The radius and ulna articulate with the humerus at the elbow joint. It is a uni-axial hinge joint, allowing flexion and extension. It has two articulations:
1. Humero-radial articulation
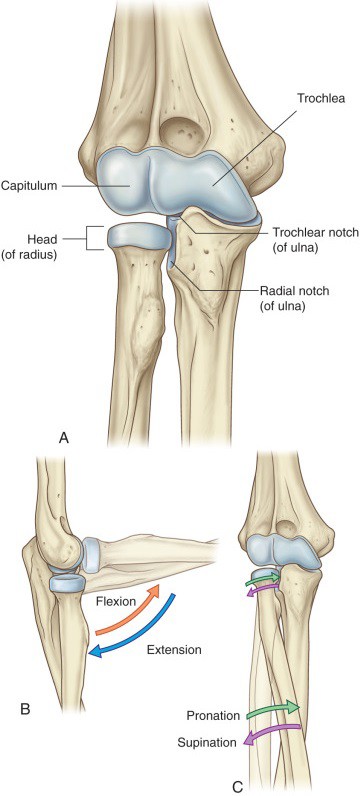
The humero-radial articulation is between the recessed superior surface of the radial head and the capitulum of the humerus. You will often hear clinicians call this the radiocapitellar joint.
2. Humero-ulnar articulation
The humero-ulnar articulation is between the trochlea of the ulna and trochlear notch of the humerus.
3. Proximal radio-ulnar joint
A third articulation is structurally within the joint capsule of the elbow: the proximal radio-ulnar joint. However, it functions separately as a uni-axial pivot joint, being involved in rotation of the radius around the ulna during the movements of supinator and pronation. This occurs when the disc-shaped radial head spins within the radial notch of the proximal ulna.
Figure 10.29 Bones and movements of the elbow complex. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.71.
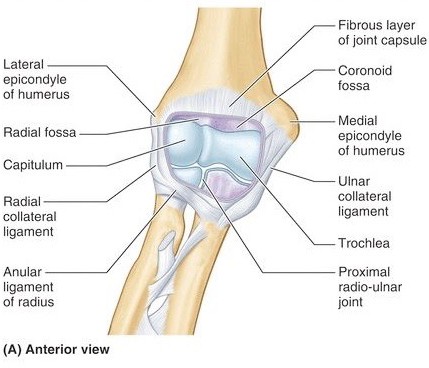
The elbow joint has typical features of a synovial joint. The articulating bony surfaces are covered with hyaline cartilage. The articular capsule of the elbow encloses all the articulating bony surfaces and their cartilages. The humero-radial, humero-ulnar, and proximal radio-ulnar articulations are all enclosed in a single joint capsule. A synovial membrane lines the inside of the joint capsule and the bony surfaces within the joint capsule that are not lined by cartilage.
Figure 10.30 The elbow and proximal radio-ulnar joints are enclosed by a single joint capsule. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, 8TH ED., FIG. 3.97.
Ligaments of the elbow joint
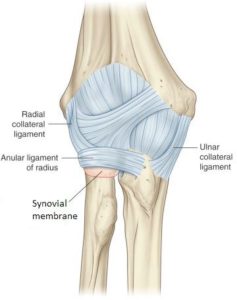
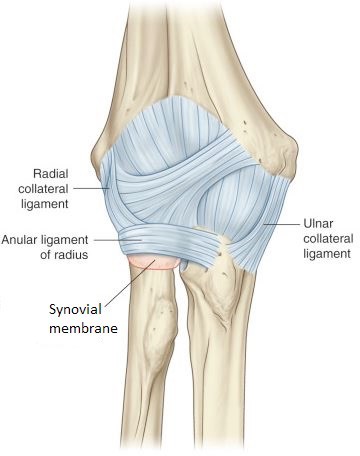
Ligaments reinforce the elbow and proximal radio-ulnar joints. These are capsular ligaments—thickenings of the fibrous layer of the joint capsule. As a rule, hinge joints in the limbs have stout collateral ligaments that reinforce the medial and lateral sides, and this is true of the elbow joint.
The radial collateral ligament is on the lateral side of the elbow. It attaches above to the lateral epicondyle of the humerus and below to the radial head, where it blends with the annular ligament (discussed below).
The radial collateral ligament resists stress on the elbow due to a varus movement of the distal forearm. Varus is a term used to describe inward (medial) angulation of a bone or segment of a limb. A varus force on the elbow results when the distal forearm is angled inward (medially). This movement transmits strain to the ligament on the lateral side (outside) of the elbow = the radial collateral.
The ulnar collateral ligament is on the medial side. It is triangular, attaching above to the medial epicondyle of the humerus and below to both the olecranon and coronoid processes of the ulna.
The ulnar collateral ligament resists stress on the elbow due to a valgus movement of the distal forearm. Valgus is a term used to describe outward (lateral) angulation of a bone or segment of a limb. A valgus force on the elbow results when the distal forearm is angled outward (laterally). This movement transmits strain to the ligament on the medial side (inside) of the elbow = the ulnar collateral.
Conley's clues
Lateral angulation of the distal part of a bone or limb segment is a vaLgus angulation. Remember that the letter “L” in valgus means Lateral.
Figure 10.31 DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.73.
The annular ligament is a ring-shaped fibrous band that attaches to the edges of the radial notch of the ulna and encircles (but does not attach to) the head of the radius. Its job is to support the head of the radius and maintain its location adjacent to the capitulum and ulna, so that the elbow and proximal radio-ulnar joints, respectively, can function properly.
Clinical correlation: Elbow ligament injuries
The radial collateral ligament (RCL) resists excessive varus stress. RCL tears are associated with acute injuries such as fractures or in patients with advanced cases of tennis elbow with tears of the common extensor tendon. They are usually not due to chronic (repetitive) stress, as is the case for the ulnar collateral ligament.
The ulnar collateral ligament (UCL) resists excessive valgus stress. The most common cause of UCL injury is chronic microtrauma from repetitive valgus stress. This is often seen in athletes who participate in overhead throwing events (baseball, javelin throwing, volleyball, to name a few). Surgery to reconstruct a torn UCL involves replacing it with a tendon harvested from somewhere else in the body (hamstring tendon for example). This is popularly known as a “Tommy John” procedure, named after the major league baseball pitcher who was the first to have it done in 1974.
Ossification of the radial head is not completed until about age five. Prior to this, the radial head is smaller and does not fit snuggly within the collar of the annular ligament. A violent tug along the long axis of a child’s limb could cause the radial head to slide distally within the loose-fitting annular ligament and become displaced from the capitulum (radial head subluxation). Because this injury is classically caused by a caregiver’s yank to a young child’s limb, it is known as “Nursemaid’s elbow.” Typically occurring in kids ages 1–5, a patient will come to the clinic refusing to use the affected limb, with the elbow slightly flexed and forearm pronated. There are several techniques used to reduce the subluxation.
One method involves supinating the affected forearm and flexing the elbow, while applying slight traction to the arm. A palpable click will indicate success in reducing the subluxed (partially dislocated) radial head. To safely lift a child, grasp them under their arms, not by their hands!
Figure 10.32 Nursemaid’s elbow.
The radio-ulnar joints
Both proximal and distal ends of the radius and ulna are joined to one another by pivot joints. These allow the radius to move around the ulna to produce supination and pronation.
Proximal radio-ulnar joint
This has been described previously, so we will summarize here. The bones involved are the head of the radius and the radial notch of the ulna. The radial head spins within a circular sleeve formed by the notch in the ulna and the annular ligament. The joint capsule communicates with the elbow joint = the elbow and proximal radio-ulnar joints share the same joint capsule.
Distal radio-ulnar joint
The articulating bones are the round head of the ulna and the ulnar notch on the medial side of the distal radius. Although a fibrous joint capsule joins the articulating bony parts, the main stabilizing structure of the joint is the articular disc of the distal radio-ulnar joint, made of fibrocartilage, that joins the ulnar styloid process to the distal radius. During supination and pronation, the articular disc twists and moves with the radius. The disc separates the joint cavities of the distal radio-ulnar and wrist (radiocarpal) joints. As such, the articular disc of the distal radio-ulnar joint is one of the articular surfaces involved in the wrist joint.
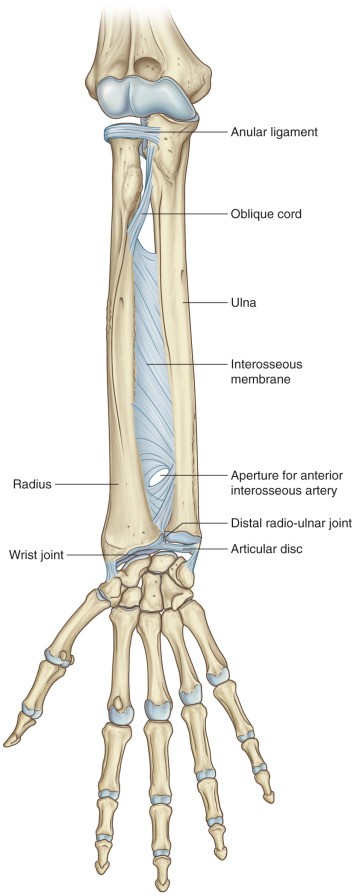
Figure 10.33 Two radio-ulnar joints and an interosseous membrane bind the radius and ulna to one another. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.82.