The abdominal esophagus extends ~3cm from the esophageal hiatus of the diaphragm, at about T10. Where it passes through the esophageal hiatus, it can become constricted and cause dysphagia (difficulty in swallowing).
Can vary a lot in people of different body types. In the supine position, it commonly lies in the RUQ and LUQ (or epigastric, umbilical, and left hypochondrium regions). When erect, the stomach moves inferiorly. For some, a very full stomach can extend into the pelvis!
Relationships with other organs:
-
- Anteriorly: Diaphragm, left lobe of liver, AAW
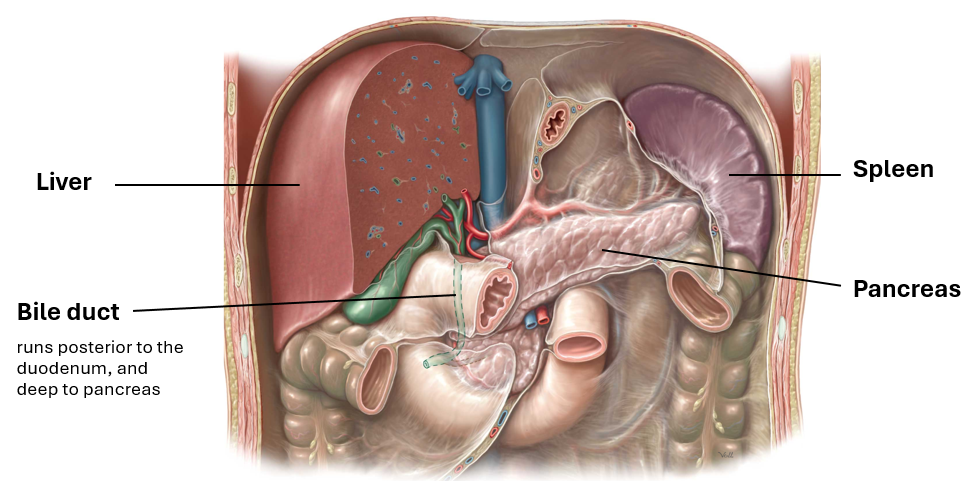
- Posteriorly: Omental bursa, pancreas, spleen, left kidney, and left suprarenal gland
- Inferolaterally: Transverse colon
Parts:
-
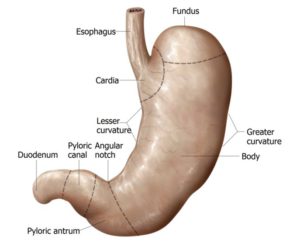
- Cardia: A narrow ring around the esophageal opening
- No sphincter, but has a physiological “cardiac orifice”: Thick muscular wall that can be tightly closed to prevent stomach reflux
- Fundus: Dome of the stomach
- Can be dilated by gas, fluid, food, or any combination; can be seen in a
radiograph
- Can be dilated by gas, fluid, food, or any combination; can be seen in a
- Body: Most of the stomach, between fundus and pyloric antrum; mechanical digestion
- Pylorus: Outflow portion that regulates the passage of food from stomach into duodenum
- Lies at the level of the transpyloric plane; in an erect patient the location varies from L2 thru L4
- Cardia: A narrow ring around the esophageal opening
Two curvatures:
-
- Lesser curvature: Short concave right border of the stomach
- Attachment site of lesser omentum
- Greater curvature: Long convex left border of the stomach
- Greater omentum is suspended from this curvature
- Lesser curvature: Short concave right border of the stomach
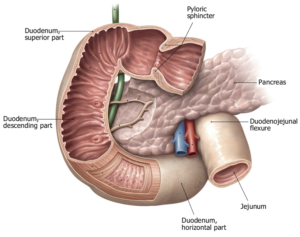
The duodenum leaves the pylorus of the stomach, and is the first section of the small intestine. It has 2 different embryological origins (foregut and midgut) and so has split vascular and neural supply (discussed later).
-
- Begins at the pylorus on the right, its four parts encircle the head of the pancreas, and ends at the duodenojejunal flexure/junction on the left side at ~L2, 2-3 cm to the left of the midline.
- Mostly retroperitoneal
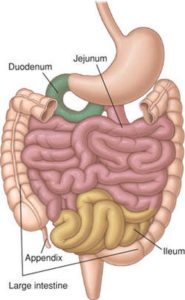
Together: 6–7 m long, with the jejunum being 2/5 of the length
-
- Jejunum: Mostly located in the LUQ (left upper quadrant)
- Ileum: Mostly located in the LRQ (lower right quadrant) at the ileocecal junction.
- Thinner walls, is paler pink, and has more fat in its mesentery (“creeps” onto the tube)
Both contain the same permanent circular mucosal folds, though they are abundant in the jejunum and become fewer until absent at the end of the ileum.
Peristalsis is not forceful in the jejunum and ileum unless an obstruction is present.
Main function: Water absorption
-
- Most reabsorption of water occurs in the ascending colon. Feces (stools) are formed in the descending and sigmoid colon and accumulate in the rectum before defecation
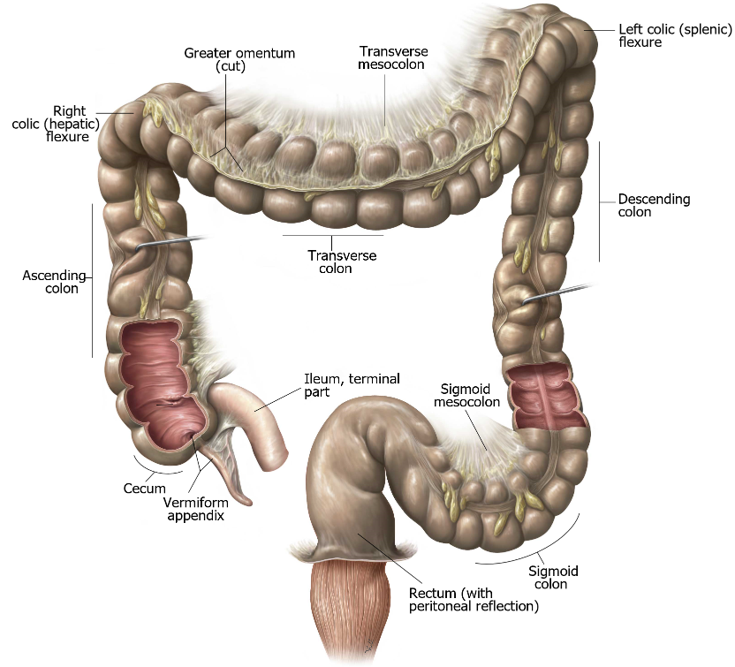
Parts:
-
- Cecum: Lies in the right iliac fossa in the LRQ, inferior to the ileocecal junction, within 2.5cm of the inguinal ligament
- Appendix: Blind diverticulum containing masses of lymphoid tissue, on the posteromedial side of the cecum, usually tucked into the retrocecal pouch
- Ascending colon: Begins at the cecum, and ends at the right colic flexure
- Secondarily retroperitoneal
- Right paracolic gutter lies between its lateral aspect and the abdominal wall
- Transverse colon: Most mobile of the large intestine and extends from right to left colic flexures.
- Variable position: It’s not uncommon for it to hang to the level of the umbilicus (L3)
- Descending colon: Passes anterior to the lateral border of the left kidney
- Secondarily retroperitoneal
- Forms left paracolic gutter
- Sigmoid colon: S-shaped loop of variable length extending from the iliac fossa to the S2 vertebra (in the true pelvis)
- Intraperitoneal: Connected via sigmoid mesocolon
- Rectum and anal canal: The rectum is fixed, and is continuous with the sigmoid colon at S3; the rest will be discussed in the pelvis section
Arteries to all the organs in the abdomen are derived from the abdominal aorta. This is the portion of the descending aorta inferior to the diaphragm. After entering the abdominopelvic cavity via the aortic hiatus in the diaphragm, the abdominal aorta descends anterior to the vertebral column, behind the peritoneum (= retroperitoneal). The abdominal aorta terminates at the level of L-4 vertebra where it bifurcates into left and right common iliac arteries.
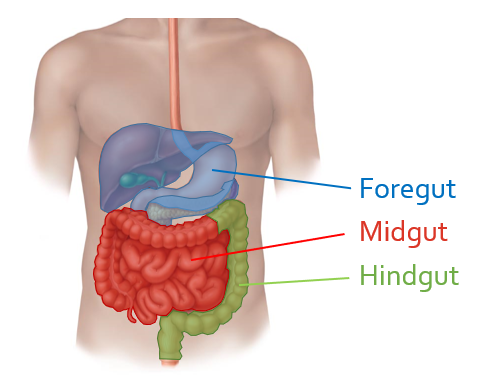
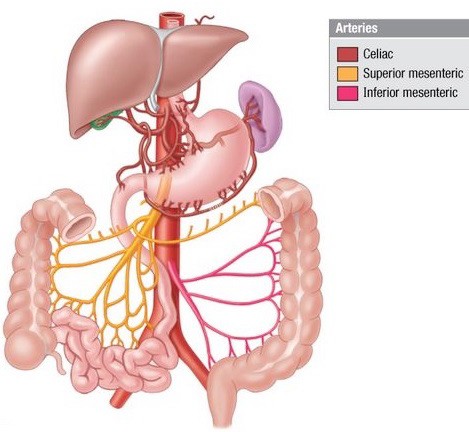
Three unpaired arteries arise from the ventral side of the abdominal aorta—these supply the digestive organs derived from the embryonic foregut, midgut and hindgut.

- The left gastric artery curls on to the left side of the lesser curvature of the stomach—it passes along the lesser curvature within the lesser omentum, meeting up and anastomosing with the right gastric artery.
- The splenic artery, highly tortuous (twisty), passes to the left along the upper border of the pancreas, behind the peritoneum. It reaches the hilum of the spleen within the splenorenal ligament. It gives off short gastric arteries to the stomach (within the gastrosplenic ligament) and the left gastro-omental artery which passes along the greater curvature of the stomach, within the gastrocolic ligament, where it anastomoses with the right gastro-omental artery.
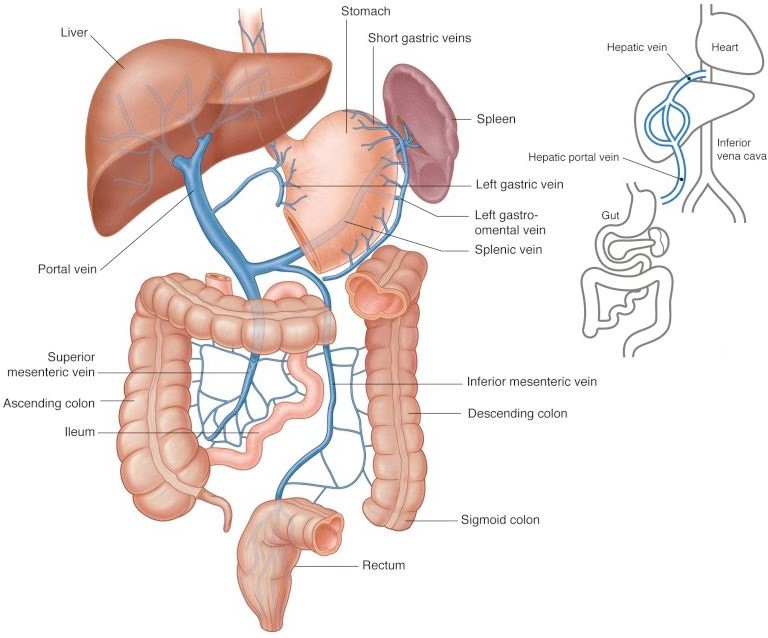
Venous drainage of digestive organs, as well as the spleen, is via the portal vein. The portal vein is formed posterior to the pancreas by the union of the splenic vein and superior mesenteric vein. The inferior mesenteric vein typically is a tributary of the splenic vein. The superior and inferior mesenteric veins drain midgut and hindgut organs, respectively. The splenic vein drains the spleen and parts of the stomach and pancreas. There is no celiac vein. The veins that correspond to arterial branches of the celiac trunk drain directly into the portal vein.
Blood from the portal vein enters the liver for processing, where it percolates through hepatic sinusoids within the liver. From here, venous blood drains into the inferior vena cava via two or three hepatic veins. These enter the IVC just below the diaphragm.
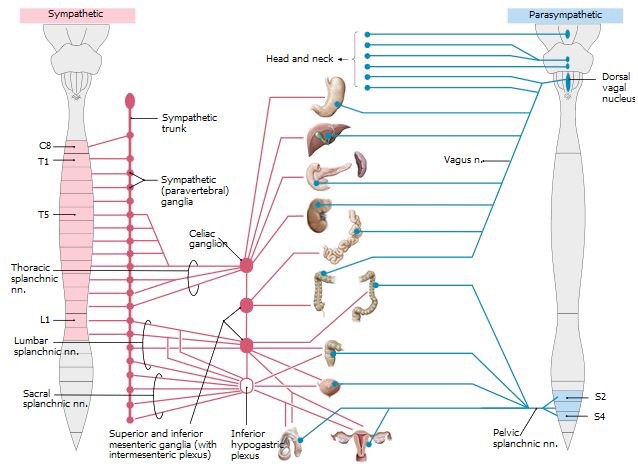
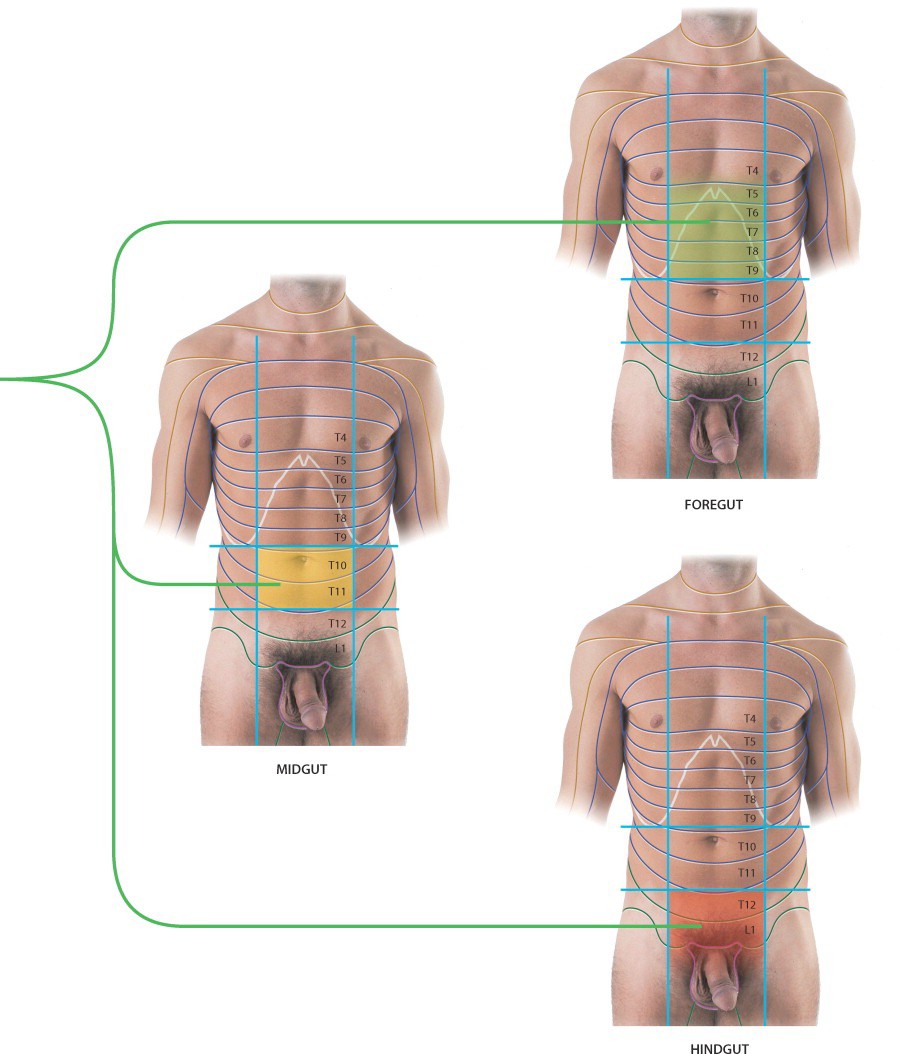
Recall from discussions in Principles of the Autonomic Nerve System (ANS) that visceral afferent fibers carrying pain from internal organs travel along sympathetic innervation routes in a reverse direction (ascend along splanchnic nerves to sympathetic chain ganglia, then pass through white rami communicantes to spinal nerves). Cell bodies of these sensory neurons are in the dorsal root ganglia of spinal nerves. Their central processes enter the dorsal side of the spinal cord through dorsal roots and synapse within the spinal cord on interneurons in the dorsal horns of grey matter.
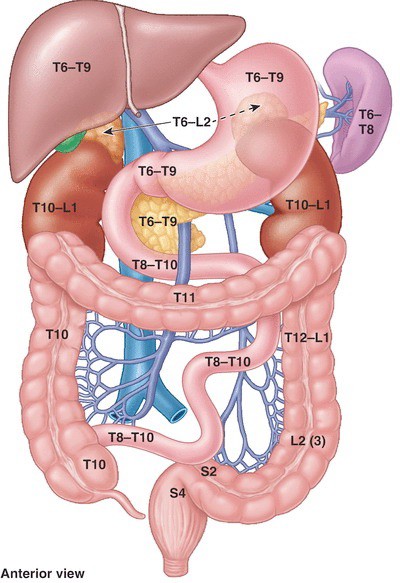
Visceral afferents from different parts of the gut enter the spinal cord at different levels. Visceral afferents from the foregut enter the spinal cord at T-5 to T-9 spinal cord levels. Those from the midgut enter at T-8 to T-12 and those from the hindgut enter L-1 and L-2 cord segments.
Keep in mind that somatic sensory neurons from the skin also enter the spinal cord through dorsal roots and have their cell bodies in the same dorsal root ganglia as do visceral afferent neurons. Once in the spinal cord, visceral afferent and somatic afferent pathways ascend to the brain, using the same pools of interneurons. Pain from an internal organ therefore may be interpreted by the brain as coming from skin dermatomes. This is the concept of “referred pain”: pain originating from an internal organ manifesting as a dull ache in the body wall. Pain referred from the three parts of the gut tube have characteristic regions of the body wall (dermatomes) where they are perceived: