There are three articulations within the knee joint complex: Lateral and medialtibiofemoral and patellofemoral joints
Movements can occur along two axes:
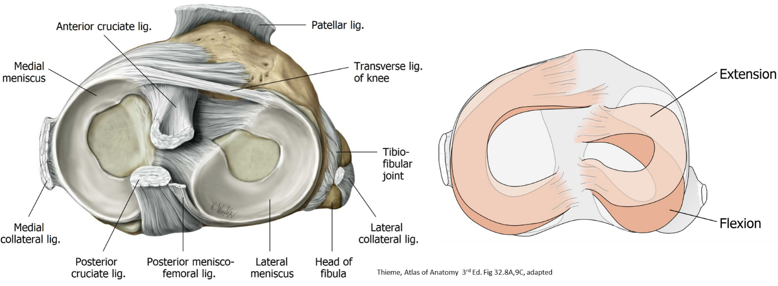
The primary movements are flexion and extension
Because the radii and lengths of the articular surfaces of the femur and tibia differ, there is a small amount of rotation around the long axis of the bones during the terminal phase of extension and initial phase of flexion.
“Screw-home” mechanism
Since the articular surfaces of the femur and tibia are not complimentary, and the size of the femoral condyles are not equal (the articular surface of medial condyle of the femur is larger than that of the lateral condyle), some rotation must occur to achieve maximum congruency of the joint surfaces.
When the knee joint is not weight bearing, as when sitting down and using a leg extension machine in the gym (femur fixed = cannot move), the tibia rotates externally (laterally) on the stable femur as the knee moves from flexion to maximum extension.
When the knee is weight bearing, as is standing up from a squatting position (tibia fixed = cannot move), the femur rotates internally (medially) on the stable tibia as the knee moves from flexion to maximum extension.
Rotation of the bones to achieve full extension places the articular surfaces in maximum congruency, “locking” the knee in its most stable position. This is called the “close-pack” position of the knee joint. The rotation occurring during the last phase of extension is known as the “screw-home” mechanism.
At full extension, the cruciate ligaments and collateral ligaments tighten and become taut.
Unlocking the knee
In the close-pack position, the femur and tibia are “screwed-home” and in their most stable arrangement. Therefore, a force must be applied to the bones to get them out of the close-pack position so that the joint can be flexed. This force is supplied by the action of the popliteus muscle.
When the knee is not weight bearing (femur fixed), the popliteus rotates the tibia internally (medially) on the stable femur as flexion of the joint is initiated.
When the knee is weight bearing (tibia fixed), the popliteus rotates the femur externally (laterally) on the stable tibia as flexion is initiated.
As the knee moves into a flexed position, the joint capsule and ligaments become lax and the articular surfaces of the tibia and femur lose congruency. This “loose-pack” position is when the knee is structurally less stable.
Osteology
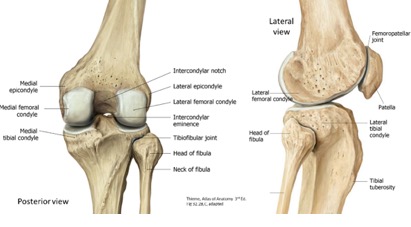
Figure 25.1Distal femur
Femoral condyles
Patellar surface
Intercondylar fossa
Medial and lateral epicondyles
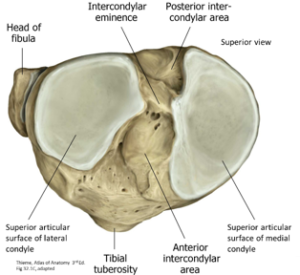
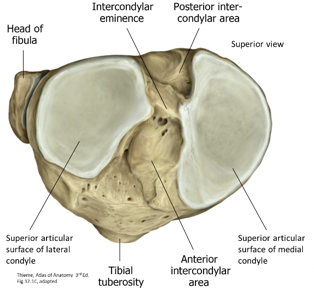
Proximal tibia
Intercondylar eminence
Superior articular surfaces
Medial and lateral condyles
The flat proximal part of the tibia above the condyles, containing the intercondylar eminence and the articular surfaces, is referred to as the tibial plateau. It is an important weight-bearing part of the lower limb
Tibial tuberosity
Figure 25.2Fibula
Head
Patella
Base
Apex
Medial and lateral articular facets
Arthrology
Figure 25.3
Knee alignment with the femur.
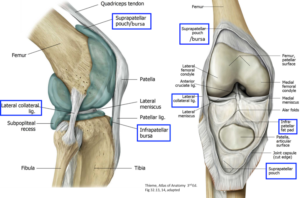
The femur angles from lateral to medial as it meets the tibia at the knee joint (see Figure 25.4). In a frontal view, with a vertical line passing through the center of the knee joint, this angle is about 15 degrees away from the vertical.
Excessive angulation of the femur laterally angles the knee joints inward toward the midline, producing genu valgum (“knock-knee’).
Reduced angulation between femur and tibia gives the appearance that the knee joint is angled outward, away from the midline, a condition called genu varum (“bow-legged”).
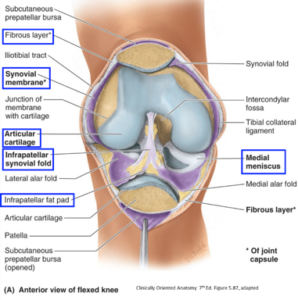
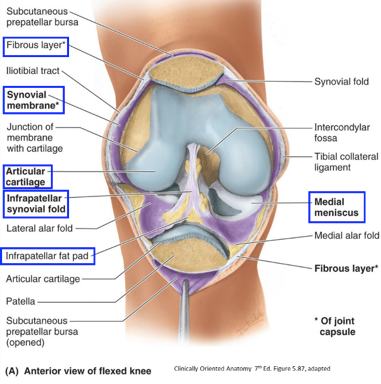
Recall a typical synovial joint: two bones covered by articular cartilage, a synovial membrane, and a fibrous capsule that may be thickened in certain regions to form capsular ligaments . . .
Knee joint: Also has intra-articular ligaments (cruciates), intra-articular menisci, and a redundancy of the synovial membrane (suprapatellar pouch)
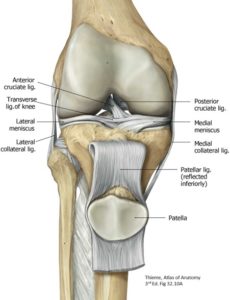
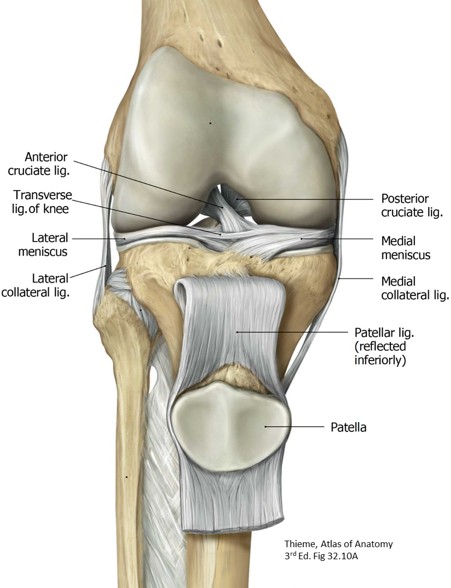
Patellar ligament: Very strong, thick band; is the continuation of the tendon of the quadriceps femoris muscle distal to the patella. It attaches distally to the tibial tuberosity.
Patella: Continuous with fibrous capsule; most easily felt when leg is extended
Osgood-Schlatter Disease: In adolescents during growth spurts: inflammation of epiphysis/growth plate deep to tibial tuberosity from running, jumping, and swift changes in direction (soccer, basketball, volleyball, or ballet)
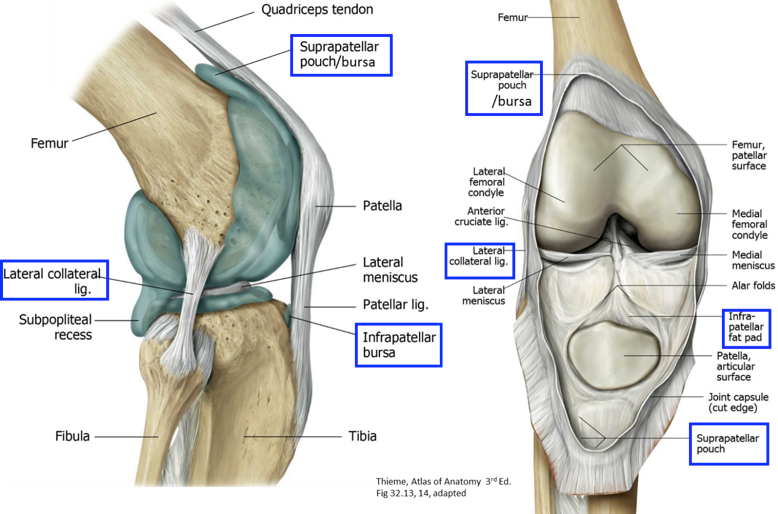
Infrapatellar fat pad: Loose fatty tissue separating synovial membrane from deep surface of patellar ligament
Patellar Reflex: Assesses damage to the femoral nerve; damage to the reflex centers in the spinal cord (L2–4) will affect the patellar reflex
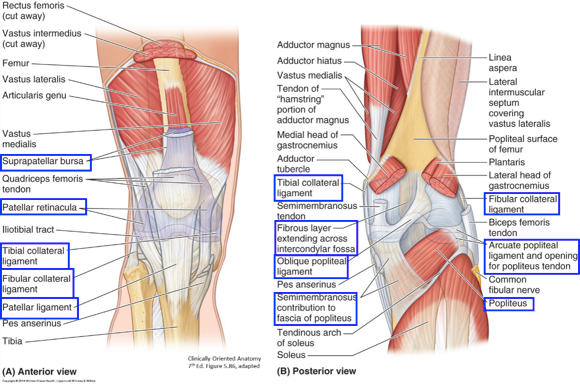
Figure 47.5Patellar retinaculum: Aponeurotic expansions of the quadriceps muscles and their overlying fascia. The retinacula make up the capsule on both sides of the patella and hold the patella in line as the knee is flexed or extended
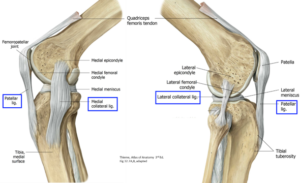
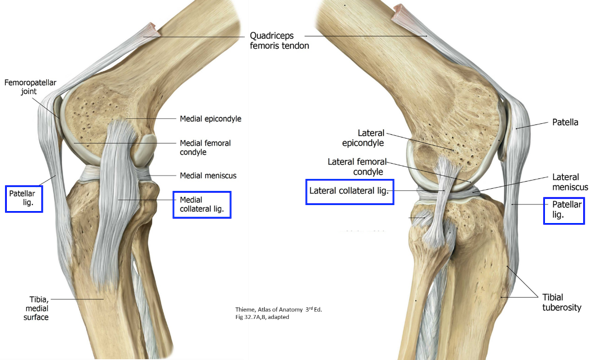
Collateral ligaments
Medial collateral ligament (MCL): a thickening of the medial knee capsule
Proximal attachment: center of medial femoral condyle
Two distal attachments
To the medial meniscus and to the proximal medial tibia posterior to the pes anserinus
Stabilizes medial side of the knee against valgus angulation
A forced abduction of the leg (lateral hit or tackle) at the knee joint (valgus stress) can result in a stretch or tear of the ligament.
Injury to the MCL from a blow to the lateral side of an extended knee can also damage the medial meniscus
Lateral collateral ligament (LCL): rounded band not part of capsule, but lies outside it
Proximal attachment: lateral femoral condyle
Distal attachment: head of the fibula
Stabilizes the lateral side of the knee against varus angulation
Forced adduction of the leg (varus stress) can strain or tear the LCL
When the knee is in extension, additional support for the lateral side is provided by the iliotibial band, the tendon of the biceps femoris, and the popliteus.
Oblique Popliteal Ligament
Broad expansion of tendon of the semimembranosus muscle
Strengthens the fibrous capsule of the knee joint posteriorly
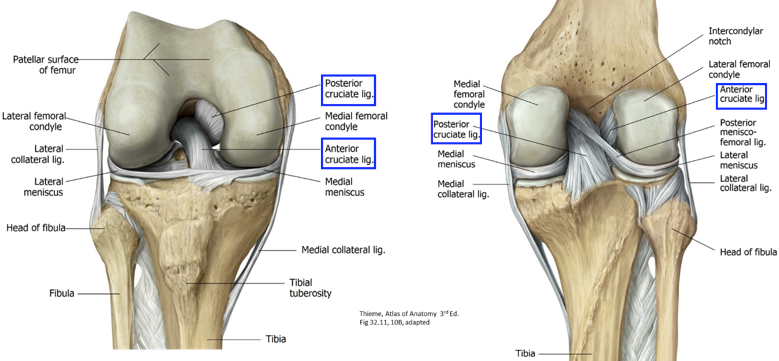
Figure 47.6Cruciate ligaments: Located within intercondylar notch; attached superiorly to the femoral condyles and inferiorly to the tibial plateau. They are so named because they cross one another, like the letter X.
Anterior cruciate ligament (ACL): From the medial side of lateral femoral condyle to anterior tibial plateau
The function of the ACL is to limit anterior displacement of the tibia on the femur, when the femur is fixed.
Most ACL injuries are non-contact: running and cutting sharply in an erect posture; landing from a jump without proper bending of the knees; step off driveway just wrong; basketball
Signs:“Pop”sound;swelling;knee“givingway”
Figure 47.7Posterior cruciate ligament (PCL): From the lateral side of medial femoral condyle to posterior tibial plateau
When femur is fixed, resists posterior displacement of the tibia
Typical injuries: fall on a flexed knee; most common dashboard injury in auto accident; foot planted, hit directly behind or tibia directly in front
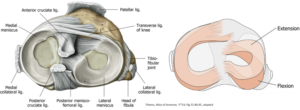
Menisci of the knee
Figure 25.8
2 wedge-shaped semilunar fibrocartilages between the femoral condyles and tibial plateau
Superior surfaces: Have a concavity that fits to the convexity of the femoral condyles
Aids in dissipating the force of the condyles more evenly over the surface of the tibia
Medial meniscus: An open “C” with each end attached to the tibia by an anterior and posterior horn; attached at periphery to the capsule
Attached to the deep surface of the MCL (medial collateral ligament).
Disruption of the MCL can tear the medial meniscus
Meniscus injury can be caused by weight bearing combined with rotary force, squatting, cutting; Signs: gradual effusion, joint line point tenderness, locking or giving away, pain on squatting
Lateral meniscus: More of an “almost O” (or closed “C”) so that its anterior and posterior horns are attached more centrally to the tibial plateau; attached at periphery to the capsule
No attachments to the lateral meniscus
Thick peripheral margins: vascularized by genicular branches of the popliteal artery
Thin unattached edges of the interior of the joint: Avascular
Figure 25.9Suprapatellar pouch
Upward extension of the knee joint cavity between quadriceps tendon and the anterior surface of the supracondylar region of the femur. As part of the joint space, it is lined by synovial membrane and contains synovial fluid. See Figure 25.9.
Provides lubrication of these surfaces during knee motion
Distensionofthesuprapatellarpouchisevidenceof excessive fluid in the joint space
Bursae
Many about the knee; you only need to know a few!
Prepatellar bursa: A subcutaneous bursa between patella and skin. Can become enlarged and inflammed with excessive pressure on the patella/ working on hands and knees, a condition known as “Housemaid’s knee.”
Infrapatellar bursa: Subcutaneous, between tibal tuberosity and skin. Can become enlarged and inflamed by excessive kneeling in an upright position (praying before the anatomy test), known as “Clergyman’s knee” or “Parson’s knee.”
Semimembranosus bursa: A bursa behind the knee between the tendon of the semimembranosus muscle and the medial head of the gastrocnemius. Swelling of this bursa produces a lump in the popliteal fossa known as popliteal cyst or a Baker’s cyst. Since the semimembranous bursa often communicates with the joint cavity of the knee, inflammatory conditions in the knee joint itself can produce the excess fluid that accumulates behind the knee, producing the Baker’s cyst.