni-axial hinge joint.
The distal fibula and tibia form a bony box (called the ankle mortise) that articulates with the trochlea (dome) of the talus.
Main movements: Plantarflexion and dorsiflexion.
When the foot is dorsiflexed, the trochlea is wedged snuggly into the ankle mortise. When the foot is plantarflexed, the trochlea has a looser fit within the mortise (since the trochlea is narrower posteriorly than it is anteriorly), allowing for slight rotation of the articular surfaces. This is the least stable position of the ankle—therefore, most ankle injuries occur when the foot is plantarflexed at the ankle.
Crossed by many tendons tightly bound down by thickenings of deep fascia called retinacula.
Osteology
Figure 26.9
Distal tibia
Medial Malleolus
Fibular notch
Distal fibula
Lateral Malleolus
Malleolar Fossa
Talus
Trochlea (dome), body, and head
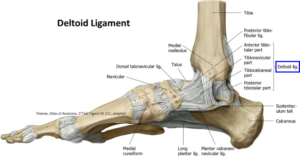
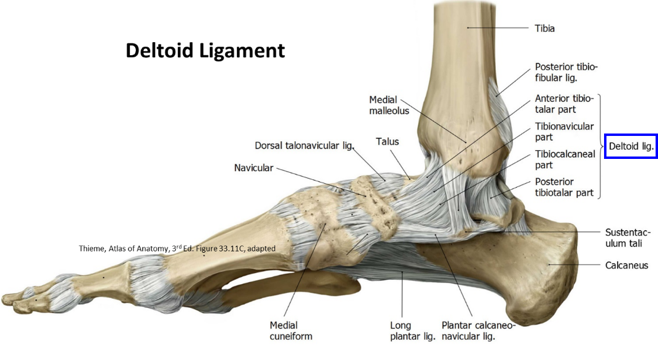
Articular capsule and ligaments
Fibrous capsule surrounds the talocrural joint
Reinforced externally by ligaments that limit excessive inversion and eversion
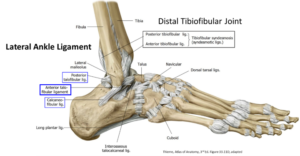
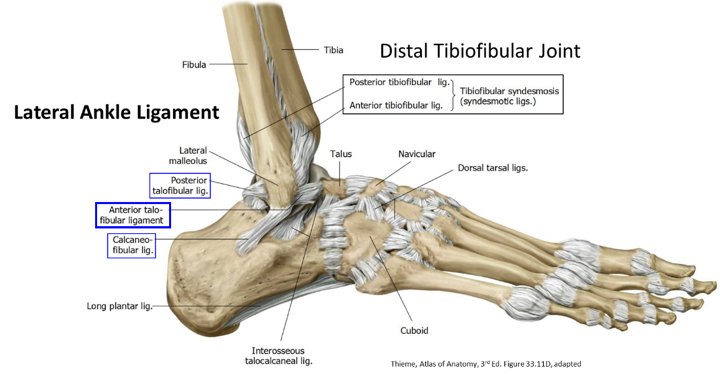
Three ligaments that attach lateral malleolus to the talus and calcaneus
Anterior talofibular ligament: Most commonly sprained ligament of the body
Flat band that extends anteromedially from lateral malleolus to the neck of the talus
Posterior talofibular ligament: Runs horizontally medially and slightly posteriorly from the lateral malleolus to the lateral tubercle of the talus
Calcaneofibular ligament: Round cord that passes posteroinferiorly from the tip of the lateral malleolus to the lateral surface of the calcaneus
Crossed superficially by the tendons of the fibularis longus and brevis
Distal tibiofibular articulation
A syndesmosis type joint
The distal leg must be stable for normal ankle function
The distal tibia and fibula are strongly joined together by an interosseous ligament that runs internally between the bones and two external ligaments: The anterior and posterior tibiofibular ligaments.
Athletes who suffer a “high ankle sprain” have damaged their distal tibiofibular articulation.
Notice how radically different the two tibiofibular articulations (proximal and distal) are compared to their counterparts in the forearm: the proximal and distal radio-ulnar joints, whose rotational movements allow for supination and pronation in the forearm—motions that are not wanted in the leg!!
Structures that cross the talocrural (ankle) joint
Tendons in the anterior, lateral, and posterior crural leg compartments