Clinically Oriented Anatomy, 8th ed., Overview of Thorax section through The bottom line: Muscles and neurovasculature of thoracic wall.
Goals
Identify the boundaries and contents of the axilla.
Learn the architecture of the brachial plexus.
Identify the muscles, nerves, and vessels of the arm.
The walls surrounding the thoracic cavity are made from layers of muscles and fascia that are reinforced by the thoracic skeleton (“rib cage”). The thoracic wall is cone- shaped; narrower above and wider below. The bones and bulky muscles of the pectoral region, which are properly part of the upper limb, overlie and obscure the relatively small thoracic skeleton, made of ribs, costal cartilages, sternum, and thoracic vertebrae. The spaces between the ribs (intercostal spaces) are filled with muscles, nerves, and vessels. The thoracic wall is flexible and compressible, yet rigid enough to support the upper limb and resist pressures generated within the thoracic cavity.
Gut tube (= inner tube) and its derivatives = air tubes of lungs, liver, gall bladder, and pancreas
From splanchnic mesoderm and endoderm
“Visceral” type of innervation from autonomic nervous system
Pain from these organs is often referred to somatic body parts.
Body wall (= outer tube)
From somatic mesoderm and ectoderm
“Somatic” type of innervation from peripheral nerves
Pain from these areas is usually sharp and well-localized.
An organ consisting of an outer layer called the epidermis and a tough connective tissue layer beneath it called the dermis.
The skeletal elements underlying the thoracic body wall consisting of ribs, costal cartilages, the sternum, and thoracic vertebrae.
Paravertebral muscles: As the name implies, these are located adjacent to the vertebral column in the back. We won’t be discussing them much in this course, but you should be aware of them, as they form an easily palpable longitudinal mass alongside the vertebral column.
Body wall muscles: Three layers in both thoracic and abdominal regions:
External layer
Internal layer
Innermost layer
Tying it all together with Acland
Additional detailed videos
3.2.4 Review of bones of the thorax.
3.2.1 The bones of the thorax.
3.2.3 First rib and clavicle.
3.2.2 Costovertebral joints. (The ligaments can be skipped.)
3.2.7 Muscles of inspiration. (Just external intercostals; actions are in chapter 7.)
3.2.8 Muscles of expiration. (Just internal intercostals; actions are covered in chapter 7.)
3.2.14 Nerves of the thorax. (Intercostal nerves section only, which is only a few seconds long.)
Anatomy is a visual science.
The best way to learn it is to be able to recall it visually and be able to describe it based on what you see in your “mind’s eye.”
Sketch! Sketch! Sketch!
Do little sketches, flow-charts, or even stick-drawings.
Protection of the spinal cord and spinal nerves
Supports the head and trunk
Transmits the weight of the trunk to the lower limbs via the pelvic skeleton
Provides attachments for postural muscles and limb muscles
Provides both a rigid and flexible axis for the body
Provides a pivot point for the head
Bulbs of the vestibule
The bulbs are elongated masses of erectile tissue located on either side of the vestibule, deep to the labia minora. They are covered by the bulbospongiosus muscles.
Greater vestibular glands (Bartholin's glands)
Oval masses about the size of a pea located posterior and deep to the vestibular bulbs. Their ducts open into the vestibule. Engorgement of the vestibular bulbs compresses the glands, causing them to secrete fluid that lubricates the vestibule and vaginal orifice.
If the vaginal orifice is viewed as a clock face, the greater vestibular glands are at 4 and 8 o’clock.
Pulmonary
Ophthalmic
Neurologic
Heme-Onc
Digestive
Dermatologic
Renal
Cardiac
Endocrine/Metabolic
Rheumatologic and Musculoskeletal
checkbox
checkbox text
item
item
item
Draw on me/interactive
(Tap to open; use your Apple Pencil to draw.)
Clinical correlation: extra info
text
Clinical correlation
text
Clinical correlation
Neural tube defects (NTDs) are congenital anomalies of the central nervous system that result from defective closure of the neural tube during the fourth week.
Because the neural tube fails to close, or is slow to close, NTDs mayalso influence the tissues surrounding the CNS: meninges,skull, vertebral arches,muscles, and skin. Folic acid deficiency has been linked to NTDs, so pregnant women (and those thinking about becoming pregnant) are advised to take vitamins containing folic acid.
Figure 2.19 LARSEN’ S HUMAN EMBRYOLOGY, 5TH ED., FIG. 4-13. See also Figure 2.20.
A note about this session
text
Because the neural tube fails to close, or is slow to close, NTDs mayalso influence the tissues surrounding the CNS: meninges,skull, vertebral arches,muscles, and skin. Folic acid deficiency has been linked to NTDs, so pregnant women (and those thinking about becoming pregnant) are advised to take vitamins containing folic acid.
Figure 2.19 LARSEN’ S HUMAN EMBRYOLOGY, 5TH ED., FIG. 4-13. See also Figure 2.20.
Question
question text
Because the neural tube fails to close, or is slow to close, NTDs mayalso influence the tissues surrounding the CNS: meninges,skull, vertebral arches,muscles, and skin. Folic acid deficiency has been linked to NTDs, so pregnant women (and those thinking about becoming pregnant) are advised to take vitamins containing folic acid.
Figure 2.19 LARSEN’ S HUMAN EMBRYOLOGY, 5TH ED., FIG. 4-13. See also Figure 2.20.
interactive
Embryonic and extraembryonic structures of Week 2. Can you identify these? (tap to open; use your Apple Pencil to draw and make notes)
HAND-DRAWN CONLEY- GRAM.
1
The outer layer is the visceral layer of serous pericardium or the epicardium, a serous membrane. It contains a variable amount of fatty tissue deep to the mesothelium.
2
The thickest portion of the heart is the middle layer, the myocardium. This layer consists of cardiac muscle tissue.
3
The smooth, inner layer of the heart is the endocardium. It is continuous with the endothelium, the simple squamous epithelium lining the blood vessels that enter and leave the heart.
A period of three calendar months. Clinicians divide the gestation period into three trimesters. The most dramatic and critical stages of development occur during the 1st trimester.
Using the estimated day of fertilization as the reference point. Gestation lasts 38 weeks. In our discussions, we will use fertilization age when describing development.
The first eight weeks of development. This is a busy time with the most striking advances in development. All of the body’s organ systems have formed by the end of the embryonic period. This period is of most interest to us as we study gross anatomy.
Fetus is the term used to describe the developing human after the completion of the embryonic period. The fetal period therefore is between the ninth week and birth.
A period of three calendar months. Clinicians divide the gestation period into three trimesters. The most dramatic and critical stages of development occur during the 1st trimester.
Using the estimated day of fertilization as the reference point. Gestation lasts 38 weeks. In our discussions, we will use fertilization age when describing development.
The first eight weeks of development. This is a busy time with the most striking advances in development. All of the body’s organ systems have formed by the end of the embryonic period. This period is of most interest to us as we study gross anatomy.
Fetus is the term used to describe the developing human after the completion of the embryonic period. The fetal period therefore is between the ninth week and birth.
A period of three calendar months. Clinicians divide the gestation period into three trimesters. The most dramatic and critical stages of development occur during the 1st trimester.
Using the estimated day of fertilization as the reference point. Gestation lasts 38 weeks. In our discussions, we will use fertilization age when describing development.
The first eight weeks of development. This is a busy time with the most striking advances in development. All of the body’s organ systems have formed by the end of the embryonic period. This period is of most interest to us as we study gross anatomy.
Fetus is the term used to describe the developing human after the completion of the embryonic period. The fetal period therefore is between the ninth week and birth.
The cardia is the region that receives the esophagus. The sharp indentation above this junction is the cardiac notch.
The fundus is the rounded part that rises above the cardiac notch. It is in contact with the diaphragm.
Below the level of the cardiac notch, the fundus is continuous with the body of the stomach—the largest part of the organ.
The pyloric part is the distal portion that connects to the duodenum. It has several named subparts. The most distal segment is known simply as the pylorus—it contains a thick ring of smooth muscle called the pyloric sphincter. This regulates the amount and consistency of chyme that is passed on to the duodenum from the stomach.
An empty stomach has flattened anterior and posterior surfaces, separated by two curvatures. On the right side is the lesser curvature, connecting to the right side of the esophagus and superior border of the duodenum. An indentation in the lesser curvature, the angular incisure, indicates the junction of the body and pyloric part. The greater curvature begins above at the cardiac notch, curves to the left, and ends below and on the right where it merges with the inferior border of the duodenum.
Figure15.9. GRANT’S ATLAS OF ANATOMY, 14TH ED., FIGURE 4.32.
The stomach is located mainly in the left upper quadrant of the abdomen under cover of the rib cage and behind the left lobe of the liver.
The fundus is separated from the left pleural cavity by the diaphragm. A prominent air bubble in a patient’s fundus is often seen superimposed on the left dome of the diaphragm in a chest X-ray.
The spleen is behind the fundus and greater curvature.
The anterior and posterior surfaces are covered with peritoneum. The lesser omentum attaches to the lesser curvature while the greater omentum (gastrocolic and gastrosplenic ligaments) hangs from the greater curvature. The posterior surface of the stomach faces into the lesser sac.
The classic cartoon of the stomach portrays it as J-shaped—its shape, however, can vary. The only two fixed parts of the stomach are the cardia and pylorus. In between these, a normal stomach’s contour depends on age, size of surrounding organs, and body type (habitus) of the individual. Stout individuals with a shorter thorax tend to have higher, more horizontal stomachs (“steer horn” stomach—do you see why?), while those with slender builds have lower, more vertical stomach shapes (See Anatomical classification of the shape and topography of the stomach). Congenital anomalies and pathologic conditions that affect nerve and muscle tone can also alter the shape.
In an empty stomach, the mucosa is raised up into sinuous ridges called gastric folds (gastric rugae). Gastric folds smooth out and become obliterated as the stomach fills and becomes distended.
Via extensive anastomoses between branches of the celiac trunk. The left and right gastric arteries anastomose along the left curvature. Left and right gastro-omental arteries join along the greater curvature. Short gastric arteries branch from the splenic artery and supply the fundus.
Left and right gastric veins are tributaries of the portal vein. The left gastro-omental vein drains to the splenic vein. The right gastro-omental vein usually empties into the superior mesenteric vein. Ultimately all venous blood enters the portal vein.
Lymphatic drainage of the stomach follows the general plan laid out in the Overview of GI tract vessels, lymphatics, and nerves: Two sets of nodes filter the lymph = peripheral nodes near the organ receive lymph first, then central nodes near the aorta. Peripheral nodes are situated near the wall of the stomach along the lesser and greater curvatures. Efferent lymph vessels from these nodes transmit the lymph to celiac nodes along the aorta. Celiac nodes drain to intestinal lymph trunks, which merge with the cisterna chyli.
Figure 15.10. GRANT’S ATLAS OF ANATOMY, 14TH ED., FIGURE 4.32.
Innervation: nerve fibers reachthe stomach via the celiac plexus
Parasympathetic—branches ofanterior and posterior vagal trunks
Sympathetic—via greatersplanchnic nerves that relay on celiac ganglia
Visceral afferent fibers transmitting pain travel in greater splanchnic nerves—cellbodies are in T-6 to T-9 dorsal root ganglia (where is pain from the stomach referred to?)
The empty bladder (rarely the case in the living body) is shaped like an inverted pyramid, and its anatomic parts are described in its empty state. The actual position and shape of the bladder vary according to the amount of urine it contains and the age of the person.
Superior surface (dome of the bladder) is covered by peritoneum. The other surfaces of the bladder are subperitoneal.
Posterior surface is called the base or fundus of the bladder.
Apex of bladder: Connects the bladder to the anterior abdominal wall via a fibrous cord called the median umbilical ligament (urachus).
Neck of bladder: Points inferior. This is where urine leaves the bladder and enters the urethra. In the male, the neck rests on the prostate and is fused to it.
Figure 20.3 NETTER, ATLAS OF HUMAN ANATOMY, PLATE 313.
The mucosa of the empty bladder is folded and loose, except in an area at the base called the trigone, where it is smooth and firmly tacked down to the underlying muscle.
The trigone is defined by three orifices = two internal ureteric orifices and the internal urethral orifice. The trigone is at the base of the bladder.
The trigone may be elevated in males = this is called the uvula of the bladder. It can become quite prominent in older males when the underlying prostate enlarges.
The smooth muscle in the bladder wall is called the detrusor (Latin = “to drive away”). It contracts to squeeze out the urine. The detrusor is the juicer!In the neck, smooth muscle forms the involuntary internal urethral sphincter.
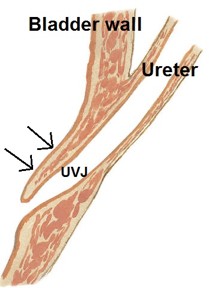
Ureterovesical junction (UVJ): The ureters pass through the wall of the bladder at an oblique angle. This is the intramural part of the ureter. As the bladder fills and distends, the intramural part closes to prevent backflow of urine from bladder into ureter. This valve mechanism doesn’t work so well in children because the intramural part of the ureter is short and there is not enough bladder musculature. Reflux of urine is a common cause of urinary tract infections in kids.
A rest-and-digest function, regulated by parasympathetic innervation. It is under voluntary control but may occur asa reflex involving the micturition center in the brainstem, as in children not “toilet-trained” or when one has an intense fight-fright-flight emergency response.
As the bladder fills, stretch receptors communicate fullness to the brain, causing reflex contraction of the detrusor muscle and relaxation of the internal urethral sphincter.
This reflex can be overcome by contraction of the voluntary external urethral sphincter in the deep perineal pouch (if you are toilet trained!), preventing flow of urine in the urethra.
Conscious relaxation of the pelvic diaphragm and external urethral sphincter allows urine to flow. When you can’t relax (as in a crowded public restroom), tense muscles and sympathetic closure of the internal urethral sphincter results in an unfortunate inability to micturate.
This site has a nice description of neural control of micturation.
Superior rectal artery (from inferior mesenteric) and middle rectal artery (from internal iliac).
Venous drainage: A submucosal rectal venous plexus drains to the superior rectal vein (portal drainage) and middle rectalveins (systemic drainage = IVC).
Sympathetic: From upper lumbar segments of spinal cord to pelvic plexus via the hypogastric nerves—this is vasomotor,but may also relax smooth muscle to inhibit peristalsis and constrict the internal anal sphincter.
Parasympathetic: From pelvic splanchnic nerves—stimulates peristalsis; relaxes internal anal sphincter.
Afferent: Carry information concerning stretch and fullness to the sacral spinal cord via pelvic splanchnic nerves. Most of the rectum is below the pelvic pain line, so pain is referred to sacral dermatomes and is poorly localized in the pelvic region.
The rectum fills slowly during the day, the feces being delivered by peristalsis in the descending and sigmoid colons.
The urge to defecate is initiated by mucosal receptors in the ampulla. This induces the relaxation of the internal anal sphincter (smooth muscle) and increases rectal peristalsis.
Reflex stimulation of the external anal sphincter (skeletal muscle) resists the pressure produced by peristalsis—maintaining fecal continence.
Relaxation of the voluntary sphincter and puborectalis muscle and initiation of the Valsalva maneuver (“bearing down”) with continued peristaltic activity empties the rectum.
Figure 20.24 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.47.
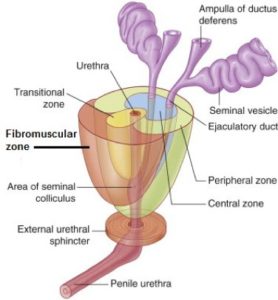
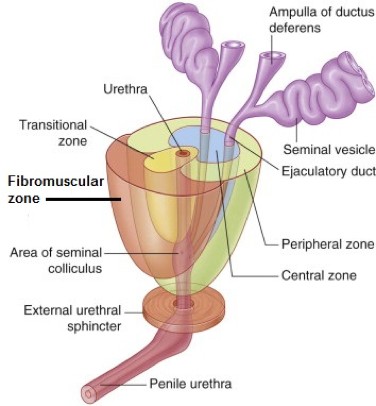
This can be confusing, since anatomists and urologists use different terms, and they are often mixed and matched. The passage of the urethra and ejaculatory ducts through the prostate divides it into anatomic lobes and clinical zones.
Anterior lobe (isthmus) is anterior to the urethra—also known as the fibromuscular zone. There is no glandular tissue here.
Left and right lobes are lateral to the urethra and meet posteriorly in a shallow groove. These lobes together constitute the peripheral zone, the posterior portion of which is palpated in a rectal exam. This zone is the most common location of prostate cancer.
Median lobe is the tissue surrounding the ejaculatory ducts. Also called the central zone.
The transitional zone is sandwiched between the three zones just described. It encircles the urethra in the core of the prostate, below the bladder. This is the region affected by benign hyperplasia.
Figure 20.14 GRAY’S ANATOMY FOR STUDENTS, FIGURE 5.54.
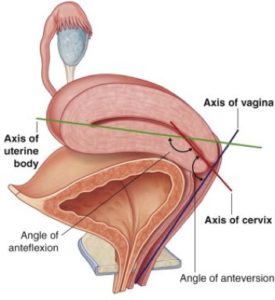
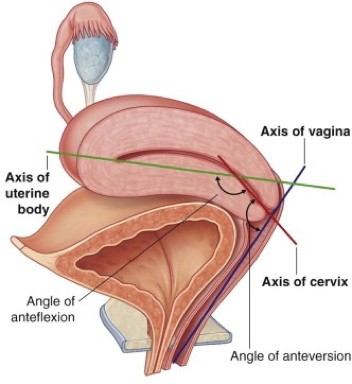
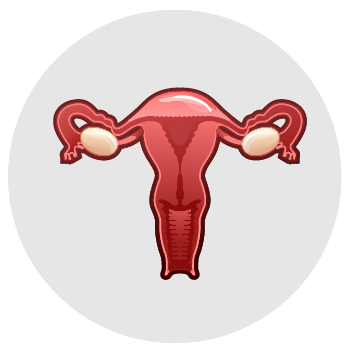
The typical orientation of the uterus is described as anteflexed and anteverted. Flexion refers to orientation of the uterine body with respect to the uterine cervix. Version refers to the orientation of the entire uterus compared to the vagina.
When anteflexed, the body of the uterus is bent anteriorly upon the cervix.
When anteverted, the entire uterus is tilted forward on the vaginal canal—the uterus and vagina thus have a profile shaped like the number “7” in a lateral view.
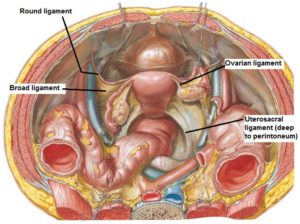
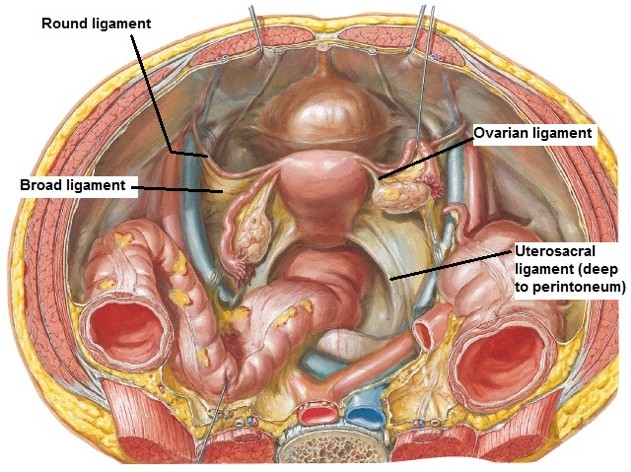
Parametrium: Outermost, composed of visceral pelvic fascia.
Myometrium: Middle layer, thick smooth muscle, branches of the uterine vessels are in this layer.
Endometrium: Inner layer, mucous membrane with uterine glands.Undergoes monthly renewal and degeneration—being cyclically prepared by hormones for implantation of the embryo.
An example: Scenario is a 20 yo F with acute appendicitis. By the CT scan, it is early (not ruptured) and is intraperitoneal.
“Miss X, my name is ____, and I’m the intern on the surgery service. I’d like to take a few minutes to talk with you about this consent form I have here. From the CT scan, my team sees that the cause of your discomfort is most likely due to your appendix. It’s an organ on the right side of your colon (large intestine) that commonly causes problems like this. Fortunately, it’s an organ we can live without. In your case, it is inflamed, but thanks to your awareness and your efficiency getting here, we’ve been able to catch it so early that it hasn’t ruptured.
We believe that the best thing to do is a small surgery to remove the appendix. That surgery is called a "laparoscopic appendectomy." I know surgery may sound scary and risky, but I want to reassure you that this particular surgery is very straightforward. It takes us around 30 minutes. What we propose to do is insert a camera and small instruments into the abdomen to view the appendix, then isolate it and divide it. We put it in a bag to remove it out of your belly button incision and send it to pathology for them to look at it under a microscope.
One alternative is that you opt not to have surgery. In that case, we’d treat you with antibiotics alone: some we’d give in the hospital—like what you’re getting now through your IV—plus a two-week course at home. The team recommends surgery because in 20–30% of cases, those treated with antibiotics will recur within the year and need emergency surgery. But it’s definitely your choice and your preference.
The benefits of surgery is that you’re here already, and it’s a definitive solution to your condition. There are risks with surgery, including bleeding, infection, and damage to surrounding structures. We do everything we can to keep those risks to a minimum.
I realize was a lot of information, and although I went through it quickly, I have lots of time to explain anything you wish in more detail. What questions do you have?
Purely sensory
I II VIII
Mainly motor
III IV VI XI XII
Mixed
V VII IX X
Functions
Olfaction (smell)—special sensory
Skull opening
Olfactory (cribriform) foramina.
Attachments to CNS
Nucleus of origin/destination in CNS
Bipolar neurons of olfactory nerves synapse on secondary olfactory neurons in olfactory bulbs.
Details
Thought question If the vermis of the cerebellum were affected, what type of signs could a child exhibit?
Review
A pediatric patient has a neuroblastoma associated with the adrenal medulla. This tumor could be related to a pathological disturbance of which of these embryonic structures?
A 75-year-old gentleman. Felipe Moreno, is brought in by his family because of a 6-month history of progressive difficulty with walking and balance and a 4-month history of urinary incontinence. Further inquiry reveals that, while he was once gregarious and busy with any one of dozens of projects, he now spends his days quietly sitting alone, staring into space.
On a neurologic exam, Felipe generally answers appropriately when asked a question, but only with single words or short sentences without elaboration. If given several tasks in sequence, he will at best complete one of them (motor impersistence). For example, if asked to write a note, fold the paper, put it in an envelope, and seal it, he may simply write one word on the paper.
Felipe cannot rise to a standing position without assistance. As he attempts to walk, his feet appear to be glued to the floor (magnetic gait). Eventually he is able to make wide-based steps, and he also has stiffness and is unable to pivot properly.
A ventriculoperitoneal shunt was placed, and Felipe's gait and urinary incontinence improved markedly, but he still had lingering significant cognitive impairment.
Describe some possible causes of NPH in this patient.
Pituitary
Thyroid and parathyroid glands
Adrenals
Pancreatic islets
Testes
Ovaries
Salivary glands: Secrete saliva into the oral cavity.
Liver
Gall bladder: Stores bile. Connected to the liver and duodenum by bile ducts.
Pancreas: Has both exocrine and endocrine functions. Snuggled up within the concavity (“C”) of the duodenum and connected to it by one (or two) pancreatic duct(s).
The retroperitoneum and kidneys (posterior abdominal wall)
Know this!
Different parts of the urinary tract come from different embryologic sources:
Nephrons
The excretory units of the kidneys (from intermediate mesoderm)
Collecting system
Collecting ducts through ureters (from mesonephric duct)
Urinary bladder and urethra
(From primitive urogenital sinus)
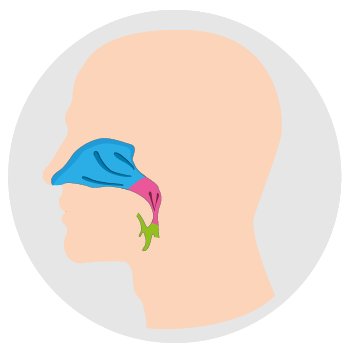
When it is removed (laryngectomy) because of laryngeal cancer, the trachea can be connected to an opening in the anterior neck (tracheostomy).
Origin
Temporalis arises from the bony floor of the fossa and from the deep surface of the stout temporal fascia, which covers the muscle externally. The temporal fascia attaches above to the superior temporal line and below to the zygomatic arch. The scalp is external to the fascia.
Insertion
The muscle fibers are arranged like a fan. They converge below on a tendon that attaches to the coronoid process of the mandible.
Actions
Temporalis is a chewing muscle. Its vertical fibers elevate the mandible to close the jaw. The horizontal fibers retract the mandible after it has been protruded.
Boundaries
The pelvic diaphragm is the ceiling separating the perineum from the pelvic cavity. Inferiorly the perineum presents a free surface covered with skin and the external genitalia. The other boundaries of the perineum are those of the pelvic outlet:
Subdivisions
A line drawn between the two ischial tuberosities divides the perineum into two triangles: Urogenital (UG) triangle and anal triangle.
contents
Mainly a large adipose body. This is semi-liquid at body temperature, allowing the anal canal to expand when feces are passed.
Pudendal canal (Alcock’s canal): Formed by a layer of obturator fascia that rolls-up in a tube in the lateral wall of the ischio-anal fossa. This provides a tunnel through the adipose body for the passage of the internal pudendal artery and vein and the pudendal nerve.
The inferior anal (rectal) nerve splits from the pudendal nerve at the entrance (posterior end) of the pudendal canal. It crosses the ischio-anal fossa from lateral to medial, innervating the external anal sphincter, the lower half of the anal canal, and the peri-anal skin.
innervation
All of the above muscles are innervated by the pudendal nerve. The same goes for the male.
Eric, a 55-year-old small business owner who repaints cars and does computer repair, has “slowed down” over the past 2–3 years and speaks in a monotone but demonstrates good insight and humor; he “shuffles” into the room. His paperwork is hard to read because the writing is small.
Unless otherwise noted, images are from Adobe Stock.
1. Skin
2. Connective tissue
Binds skin to the epicranial aponeurosis, ensheaths most of the blood vessels, and contains the nerves supplying the scalp.
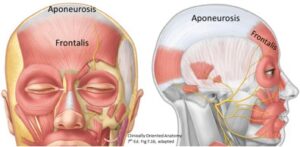
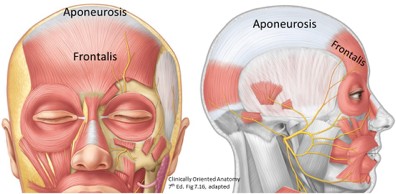
3. Aponeurosis
Epicranial aponeurosis: 2 flat skeletal muscles attached to its anterior and posterior ends (the frontal and occipital parts of the occipitofrontalis muscle) move the scalp forward and backward. These muscles are innervated by the facial nerve (cranial nerve VII).
Figure 2.
Aponeurosis: When it is cut, the occipitofrontalis holds the wound open so lacerated arteries can’t retract. This is one of the reasons that scalp wounds bleed profusely. Superficial lacerations that do not extend to the aponeurosis are easily closed.
4. Loose connective tissue
Creates a potential space that allows movement of the scalp proper on the calvaria, and also can fill with fluid from injury or infection.
5. Pericranium (external layer of periosteum)
Innervation: Pre-G PARA in CN III ciliary ganglion Post-G parasympathetic fibers in short ciliary nerves