Please review the anatomy of the acetabulum, posterior hip bone, sciatic notches, and femur.
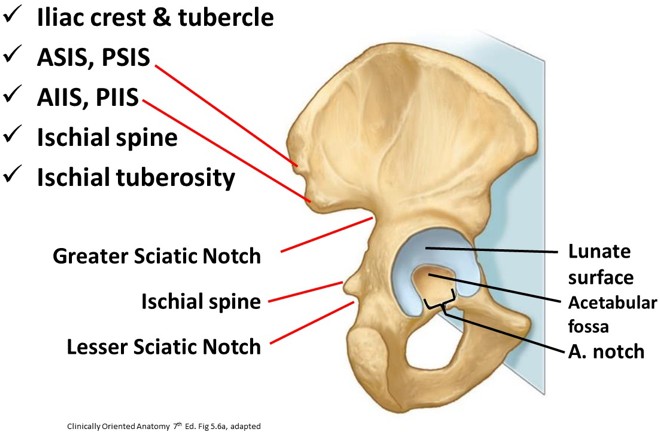
Figure 24.1 Osteology of the os coxae.
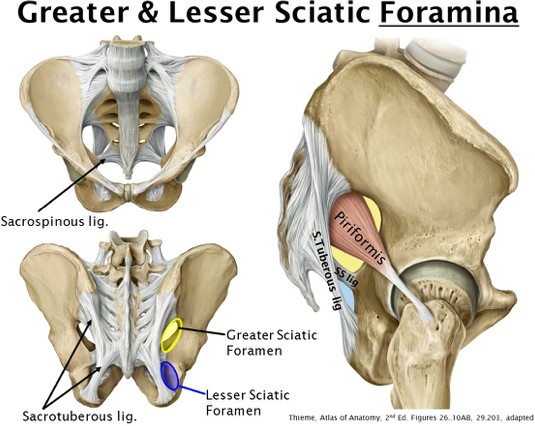
Figure 24.2 Sciatic foramina.
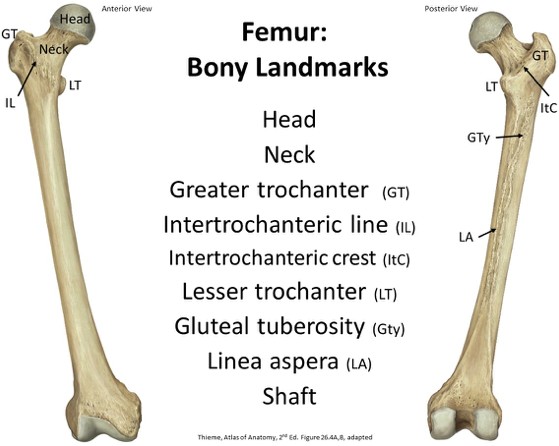
Figure 24.3 Osteology of the femur.
Gluteal region
Physically, the gluteal region is part of the trunk, but functionally, it is clearly part of the limb. The gluteal region includes everything posterior and inferior to the iliac crest and superior to the gluteal folds (the skin crease separating the buttocks from the posterior thigh).
Hip joint (briefly)
Connects pelvic girdle and the lower limb: femoral head articulates with the acetabulum.
Multiaxial ball and socket synovial joint: very strong, primary function:support body weight.
Motions at the hip joint include flexion and extension in the sagittal plane; adduction and abduction in the frontal plane; and internal and external rotation in the horizontal plane.
Muscles of the gluteal region
Study the attachments of the muscles to bones of the gluteal region. One way to begin your study is to group the muscles, either by function or by layer.
Functional grouping
Grouping by layer
Hip extensor: Gluteus maximus
Hip abductors: Gluteus medius, Gluteus minimus (and Tensor Fascia Latae)
Hip external rotators: Piriformis, Gemellus Superior and Inferior, Obturator internus, and Quadratus femoris
We dissect superficial to deep, so it helps to group the muscles this way. The superficial layer includes the Gluteus maximus, G. medius, G. minimus, and tensor fascia latae. The deep layer contains the external rotators of the hip. For full details on attachment, action, and innervation, see the tables at the end of this section of notes.
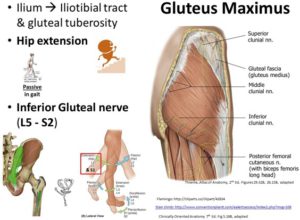
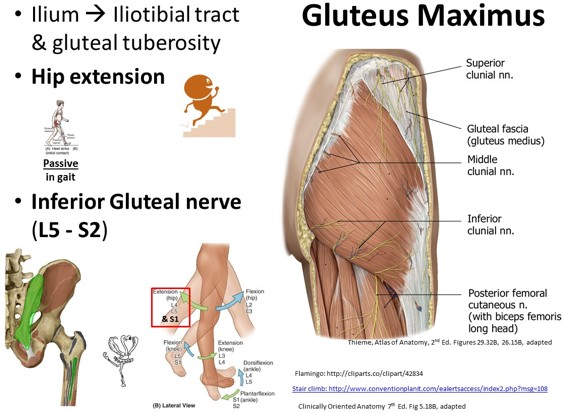
Figure 24.4
Largest muscle and the most superficial
Origin: posterior ilium, to the posterior gluteal line, and the sacrum all the way down to the coccyx and sacrotuberous ligament
Insertion: ~1/4 attaches to gluteal tuberosity of femur, and remaining fibers attach to iliotibial tract
Action: extends the hip, most actively when the hip is already flexed (i.e., going up stairs)
With tensor fascia latae: help stabilize patella laterally when knee extended, via the ilitotibial tract
Nerve: inferior gluteal nerve of the sacral plexus (L5-S2)
Did you know we don’t actually sit on our Gmax? When you flex your hip, it slides superiorly so you are really sitting on skin, fat, and a bursa covering the ischial tuberosity. Ha! So everyone has a ‘bony butt’!!
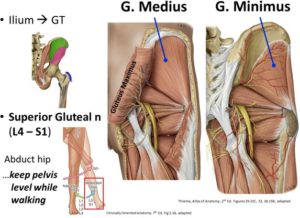
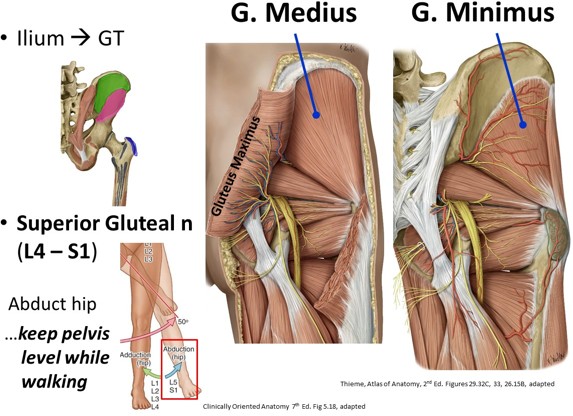
Figure 24.5
O, Gmed: between anterior and posterior gluteal lines of the iliac fossa
O, Gmin: between anterior and inferior gluteal lines of the iliac fossa
I, Both: together to dome of greater trochanter
N: superior gluteal nerve (L4–S1)
A: abduct the hip. These muscles together are the “deltoid of the hip joint.”
Everyday activity: The gluteus medius and minimis are abductors of the thigh, an important motion if you like to ski in the snow or the water. However, their main everyday importance is in walking. With one leg off the ground prior to taking a forward step, the Gmed and Gmin muscles of the planted limb (the limb whose foot is on the ground) contract to keep the unsupported limb (the limb on the opposite side, whose foot is off the ground) from falling down. Without theses muscles, the unsupported hip would drop suddenly each time you take a step forward.
Weakness or paralysis: Hip will tilt toward the unaffected/non- weight bearing side = Trendelenburg sign
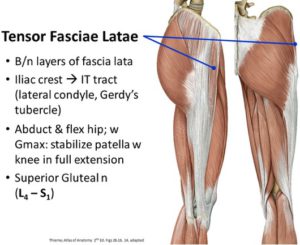
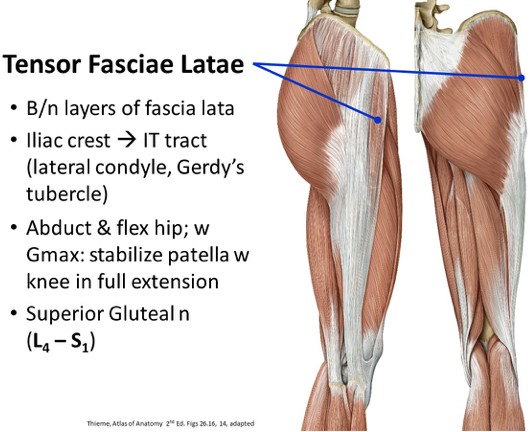
Figure 24.6
Fusiform muscle that is enclosed in the fascia lata
O: ASIS and anterior iliac crest
I: iliotibial tract (which itself attaches to Gerdy’s tubercle on the lateral condyle of the tibia)
N: superior gluteal nerve
A: main action, stabilize the patella when the knee is fully extended
Assists in flexion and abduction of the thigh
Deep muscles of the gluteal region
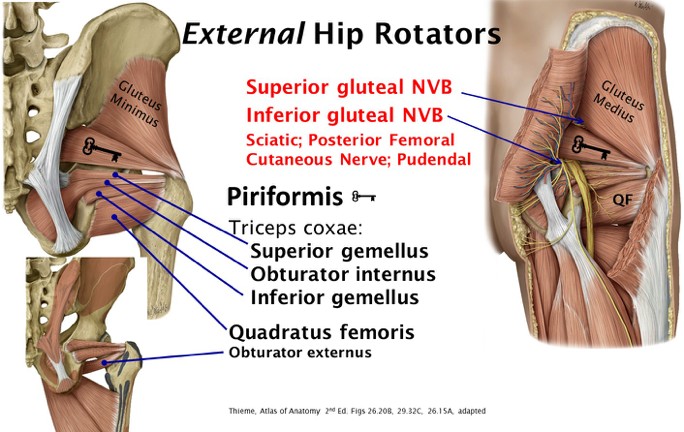
Figure 24.7
Hip external rotators: piriformis, obturator internus, obturator externus, superior and inferior gemelli, and quadratus femoris
Located deep to gluteus maximus
These small muscles also behave like the rotator cuff of the upper limb, by stabilizing the ball (femoral head) within the socket (acetabulum), although this function is much less important in the lower limb, due to the robust stability of the hip joint skeleton and ligaments.
Piriformis: almost fills the greater sciatic foramen, is partly posterior to the hip joint, and attaches to the greater trochanter
“Key to the gluteal region”: neurovasculature structures pass superior to or inferior to it
Obturator internus leaves the pelvis through the lesser sciatic foramen
Gemelli serve as “extrapelvic reinforcements” to the obturator internus
Vessels and nerves of the gluteal region
Superior and inferior gluteal arteries: Arise from the internal iliac arteryin the pelvic cavity and pass through the greater sciatic foramen. Named according to their relationship to the piriformis muscle; see Figure 24.7.
Superior gluteal artery: Travels between Gmed and Gmin
Inferior gluteal artery: Travels superficial to the sciatic nerve
Anastomose around the hip
Superior and Inferior gluteal veins: Tributaries to internal iliac vein, follow same path as the arteries
Clunial nerves are sensory nerves of the buttocks. (L. clunes = buttocks)
Superior and middle clunial nerves: Dorsal rami of spinal nerves
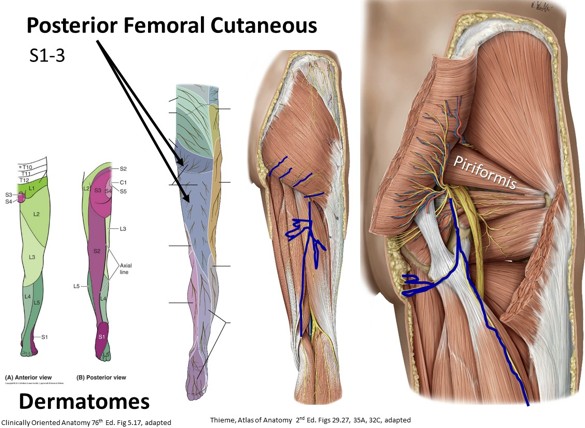
Inferior clunial nerve: A branch of the posterior cutaneous nerve of the thigh
Motor nerves of the gluteal region are from the sacral plexus
Ventral rami of lower part of lumbosacral plexus (L4–S3); exit anteriorsacral foramina and fuse to supply abductors and extensors of the hip and all muscles below the knee. You need to know the names and distribution of the peripheral nerves that emerge from the plexus.
Pass inferior to piriformis EXCEPT the superior gluteal nerve, which courses with the superior gluteal artery to serve Gmin, Gmed, and tensor fasciae latae
Inferior gluteal nerve: Courses with the inferior gluteal artery and serves Gmax
Figure 24.8
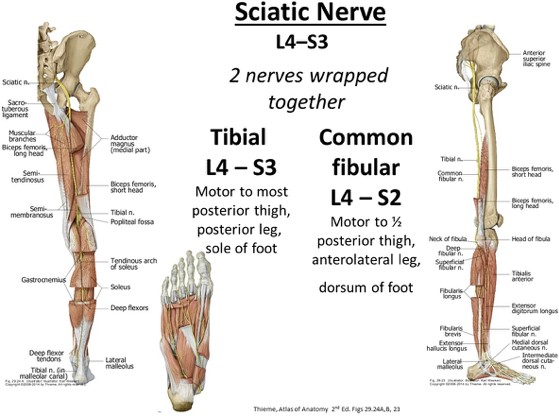
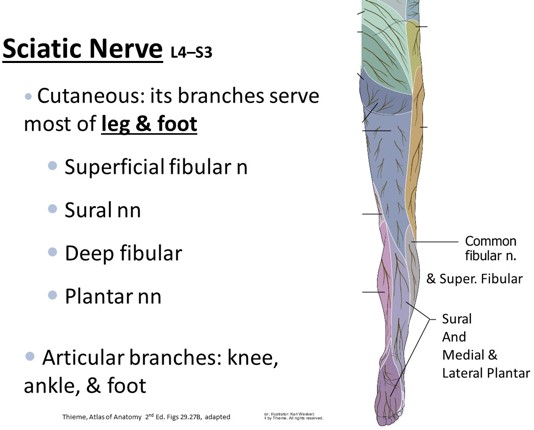
Figure 24.9.Sciatic nerve: Formed at the inferior border of the piriformis, and is the most lateral structure leaving the greater sciatic foramen
Courses midway between the greater trochanter and the ischial tuberosity, then posterior to the obturator internus and quadratus femoris muscles
2 nerves wrapped together: The tibial and common fibular nerves
In posterior thigh: 2 nerves separate and are then no longer called the sciatic nerve
Components of the sciatic nerve serve muscles in the posterior thigh. When they have separated, each nerve will serve their respective muscles and (most) skin of the leg and foot.
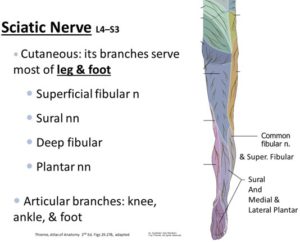
Figure 24.10
Posterior cutaneous nerve of the thigh: Courses just medial to the sciatic nerve and supplies the inferior buttock (via its branches called the inferior clunial nerves), the posterior thigh, the popliteal fossa, and sometimes the proximal posterior leg
Clinical correlation: Intragluteal injections
The ‘glutes’ are thick large muscles with a great volume of absorption through intramuscular veins; just don’t stab the nerves in this area!
Figure 24.11
Retrace the course of the sciatic nerve; recall it is the most lateral “gluteal” nerve, and it doesn’t always exit inferior to the piriformis. Hitting the superior gluteal nerve will cause hip drop/ Trendelenburg sign! The safest site is in the superolateral quadrant of the buttock, from the posterior superior iliac spine to the superior border of the greater trochanter. Locate this site: put your index finger on the anterior superior iliac spine, and your middle finger on the iliac crest.Inject between the two fingers. See Figure 24.3.
Table 24.1 Table of nerves, spinal segments, muscles innervated, and cutaneous distribution
Nerve
Segments
Muscles
Cutaneous
N. to quadratus femoris and Inf. Gemellus Note: Will be difficult to locate on donor
L4, L5, S1
Inferior gemellus, quadratus femoris
N. to obturator internus & Sup. gemellus Note: Will be difficult to locate on donor
L5, S1, S2
Supeiror gemellus, obturator internus
Pudendal
S2–4
Bulbospongiosus. Deep transverse perineal, ischiocavernosus, sphincter urethrae, superficial transverse perineal
Clitoris, Penis
Posterior femoral cutaneous
S1–3
Lower buttock, posterior thigh, & popliteal fossa
N. to piriformis Note: Will be difficult to locate on donor
S1-2
Piriformis
Superior gluteal
L4–S1
Gluteus medius and minimus, Tensor fasciae latae
Inferior gluteal
L5–S2
Gluteus maximus
Sciatic (two parts)
Tibial
L4, 5, S1–3
Semimembranosus, Semitendinosus, Long head Biceps femoris; Posterior leg muscles
Posterolateral leg and foot
Common fibular
L4–S2
Short head of Biceps femoris; Anterior and lateral leg muscles
Anterolateral leg and foot
Gluteal region lymphatics
Lymph follows the superior and inferior gluteal vessels to nodes of the same name, then to the internal, external, and common iliac lymph nodes. Lymph in the superficial tissues drains to the superficial inguinal lymph nodes then into the external iliac lymph nodes.
Posterior thigh
Figure 24.12
“Hamstring” muscles: Primary flexors of the knee and play a shared role in hip extension
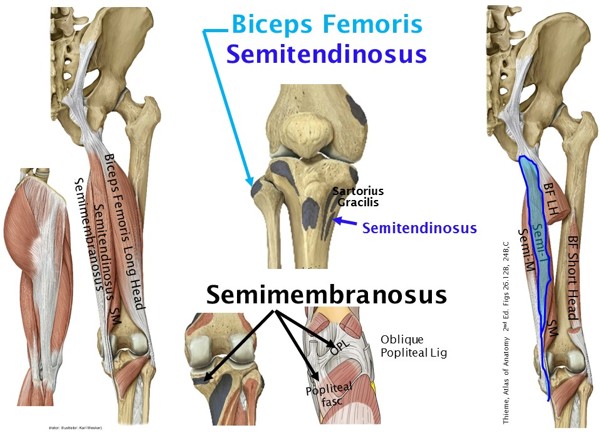
Muscles: Semitendinosus, Semimembranosus, and Biceps Femoris (short head and long head)
O: Common proximal attachment to ischial tuberosity deep to thegluteus maximus
Tendons are visible posterior to the knee and can be made to stand out by flexing the leg against resistance
Span the hip and knee joints, so they extend the thigh and flex the leg.Both actions cannot be performed fully at the same time. Check out the tables for details on attachments, actions, and innervations.
Myotomes: L5, S1
Biceps Femoris
Fusiform muscle has two heads: long and short. Both have separate proximal attachments, and separate innervations, as previously stated.
O: Long head: o ischial tuberosity Short head: linea aspera
I: Both heads fuse to form its rounded distal tendon, which can easily be seen and felt as it passes the knee to insert on the head of the fibula.
N: Long Head: tibial part, sciatic nerve Short Head: common fibular part, sciatic nerve
A: Long Head: Extends thigh at the hip joint; Both heads: flex legat the knee, and laterally rotate the leg when the knee is flexed
Semitendinosus
Half-tendinosus, fusiform with a long, cord-like tendon that begins about 2/3 down the thigh
A: Extends the thigh, flexes the leg and medially rotates the leg when the thigh and leg are flexed. It can extend the trunk when the feet are planted.
N: Tibial part of sciatic nerve
Semimembranosus
Broad muscle is half-membranous and flattened at its proximal attachment. It is located deep to the semitendinosus muscle with has the same actions.
I: Posterior medial condyle of tibia; part that blends with popliteal fascia, and part called oblique popliteal ligament (reinforces intercondylar part of knee joint capsule)
A: Extends the thigh, flexes the leg and medially rotates the leg when the thigh and leg are flexed. It can extend the trunk when the feet are planted.
N: Tibial part of sciatic nerve
Blood supply and cutaneous innervation
The posterior thigh is supplied by perforating branches of the deep artery of the thigh (profunda femoris).
Cutaneous sensation is serve mostly by the posterior femoral cutaneous nerve, and a little by the lateral femoral cutaneous nerve.
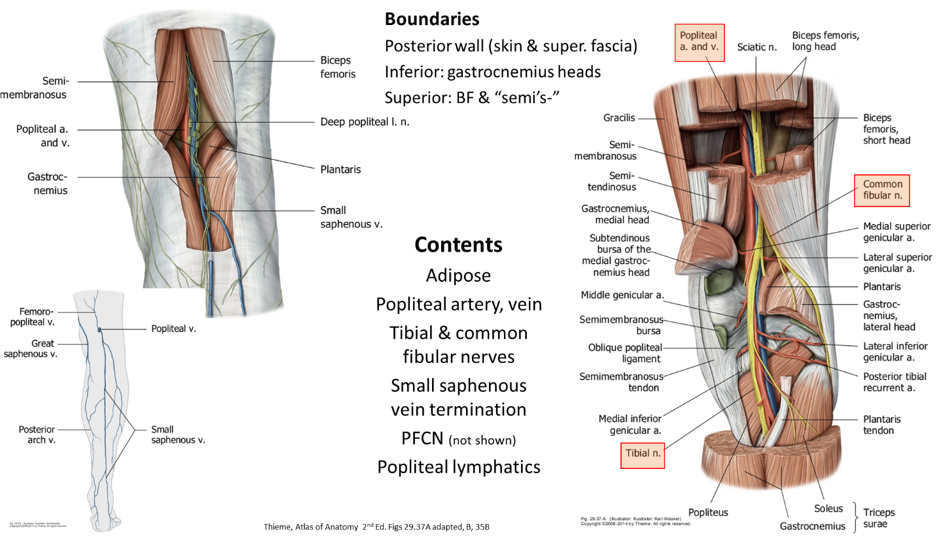
Popliteal fossa
Diamond-shaped region posterior to the knee, and appears hollowed when the knee is flexed
Lies posterior to distal third of femur, knee joint, and proximal part of tibia
Roof (posterior wall): Skin and fascia
Superficial fascia contains fat, small saphenous vein, and cutaneous nerves
Roof: Pierced by posterior femoral cutaneous nerve and by small saphenous vein
Small saphenous vein drains into the popliteal vein
Deep fascia: Forms a strong, dense sheet, which affords a protective covering for the neurovascular structures passing from the thigh to the leg
Floor (anterior wall): Popliteal surface of the femur, oblique popliteal ligament (an expansion of the semimembranosus tendon), and popliteus fascia
Medial border: Semimembranosus and semitendinosus muscles and medial head of gastrocnemius
Lateral border: Biceps femoris muscle and lateral head of gastrocnemius