The arm is the proximal segment of the free upper limb. The organization of the arm is simple: two muscle compartments (anterior and posterior) separated by a single bone (humerus). Let’s begin with the bone and then delve into the compartments, describing their muscles, nerves, and vessels.
The proximal humerus was described in the Shoulder Region because of its importance in shoulder function.
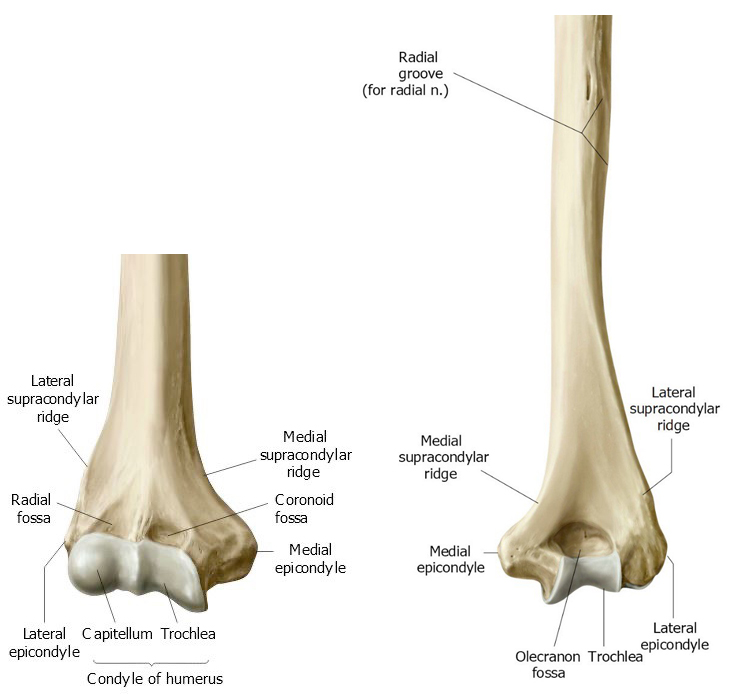
As a typical long bone, the humerus has expanded proximal and distal portions (with specialized protuberances for muscle and ligament attachments) connected by a shaft (body). The shaft is cylindrical in cross section and contains a marrow cavity. Proximally, below the greater and lesser tubercles (The Shoulder Region), the shaft is expanded to form the surgical neck, named because it is a common site of fractures, especially in older patients. A shallow groove spirals around the posterior side of the midshaft of the humerus. This is the called the radial groove since it contains the radial nerve.
Distally, the shaft expands along its medial and lateral borders, forming the medial and lateral supracondylar ridges. These flare outward like groovy bell bottom pants and end as medial and lateral epicondyles, which are easily palpable through the skin and serve as important sites for muscle attachments. The wide distal part of the humerus between the epicondyles is called the condyle (Latin = knuckle). Subparts of the condyle figure prominently in elbow joint construction. Laterally, on the anterior side of the condyle is a round prominence resembling a marble = the capitulum (from Latin caput = head). Clinicians often call this structure the capitellum, which is an equivalent name. Medially is an oblong elevation resembling a spool of thread, visible on both sides of the condyle, called the trochlea (Latin = pulley, because the ulna spins around it). Above the trochlea on the anterior side is the coronoid fossa, where the coronoid process of the ulna slides when the elbow is flexed. Above the trochlea posteriorly is the olecranon fossa, where the olecranon of the ulna fits when the elbow is extended.
Clinical correlation
Supracondylar humeral fractures are common traumatic pediatric fractures. Most often seen in 5- to 7-year-olds, they usually result from a fall on an outstretched hand (FOOSH), with elbow and wrist extended. These occur in this age range since the bone in the distal humerus undergoes extensive childhood remodeling and is thinner than in other regions of the bone.
Figure 10.2 CASE COURTESY OF ASSOC PROF FRANK GAILLARD, RADIOPAEDIA.ORG, RID: 10342.
The ossification process in the distal humerus is complex, involving multiple sites of ossification that occur at different ages. The capitellum usually ossifies first, followed by the medial epicondyle, trochlea, and lateral epicondyle. Fusion of these parts with each other and with the shaft is not completed until adolescence.
Fasciae of arm
The superficial fascia of the arm is typical, containing adipose tissue and cutaneous nerves and vessels. Of note are two large veins that course within the superficial fascia along the pre- and postaxial borders of the arm, the cephalic and basilic veins, respectively. Deep fascia of the arm (brachial fascia), like that of the entire upper limb, forms a snug-fitting glove around the muscles. Cutaneous nerves and vessels penetrate the deep fascia. The anterior and posterior compartments of the arm are defined by the deep fascia, medial and lateral intermuscular septa (inward extensions of the deep fascia—see Introduction the the Limbs), and humerus. Compartments are occupied by muscles, nerves, and vessels.
Anterior compartment of arm
Muscles
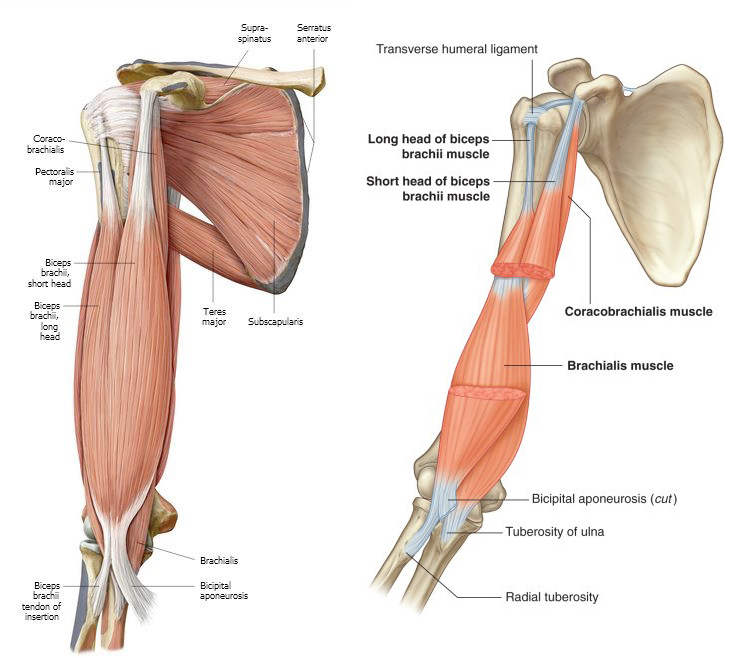
Figure 10.3 (left) Muscles of anterior arm; superficial dissection. GILROY, ATLAS OF ANATOMY, 3RD ED. FIG. 25.19A. (right) Muscles of anterior arm; deep dissection. DRAKE, GRAY’ S ANATOMY FOR STUDENTS, 4TH ED.FIG. 7.64.
Coracobrachialis
Biceps brachii
Brachialis
Its attachments are in its name: Origin = coracoid process of scapula; Insertion = midshaft of humerus. Not a prime mover—it assists other muscles in flexing and adducting the arm at the glenohumeral joint. Assists the rotator cuff muscles in preventing humeral head dislocation.
This sexy muscle gets all the attention, producing the “gun show” in the arm when a fist is made, and elbow flexed.
Attachments: The name implies it has “two heads,” which it does (long and short), and two proximal attachments.
The long head of biceps has a long tendon that originates from the supraglenoid tubercle of the scapula. The first part of the tendon passes through the cavity of the glenohumeral joint (odd),where it is covered with synovial membrane. After leaving the joint, the tendon of the long head slides within the intertubercular sulcus (bicipital groove), between the greater and lesser tubercles of the humerus. A ligament connecting the two tubercles converts the groove into a tunnel for the tendon.
The short head of the biceps arises from the coracoid process of the scapula.
Each of the biceps tendons attaches to a muscle belly. The two bellies fuse at the midpoint of the humeral shaft.
The biceps also has two distal attachments.
The major distal attachment is through a tendon that connects to the radial tuberosity of the proximal radius.
A second distal attachment to the ulna occurs through the bicipital aponeurosis, a fibrous band of tissue that arises from the main biceps tendon, crosses over the cubital fossa (described later in this chapter), and fuses with the deep fascia of the proximal forearm.
Although the biceps is a muscle in the arm, it has no attachments to the humerus!
Actions of biceps:
Proximally, the biceps can flex the glenohumeral joint, since both its tendons cross the joint.
The biceps flexes the elbow joint powerfully when the forearm is supine (palms facing forward).
When the forearm is pronated (palms facing backwards), the radial tuberosity faces posterior and the biceps tendon is curled around the radius. From this starting position, contraction of the biceps rotates the radius around its long axis and supinates the forearm. To demonstrate this, palpate the biceps while driving a screw with a screwdriver. Do you feel it contract? You bet! The biceps is a weak elbow flexor when the forearm is prone.
Summary of actions: The biceps brachii flexes the glenohumeral joint, supinates the forearm, and flexes the elbow when the forearm is supine.
Whereas biceps is the glamour muscle in the arm, the brachialis is the workhorse. It originates from the shaft of the humerus and inserts distally onto the coronoid process of the ulna. Most of the brachialis is covered by the overlying biceps. It gets no respect! Brachialis however is the most important and powerful flexor of the elbow because it can do so regardless of forearm position—pronated or supinated. Take that, biceps!
Clinical correlation
Pain in the anterior shoulder resulting from trauma or impingement of the tendon of the long head of biceps as it slides through the bicipital groove is known as bicipital tendinopathy. The term bicipital tendinitis is used when there is accompanying tendon inflammation. Whatever the name, this is a common cause of shoulder pain, often due to overuse when the upper limb is repeatedly positioned overhead,as in athletic endeavors or painting a ceiling.
All muscles in the anterior compartment of the arm
are innervated by the musculocutaneous nerve, from the lateral cord of the brachial plexus.
Table 10.1 Muscles in the anterior compartment of the arm
Muscle
Proximal attachment(origin)
Distal attachment (insertion)
Innervation
Primary actions
Coracobrachialis
Coracoid process of scapula
Midshaft of humerus
Musculocutaneous nerve
Flexes and adducts arm; Assists rotator cuff in preventing humeral head dislocation
Biceps brachii
Long head: Supraglenoid tubercle of scapula
Short head: Coracoid process of scapula
Radial tuberosity; Ulna via bicipital aponeurosis and deep fascia
Flexes arm; Supinates forearm;
Flexes forearm when it is supinated
Brachialis
Distal shaft of humerus
Coronoid process of ulna
Flexes forearm
Nerves
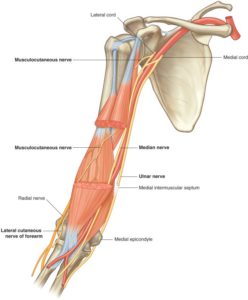
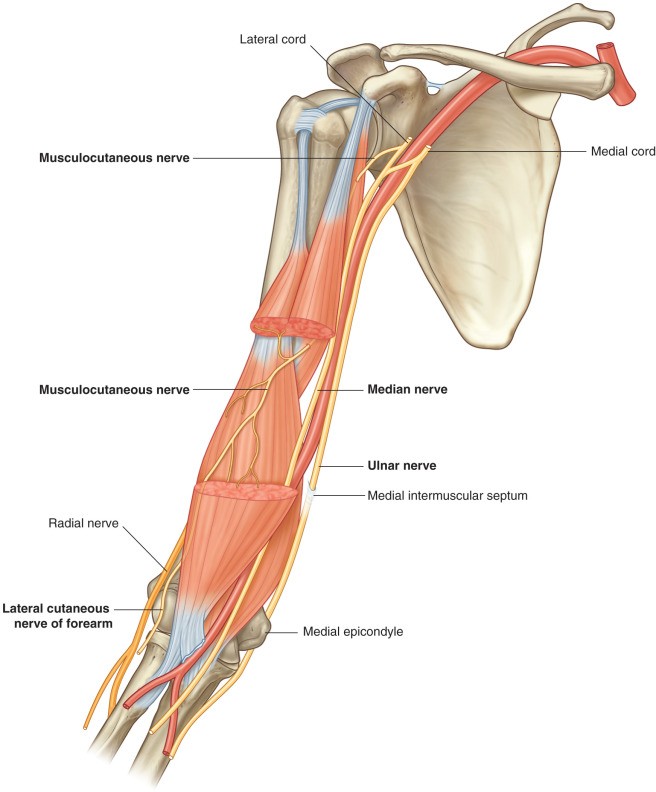
Figure 10.4 Nerves in the anterior compartment of the arm. DRAKE, GRAY’ S ANATOMY FOR STUDENTS, 4TH ED. FIG. 7.68.
The musculocutanous nerve (from the lateral cord of the brachial plexus) penetrates and innervates the coracobrachialis (an important landmark in the dissection laboratory!). Afterwards, it enters the plane between the biceps brachii and brachialis muscles, innervating both. Distally it leaves this plane and enters the superficial fascia of the lateral forearm, becoming the lateral cutaneous nerve of the forearm.
The median and ulnar nerves pass through the anterior compartment on the medial side of the arm in parallel with the brachial artery and veins. Neither functions in the anterior compartment—just passin’ through to get to the forearm.
Cutaneous innervation of the arm:
Skin on the medial side of the arm is supplied by the medial cutaneous nerve of the arm from the medial cord of the brachial plexus. Skin on the lateral side of the arm is supplied by the axillary and radial nerves.
Vessels
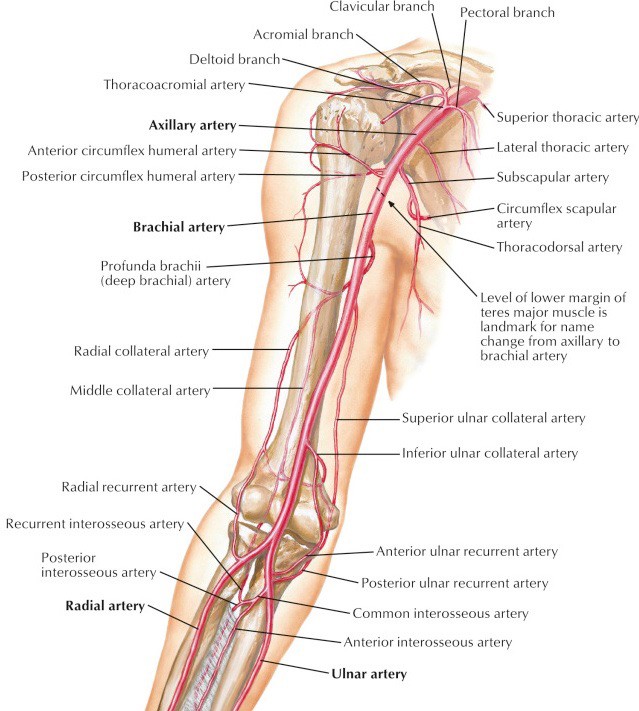
Figure 10.5 Arteries of the arm. NETTER, ATLAS OF HUMAN ANATOMY, 7 TH ED., PLATE 424 .
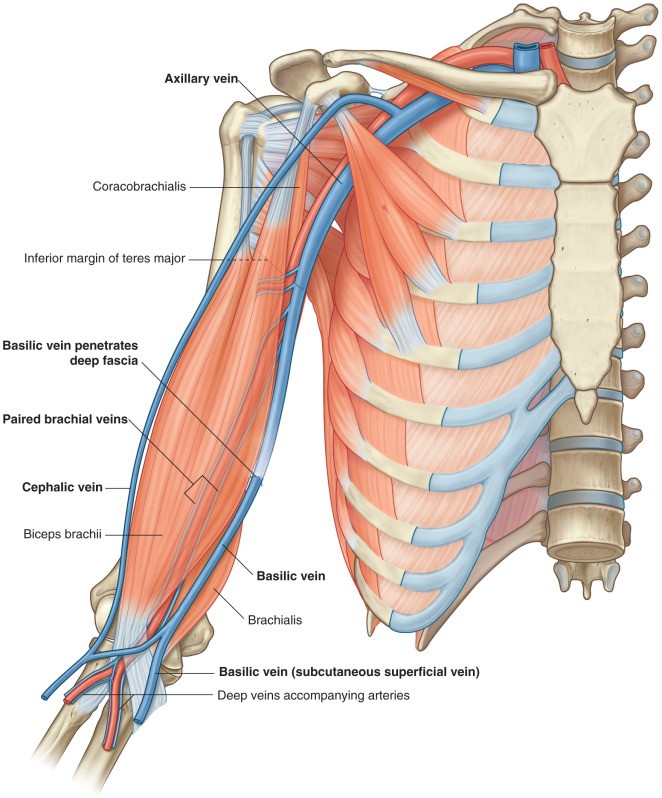
Figure 10.6 Vessels of the arm. DRAKE, GRAY’S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.67.
The brachial artery is the direct continuation of the axillary artery distal to the teres major muscle. It passes down the medial arm on the surface of the brachialis. When it reaches the cubital fossa over the elbow it divides into radial and ulnar arteries.
The chief supply of blood to both compartments of the arm is the deep artery of the arm (profunda brachii artery). It branches from the proximal brachial artery and accompanies the radial nerve into the posterior compartment of the arm. Before doing so it provides branches to the muscles in the anterior compartment.
The brachial artery is accompanied by two brachial veins. These arise from the union of the radial and ulnar veins. They collect blood from the deep arm, below the deep fascia. In the upper medial arm, the brachial veins join the basilic vein (a superficial vein) to form the axillary vein.
Superficial veins in the arm (also described in Introduction to the Limbs): These are in the superficial fascia. The basilic vein courses along the medial arm, sandwiched between the median and ulnar nerves. In the upper arm it penetrates the deep fascia and joins the brachial veins to form the axillary vein. The cephalic vein passes upward in the arm on the lateral side of the biceps, where it can be seen in lean individuals below the skin, popping out as the “body builder’s vein.” Above the arm the cephalic vein runs in a groove between the pectoralis major and deltoid muscles, then dives through the deep fascia to flow into the axillary vein.
Supratrochlear lymph nodes (also called epitrochlear). Most lymph from the upper limb drains directly to nodes in the axilla. There are one or two nodes consistently located in the arm just above the medial epicondyle. These are called supratrochlear nodes. They receive lymph from the medial three fingers and medial hand. Finger infections are not uncommon, and they may produce red streaks on the anterior forearm (inflamed lymph vessels) and swollen supratrochlear nodes. Lymph from these nodes does eventually make its way to axillary nodes.
Posterior compartment of arm
Muscle
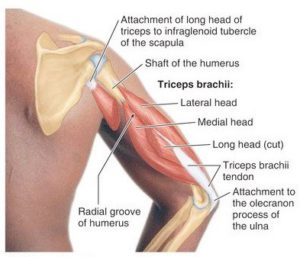
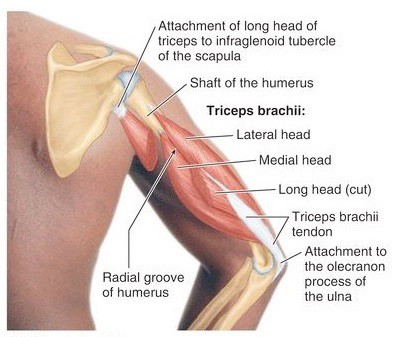
Figure 10.7 MOORE ET AL., CLINICALLY ORIENTED ANATOMY, 8TH ED., FIG. 3.49.
There is only one muscle in the posterior compartment: the triceps brachii. Can you guess why it received this name? You got it: three heads = long, lateral, and medial. The triceps therefore has three proximal attachments (origins).
Attachments:
The long head of triceps originates via a tendon from the infraglenoid tubercle of the scapula, outside of the glenohumeral joint. As it passes downward along the medial side of the arm, it separates the quadrangular space (on the tendon’s lateral side) from the triangular space (medial side of the tendon).
The lateral head of triceps originates from the posterior humeral shaft above the radial groove. This head is prominently displayed in bodybuilder poses. Practice this at home in the mirror!
The medial head of triceps originates from the posterior humeral shaft below the radial groove. Its attachment to the posterior humerus is essentially the mirror image of the brachialis in the anterior compartment. Like the brachialis, the medial head of the triceps is the “workhorse,” always active in extending the forearm at the elbow joint.
The three heads of the triceps fuse in the distal arm to form a tendon that inserts into the olecranon of the ulna.
Actions of triceps:
The long head is the only part of the triceps that crosses the glenohumeral joint. It can assist other muscles in extending and adducting the arm at this joint. In this capacity, the long head helps the rotator cuff resist dislocation of the humeral head.
The main action of triceps is extension of the forearm at the elbow. The medial head is always active in this role; the long and lateral heads are recruited when extending the elbow against resistance.
Table 10.2 Muscles in the posterior compartment of the arm
Muscle
Proximal attachment (origin)
Distal attachment (insertion)
Innervation
Primary actions
Triceps brachii
LONG HEAD: Infraglenoid tubercle of scapula
LATERAL HEAD: Shaft of humerus above radial groove
MEDIAL HEAD: Shaft of humerus below radial groove
Olecranon of ulna
Radial nerve
Long head extends and adducts arm and assists rotator cuff in preventing humeral head dislocation; All three heads extend forearm at elbow
Nerves
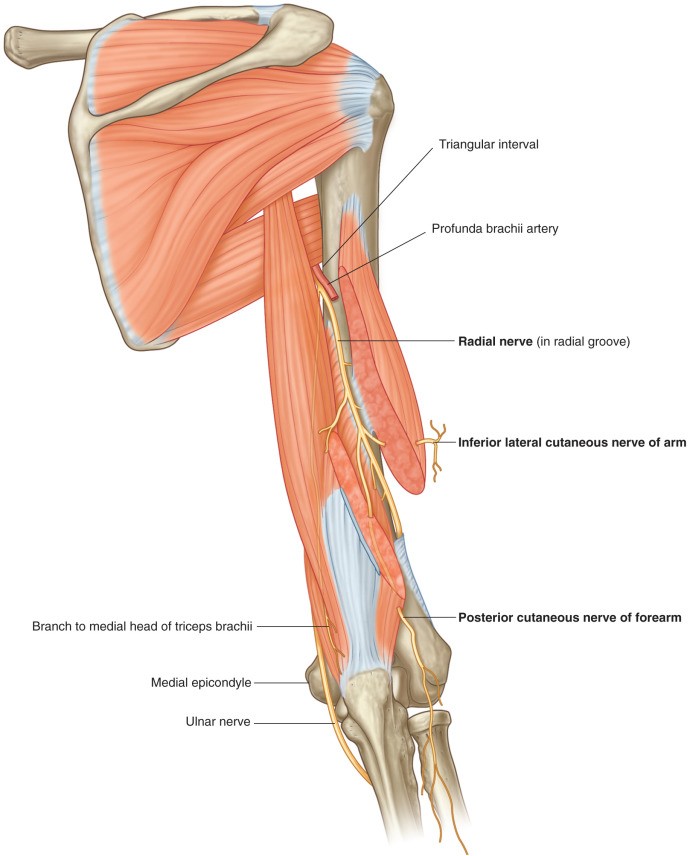
The radial nerve passes from the axilla into the posterior compartment of the arm through the gap between the long and lateral heads of the triceps. It spirals around the shaft of the humerus from medial to lateral in the radial groove, between the origins of the medial and lateral heads of the triceps. On the lateral side of the arm, the radial nerve enters the anterior compartment for a brief time, between the brachialis and brachioradialis muscles. Over the lateral epicondyle of the humerus, the radial nerve splits into deep and superficial branches.
The radial nerve innervates the triceps—in fact, it innervates all muscles in the posterior compartments of the arm and forearm. These muscles by and large extend the forearm and wrist.
The radial nerve also supplies the skin over the posterior compartment.
Clinical correlation
The radial nerve can be compressed against the humerus where it enters the arm, producing temporary numbness. The classic cause is persistent pressure applied by a firm object to the axilla, either by the use of crutches, or falling asleep with an arm slung over the back of a chair (perhaps after a night celebrating the passing of an anatomy exam!). The latter case is known as “Saturday-night” palsy.
Because it lies adjacent to the humerus in the radial groove, the radial nerve is vulnerable to injury should a midshaft fracture of the humerus occur.
These are caused by direct trauma to the arm and account for about 3% of all fractures (NCBI). They are more likely to occur in young men and older women. A midshaft fracture could cause radial nerve palsy and lead to wrist drop = inability to extend the wrist due to denervation of muscles in the posterior forearm. The triceps is usually spared from paralysis (elbow extension intact or weakened) since most of the motor fibers to the triceps are given off from the radial nerve proximal to the radial groove.
Vessels
The deep artery of the arm (profunda brachii artery), a branch of the brachial artery, accompanies the radial nerve into the posterior arm. This artery is the major source of blood to both compartments of the arm.
Figure 10.8 Radial nerve in the posterior arm. DRAKE, GRAY’ S ANATOMY FOR STUDENTS, 4TH ED., FIG. 7.69.
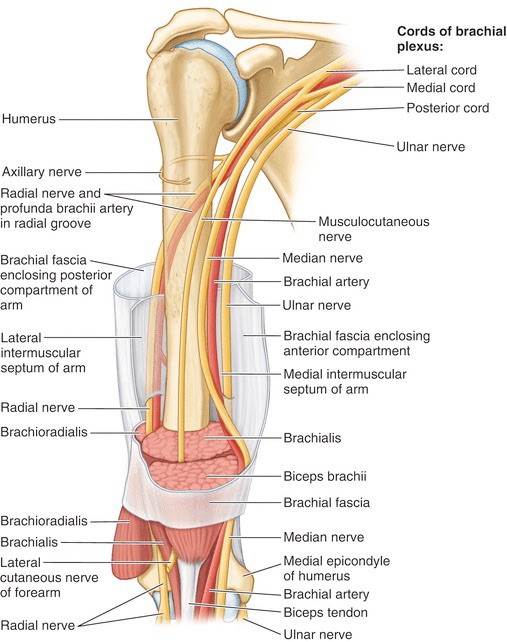
Figure 10.9 Summary of nerves and vessels of the arm. MOORE ET AL., CLINICALLY ORIENTED ANATOMY, 8TH ED., FIG. 3.53.