The internal iliac arteries are the prime sources of blood to pelvic structures. They also supply musculoskeletal structures outside the pelvic cavity (hip and gluteal regions). Arising from the common iliac arteries anterior to the sacro-iliac joints, their branching pattern is highly variable, so it is important to identify branches by tracing them to their destinations. The branches are also somewhat different in the sexes. The internal iliac artery usually divides into anterior and posterior divisions.
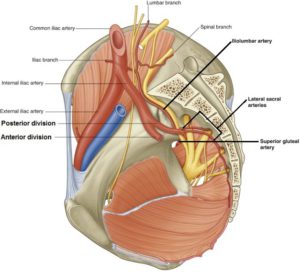
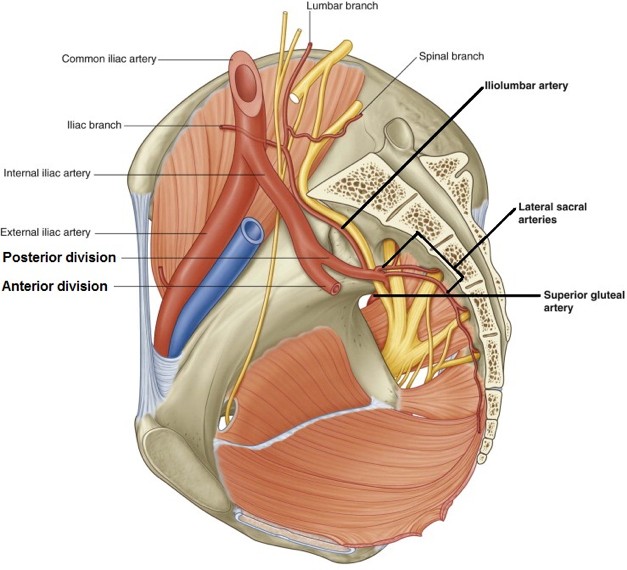
Figure 21.1 Branches from the posterior division. GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.63.Iliolumbar artery: Ascends along the ala of the sacrum and leaves the pelvic cavity to supply the iliacus muscle and become the fifth lumbar artery (a segmental artery to the body wall).
One or two lateral sacral arteries: Send branches into the anteriorsacral formina. They supply the bone of the sacrum and dura in thesacral canal.
Superior gluteal artery: Large artery that leaves the pelvic cavity through the greater sciatic foramen above the piriformis muscle to supply the gluteus medius and minimus muscles.
Note: Most of the branches of the internal iliac arise in front of the greater sciatic foramen and several of them leave the pelvic cavity through it. The piriformis muscle is a good landmark for describing this exodus = the superiorgluteal artery exits above it and the inferior gluteal and internal pudendal arteries pass below.
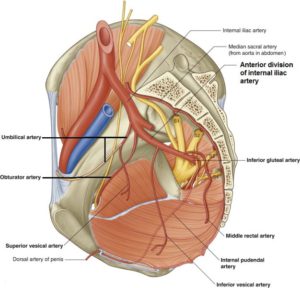
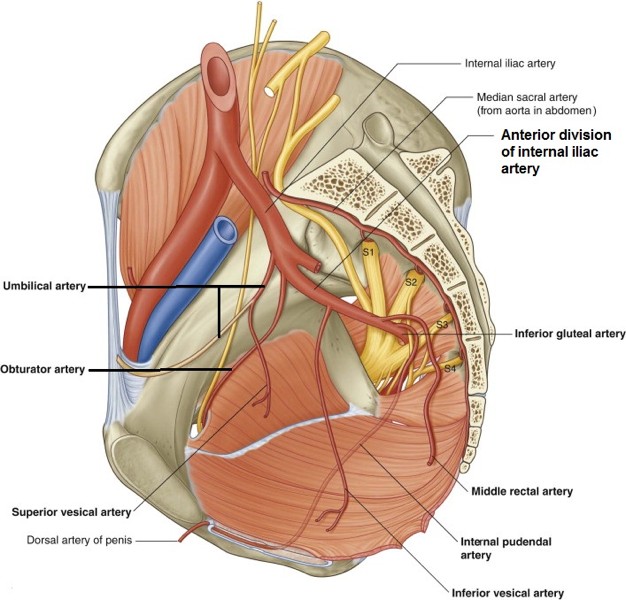
Figure 21.2 Branches from the anterior division of the internal iliac artery in the male. GRAY’ S ANATOMY FOR STUDENTS, FIGURE 5.64.Umbilical artery: Normally the first branch from the anterior division, it passes lateral to the bladder and ascends the internal body wall external to the peritoneum toward the umbilicus. In the fetus it carried deoxygenated blood through the umbilical cord to the placenta. After birth, the extrapelvic part of the artery obliterates to become the fibrous medial umbilical ligament. The proximal intrapelvic part remains patent and carries blood to the bladder.
Superior vesical arteries: Several in number, they branch from thepatent part of the umbilical artery to supply the upper part of the bladder.
In the male, the artery of the ductus deferens is typically a branch ofthe umbilical artery.
Obturator artery: Runs along the pelvic surface of the obturator internus muscle with the obturator nerve. They both leave the pelvic cavity through the obturator canal to supply the medial thigh. In about 25% of cases, the obturator artery arises from the inferior epigastric artery. Surgeons need to know about this variation when performing hernia repair surgeries in this area.
Inferior vesical artery: Some sources claim this artery is only present in the male. It supplies the lower part of the bladder and the prostate.
Uterine artery: In females, it turns medially and heads toward the cervix of the uterus in the cardinal ligament. It passes just above the ureter (“bridge over water”)—an important relationship for surgeons. It supplies the uterus and fallopian tube (anastomosing with the ovarian artery).
Vaginal artery: In females only and highly variable. It may arise from the uterine artery or independently. Supplies the lower part of the bladder and vagina. It is said to replace the inferior vesical artery.
Inferior gluteal artery: Leaves the pelvic cavity through the greater sciatic foramen inferior to the piriformis muscle to supply the gluteus maximus muscle.
Internal pudendal artery: Leaves the pelvic cavity through the greater sciatic foramen, between the piriformis and coccygeus muscles. It loops around the ischial spine and then passes through the lesser sciatic foramen to enter the ischio-anal fossa. As described earlier, it is the main blood supply to the perineum.
Middle rectal artery: May arise from the inferior vesical, vaginal, or internal pudendal arteries. Supplies the rectum just above the pelvic diaphragm and the prostate/vagina. Anastomoses with the superior rectal and inferior anal arteries.
Ovarian arteries: Branch from the abdominal aorta just inferior to the renal arteries. They descend behind the peritoneum on the psoas major muscles and cross the pelvic brim. In the pelvic cavity they run in the suspensory ligament of the ovary (infundibulopelvic ligament) to supply the ovary and fallopian tube.
Superior rectal artery: The continuation of the inferior mesenteric artery. It crosses the pelvic brim within the sigmoid mesocolon. Once in the pelvic cavity, it supplies blood to the rectum and upper anal canal.
Venous drainage
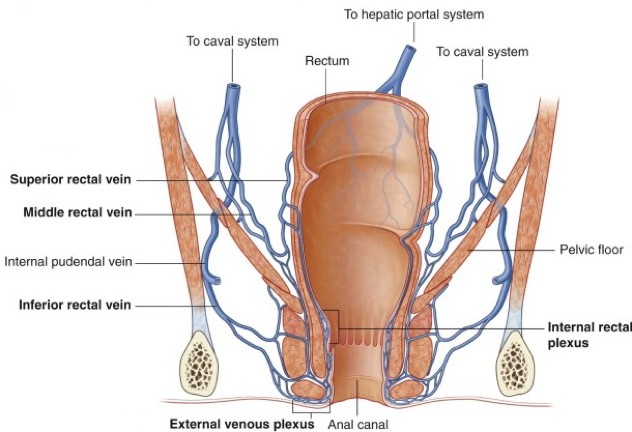
Figure 21.3 Venous drainage of rectum and anal canal. GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.66.
Internal iliac veins
The internal iliac veins are the chief venous drainage routes. They lie posterior to the internal iliac arteries. In general,their tributaries correspond to the branches of the internal iliac artery.
Superior rectal vein
The superior rectal vein is a tributary of the inferior mesenteric vein, so it is part of the portal venous system, whereas blood from the middle and inferior rectal (anal) veins flows into the internal iliac veins and then to the inferior vena cava, so these veins are systemic tributaries.
Most pelvic organs are surrounded by networks of small veins (plexuses) with no valves, located in the organ’s visceral pelvic fascia. These venous plexuses communicate with each other and give rise to the tributaries of the internal iliac veins. The prostatic venous plexus is clinically important since it communicates via the internal iliac vein with the vertebral venous plexuses, providing a route for the metastasis of prostate cancer to bone.
Clinical correlation
The rectum and anal canal have extensive venous connections with each other, forming a clinically important portosystemic anastomosis. As mentioned earlier in the discussion of the anal canal, chronic elevation of intra-abdominal pressure (as in straining during bowel movements) or portal hypertension due to liver obstruction can cause varicosities of veins in the anal canal = hemorrhoids.
Lymphatic drainage of pelvic structures
General rule
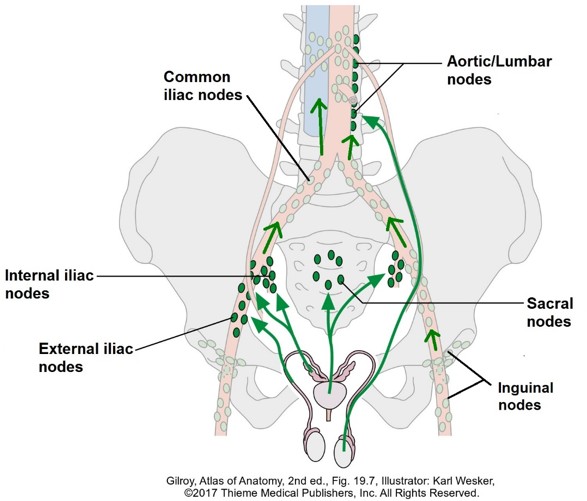
Most lymphatic vessels in the pelvic cavity follow the branches of the internal iliac artery to internal iliac nodes and sacral nodes. From these nodes, lymph flows to common iliac nodes along the pelvic brim, then to clusters of nodes along the vertebral column and abdominal aorta. These nodes are known by different names depending on the source = lumbar, aortic, or retroperitoneal nodes.
There are exceptions to this general rule, which will be dealt with when we discuss the anatomy of the individual pelvic organs. For example, external iliac nodes (situated along the artery of the same name) receive lymph mainly from inguinal nodes, but also receive lymph from a few pelvic organs that are higher up in the pelvic cavity (bladder). Like the internal iliac nodes, the external iliac nodes send lymph to common iliac nodes.
Figure 21.4 Major pelvic lymph nodes (example shown in the male).
Clinical correlation
Cancer from pelvic organs often spreads via lymphatics. Sadly, enlarged pelvic nodes are not palpable due to their deep inaccessible location. Recall that lymph from the testes follows the testicular arteries retrograde to lumbar nodes (as do the ovaries, following the ovarian arteries). Dissection of lumbar nodes in the retroperitoneum is done by surgeons to stage and treat testicular cancer.
Nerves in the pelvic cavity
There are two categories of nerves associated with the pelvic cavity:
1
Somatic nerves derived from the sacral plexus.
2
Autonomic nerves that serve the pelvic viscera.
Sacral plexus
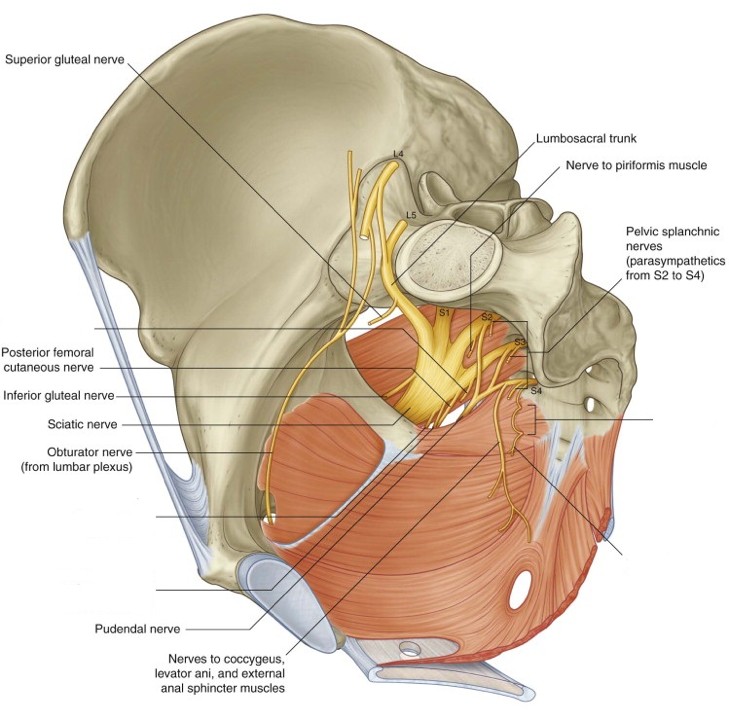
The sacral plexus is the lower portion of the lumbosacral plexus. It is formed by the union of the lumbosacral trunk (ventral rami of L-4 and L-5 spinal nerves) and the ventral rami of the first four sacral spinal nerves. The sacral plexus is formed in the posterior wall of the pelvic cavity on the surface of the piriformis muscle. The branches derived from the sacral plexus are difficult to see in a pelvic dissection because they immediately leave the pelvic cavity through the greater sciatic foramen. In general, the branches supply the buttocks, lower limb, and the perineum.
Table 22.1 summarizes the major branches of the sacral plexus.
Table 22.1 The major branches of the sacral plexus
Nerves
Composition (spinal nerves)
Function
Superior gluteal
L-4 to S-1
Gluteus medius and minimus muscles; Tensor fasciae latae muscle
Inferior gluteal
L-5 to S-2
Gluteus maximus muscle
Sciatic nerve
L-4 to S-3
Muscles in posterior thigh (“hamstrings”); All muscles below the knee (leg and foot).
Posterior cutaneous nerve of the thigh
S-1 to S-3
Skin of posterior thigh
Pudendal nerve
S-2, S-3,and S-4
All muscles in the perineum; Most sensation in the perineum
Note
For now, students should know the spinal nerves that give rise to the pudendal nerve (S-2, S-3, and S-4). The other nerves in Table 22.1 will be covered in more depth later when we tackle the lower limb.
Figure 21.5 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.59.
The obturator nerve, derived from the lumbar plexus (L-2 to L-4 spinal nerves), traverses the lateral pelvic wall on its way to the obturator canal and the medial thigh. It is just passin’ through.
Autonomic innervation of pelvic viscera
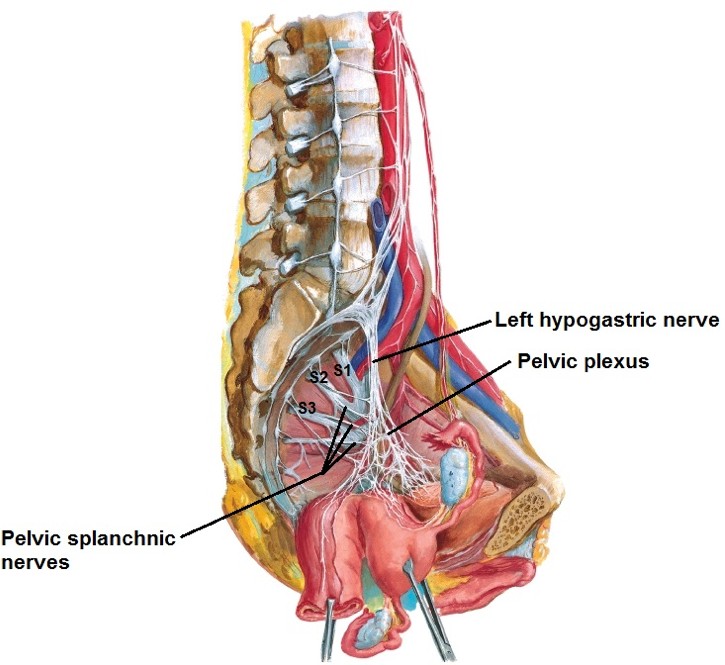
Figure 21.6 NETTER, ATLAS OF HUMAN ANATOMY, PLATE 390.
All pelvic organs presumably receive both sympathetic and parasympathetic fibers (although in some cases their exact function is unknown) and visceral afferent fibers. Blood vessels in the pelvis only receive sympathetic innervation.
The hubs of autonomic nerves in the pelvis are the left and right pelvic plexuses, also called the inferior hypogastric plexuses. These are located below the peritoneum on the lateral pelvic walls, between the rectum and internal iliac artery. Like the cardiac plexus in the thorax and aortic plexus in the abdomen, the pelvic plexuses contains a mix ofsympathetic, parasympathetic, and visceral afferent nerve fibers. These fibers are routed to their target organs along the branches of the internal iliac artery—these tufts of nerve fibers are given specific names associated with the organs they innervate (e.g., vesical plexus, uterovaginal plexus).
The main sources are the left and right hypogastric nerves. These descend from the aortic plexus in the abdomen along the surface of the sacrum on either side of the rectum. The hypogastric nerves probably contain both pre- and postganglionic sympathetic fibers, derived from the lower thoracic and upper lumbar spinal cord. There are scattered prevertebral ganglia in the pelvic plexus. Other sympathetic fibers reach the pelvic plexus via sacral splanchnic nerves from the sacral sympathetic trunk.
Pelvic splanchnic nerves, branches of the ventral rami of spinal nerves S-2, S-3, and S-4 transmit preganglionic parasympathetic fibers to the pelvic plexuses. The cell bodies of these fibers are in the lateral gray horns in S-2 to S-4 spinal cord segments. They synapse on postganglionic neurons in intramural ganglia in the walls of pelvic organs.
Conscious sensations (pain) from pelvic organs are poorly localized. In general, the routes taken are different for organs at the “pelvic pain line” and for those below it (refer back to the notes earlier in the course for the Autonomic Nervous System).
Pelvic viscera at the pelvic pain line (touching the peritoneum): Visceral afferents follow sympathetic routes back to the lower thoracic and upper lumbar spinal cord levels. Cells bodies of these sensory neurons are in the corresponding dorsal root ganglia.
Subperitoneal pelvic viscera (below the pelvic pain line): Visceral afferents follow pelvic splanchnic nerves (parasympathetic) to spinal cord segments S-2 to S-4. Cells bodies are in the corresponding dorsal root ganglia.
Autonomic innervation will be covered with the anatomy of each pelvic organ.